Cyproterone acetate
Cyproterone acetate (CPA), sold alone under the brand name Androcur or with ethinylestradiol under the brand names Diane or Diane-35 among others, is an antiandrogen and progestin medication which is used in the treatment of androgen-dependent conditions like acne, excessive hair growth, early puberty, and prostate cancer, as a component of feminizing hormone therapy for transgender women, and in birth control pills.[1][11][13][14][15] It is formulated and used both alone and in combination with an estrogen and is available for use both by mouth and by injection into muscle. CPA is taken by mouth one to three times per day or given by injection once or twice per week.
 | |
 | |
| Clinical data | |
|---|---|
| Trade names | Androcur, Androcur Depot, Cyprostat, Siterone, others |
| Other names | SH-80714; SH-714; NSC-81430; 1α,2α-Methylene-6-chloro-17α-hydroxy-δ6-progesterone acetate; 1α,2α-Methylene-6-chloro-17α-hydroxypregna-4,6-diene-3,20-dione acetate |
| AHFS/Drugs.com | Micromedex Detailed Consumer Information |
| Pregnancy category |
|
| Routes of administration | By mouth, intramuscular injection |
| Drug class | Steroidal antiandrogen; Progestogen; Progestin; Progestogen ester; Antigonadotropin |
| ATC code | |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | Oral: 68–100%[1][2] |
| Protein binding | Albumin: 93% Free: 7%[3][4][5][6] |
| Metabolism | Hepatic (CYP3A4)[7][8] |
| Metabolites | • 15β-OH-CPA (major)[1][9] • Cyproterone (minor)[10] • Acetic acid (minor)[10] |
| Elimination half-life | Oral: 1.6–4.3 days[10][11][12] IM: 3–4.3 days[2][10][12] |
| Excretion | Feces: 70%[10] Urine: 30%[10] |
| Identifiers | |
| |
| CAS Number |
|
| PubChem CID | |
| IUPHAR/BPS | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| CompTox Dashboard (EPA) | |
| ECHA InfoCard | 100.006.409 |
| Chemical and physical data | |
| Formula | C24H29ClO4 |
| Molar mass | 416.94 g·mol−1 |
| 3D model (JSmol) | |
| Melting point | 200 to 201 °C (392 to 394 °F) |
| |
| |
| (verify) | |
Common side effects of high-dose CPA in men include gynecomastia (breast development) and feminization. In both men and women, possible side effects of CPA include low sex hormone levels, reversible infertility, sexual dysfunction, fatigue, depression, weight gain, and elevated liver enzymes. At very high doses in older individuals, significant cardiovascular complications can occur. Rare but serious adverse reactions of CPA include blood clots, liver damage, and certain types of benign brain tumors. CPA can also cause adrenal insufficiency as a withdrawal effect if it is discontinued abruptly from a high dosage. CPA blocks the effects of androgens like testosterone in the body, which it does by preventing them from interacting with their biological target, the androgen receptor (AR), and by reducing their production by the gonads and hence their concentrations in the body.[1][13][16] In addition, it has progesterone-like effects by activating the progesterone receptor (PR).[1][13] It can also produce weak cortisol-like effects at very high doses.[1]
CPA was discovered in 1961.[17] It was originally developed as a progestin.[17] In 1965, the antiandrogenic effects of CPA were discovered.[18] CPA was first marketed, as an antiandrogen, in 1973, and was the first antiandrogen to be introduced for medical use.[19] A few years later, in 1978, CPA was introduced as a progestin in a birth control pill.[20] It has been described as a "first-generation" progestin.[21] CPA is available widely throughout the world.[22][23] An exception is the United States, where it is not approved for use.[24] CPA has been described as the prototypical antiandrogen.[25]
Medical uses
CPA is used as a progestin and antiandrogen in hormonal birth control and in the treatment of androgen-dependent conditions.[13] Specifically, CPA is used in combined birth control pills, in the treatment of androgen-dependent skin and hair conditions such as acne, seborrhea, excessive hair growth, and scalp hair loss, high androgen levels, in transgender hormone therapy, to treat prostate cancer, to reduce sex drive in sex offenders or men with paraphilias or hypersexuality, to treat early puberty, and for other uses.[26] It is used both at low doses and at higher doses.
In the United States, where CPA is not available, other medications with antiandrogenic effects are used to treat androgen-dependent conditions instead.[27] Examples of such medications include gonadotropin-releasing hormone modulators (GnRH modulators) like leuprorelin and degarelix, nonsteroidal antiandrogens like flutamide and bicalutamide, the diuretic and steroidal antiandrogen spironolactone, the progestin medroxyprogesterone acetate, and the 5α-reductase inhibitors finasteride and dutasteride.[27] The steroidal antiandrogen and progestin chlormadinone acetate is used as an alternative to CPA in Japan, South Korea, and a few other countries.
Birth control
CPA is used with ethinylestradiol as a combined birth control pill to prevent pregnancy. This birth control combination has been available since 1978.[20] The formulation is taken once daily for 21 days, followed by a 7-day free interval.[28] CPA has also been available in combination with estradiol valerate (brand name Femilar) as a combined birth control pill in Finland since 1993.[29][30] High-dose CPA tablets have a contraceptive effect and can be used as a form of birth control, although they are not specifically licensed as such.[31]
Females
CPA is used as an antiandrogen to treat androgen-dependent skin and hair conditions such as acne, seborrhea, hirsutism (excessive hair growth), scalp hair loss, and hidradenitis suppurativa in women.[32][33][34][35][36][37][38] These conditions are worsened by the presence of androgens, and by suppressing androgen levels and blocking their actions, CPA improves the symptoms of these conditions. CPA is used to treat such conditions both at low doses as a birth control pill and on its own at higher doses.[32][33][34][35][39] A birth control pill containing low-dose CPA in combination with ethinylestradiol to treat acne has been found to result in overall improvement in 75 to 90% of women, with responses approaching 100% improvement.[40] High-dose CPA alone likewise has been found to improve symptoms of acne by 75 to 90% in women.[41] Discontinuation of CPA has been found to result in marked recurrence of symptoms in up to 70% of women.[42] CPA is one of the most commonly used medications in the treatment of hirsutism, hyperandrogenism, and polycystic ovary syndrome in women throughout the world.[43][44]
Higher dosages of CPA are used in combination with an estrogen specifically at doses of 25 to 100 mg/day cyclically in the treatment of hirsutism in women.[44][45][46] The efficacy of such dosages of CPA in the treatment of hirsutism in women appear to be similar to that of spironolactone, flutamide, and finasteride.[45][46][43][44] Randomized controlled trials have found that higher dosages of CPA (e.g., 20 mg/day or 100 mg/day) added cyclically to a birth control pill containing ethinylestradiol and 2 mg/day CPA were no more effective or only marginally more effective in the treatment of severe hirsutism in women than the birth control pill alone.[44][46][43][47][48][49] Maintenance therapy with lower doses of CPA, such as 25 mg/day, has been found to be effective in preventing relapse of symptoms of hirsutism.[42] CPA has typically been combined with ethinylestradiol, but it can alternatively be used in combination with hormone replacement therapy dosages of estradiol instead.[44] CPA at a dosage of 50 mg/day in combination with 100 μg/day transdermal estradiol patches has been found to be effective in the treatment of hirsutism similarly to the combination of CPA with ethinylestradiol.[46][50]
The efficacy of the combination of an estrogen and CPA in the treatment of hirsutism in women appears to be due to marked suppression of total and free androgen levels as well as additional blockade of the androgen receptor.[43][44][51]
Males
CPA has been found to be effective in the treatment of acne in males, with marked improvement in symptoms observed at dosages of 25, 50, and 100 mg/day in different studies.[52][53][54][55] It can also halt further progression of scalp hair loss in men.[56][57][58] Increased head hair and decreased body hair has been observed with CPA in men with scalp hair loss.[59][13] However, its side effects in men, such as demasculinization, gynecomastia, sexual dysfunction, bone density loss, and reversible infertility, make the use of CPA in males impractical in most cases.[56][57][53][54][60][61][62] In addition, lower dosages of CPA, such as 25 mg/day, have been found to be better-tolerated in men.[54] But such doses also show lower effectiveness in the treatment of acne in men.[52]
High androgen levels
CPA is used as an antiandrogen to treat high androgen levels and associated symptoms such as masculinization due to conditions like polycystic ovary syndrome (PCOS) and congenital adrenal hyperplasia (CAH) in women.[33][38][63][64][65][66] It is almost always combined with an estrogen, such as ethinylestradiol, when it is used in the treatment of PCOS in women.[67]
Menopausal hormone therapy
CPA is used at low doses in menopausal hormone therapy in combination with an estrogen to provide endometrial protection and treat menopausal symptoms.[68][1][69][70] It is used in menopausal hormone therapy under the brand name Climen, which is a sequential preparation that contains 2 mg estradiol valerate and 1 mg CPA.[68][69][70] Climen was the first product for use in menopausal hormone therapy containing CPA to be marketed.[69] It is available in more than 40 countries.[68]
Transgender hormone therapy
CPA is widely used as an antiandrogen and progestogen in feminizing hormone therapy for transgender women.[71][72][73][74][75][76][77] It is used orally at a dosage of 10 to 100 mg/day and by intramuscular injection at a dosage of 300 mg once every 4 weeks.[78][79] Studies have found that 10, 25, and 50 mg/day CPA in combination with estrogen all result in equivalent and full testosterone suppression in transgender women.[80][81] In light of risks of CPA such as fatigue, blood clots, benign brain tumors, and liver damage, the use of lower dosages of the medication may help to minimize such risks.[81] The side effects of CPA, such as demasculinization and decreased libido, are more acceptable for transgender women than for (cis) men.[57]
CPA has also been used as a puberty blocker and hence as an antiandrogen and antiestrogen to suppress puberty in transgender youth, although GnRH modulators are primarily used for this purpose.[82][83][73][84][85]
Prostate cancer
CPA is used as an antiandrogen monotherapy and means of androgen deprivation therapy in the palliative treatment of prostate cancer in men.[11][86][87][88][89][90] It is used at very high doses by mouth or by intramuscular injection to treat this disease. Antiandrogens do not cure prostate cancer, but can significantly extend life in men with the disease.[91][92][86] CPA has similar effectiveness to GnRH modulators and surgical castration, high-dose estrogen therapy (e.g., with diethylstilbestrol), and high-dose nonsteroidal antiandrogen monotherapy (e.g., with bicalutamide), but has significantly inferior effectiveness to combined androgen blockade with a GnRH modulator and a nonsteroidal antiandrogen (e.g., with bicalutamide or enzalutamide).[86][92][93][94][95] In addition, the combination of CPA with a GnRH modulator or surgical castration has not been found to improve outcomes relative to a GnRH modulator or surgical castration alone, in contrast to nonsteroidal antiandrogens.[96] Due to its inferior effectiveness, tolerability, and safety, CPA is rarely used in the treatment of prostate cancer today, having largely been superseded by GnRH modulators and nonsteroidal antiandrogens.[97][98] CPA is the only steroidal antiandrogen that continues to be used in the treatment of prostate cancer.[92]
Dose-ranging studies of CPA for prostate cancer were not performed, and the optimal dosage of CPA for the treatment of the condition has not been established.[99][100] A dosage range of oral CPA of 100 to 300 mg/day is used in the treatment of prostate cancer, but generally 150 to 200 mg/day oral CPA is used.[101][102] Schröder (1993, 2009) reviewed the issue of CPA dosage and recommended a dosage of 200 to 300 mg/day for CPA as a monotherapy and a dosage of 100 to 200 mg/day for CPA in combined androgen blockade (that is, CPA in combination with surgical or medical castration).[103][88] However, the combination of CPA with castration for prostate cancer has been found to significantly decrease overall survival compared to castration alone.[104] Hence, the use CPA as the antiandrogen component in combined androgen blockade would appear not to be advisable.[104] When used by intramuscular injection to treat prostate cancer, CPA is used at a dosage of 300 mg once a week.[62]
The combination of CPA with an estrogen such as ethinylestradiol sulfonate or low-dose diethylstilbestrol has been used as a form of combined androgen blockade and as an alternative to the combination of CPA with surgical or medical castration.[103][105][106][107][108]
Sexual deviance
CPA is used as an antiandrogen and form of chemical castration in the treatment of paraphilias and hypersexuality in men.[109][110][111][59][112][113] It is used to treat sex offenders. The medication is approved in more than 20 countries for this indication and is predominantly employed in Canada, Europe, and the Middle East.[114] CPA works by decreasing sex drive and sexual arousal and producing sexual dysfunction. CPA can also be used to reduce sex drive in individuals with inappropriate sexual behaviors, such as people with intellectual disability and dementia.[115][116] The medication is also useful for treating self-harmful sexual behavior, such as masochism.[117] CPA has comparable effectiveness to medroxyprogesterone acetate in suppressing sexual urges and function but appears to be less effective than GnRH modulators like leuprorelin and has more side effects.[110]
High-dose CPA significantly decreases sexual fantasies and sexual activity in 80 to 90% of men with paraphilias.[114] In addition, it has been found to decrease the rate of reoffending in sex offenders from 85% to 6%, with most of the reoffenses being committed by individuals who did not follow their CPA treatment prescription.[114] It has been reported that in 80% of cases, 100 mg/day CPA is adequate to achieve the desired reduction of sexuality, whereas in the remaining 20% of cases, 200 mg/day is sufficient.[118] When only a partial reduction in sexuality is desired, 50 mg/day CPA can be useful.[118] Reduced sexual desire and erectile function occurs with CPA by the end of the first week of treatment, and becomes maximal within three to four weeks.[118][62] The dosage range is 50 to 300 mg/day.[62][118]
Early puberty
CPA is used as an antiandrogen and antiestrogen to treat precocious puberty in boys and girls.[13][64][119] However, it is not fully satisfactory for this indication because it is not able to completely suppress puberty.[120] For this reason, CPA has mostly been superseded by GnRH agonists in the treatment of precocious puberty.[64] CPA is not satisfactory for gonadotropin-independent precocious puberty.[121] CPA has been used at dosages of 50 to 300 mg/m2 to treat precocious puberty.[62][13]
Other uses
CPA is useful in the treatment of hot flashes, for instance due to androgen deprivation therapy for prostate cancer.[93][122][123][124]
CPA is useful for suppressing the testosterone flare at the initiation of GnRH agonist therapy.[125][93][126][11][64][127][128][129][130] It has been used successfully both alone and in combination with estrogens such as diethylstilbestrol for this purpose.[125][131]
Available forms
CPA is available in the form of oral tablets alone (higher-dose; 10 mg, 50 mg, 100 mg) or in combination with ethinylestradiol or estradiol valerate (low-dose; 1 or 2 mg CPA) and in the form of ampoules for intramuscular injection (higher-dose; 100 mg/mL, 300 mg/3 mL; brand name Androcur Depot).[132][133][134][135][136]
The higher-dose formulations are used to treat prostate cancer and certain other androgen-related indications while the low-dose formulations which also have an estrogen are used as combined birth control pills and are used in menopausal hormone therapy for the treatment of menopausal symptoms.[135][137]
Contraindications
Contraindications of CPA include:[138][139][51]
- Hypersensitivity to CPA or any of the other components of the medication
- Pregnancy, lactation, and breastfeeding
- Puberty (except if being used to treat precocious puberty or delay puberty)
- Liver diseases and liver dysfunction
- Chronic kidney disease
- Dubin–Johnson syndrome and Rotor syndrome
- History of jaundice or persistent pruritus during pregnancy
- History of herpes during pregnancy
- Previous or existing liver tumors (only if not due to metastases from prostate cancer)
- Previous or existing meningioma, hyperprolactinemia, or prolactinoma
- Wasting syndromes (except in inoperable prostate cancer)
- Severe depression
- Previous or existing thromboembolic processes, as well as stroke and myocardial infarction
- Severe diabetes with vascular changes
- Sickle-cell anemia
When CPA is used in combination with an estrogen, contraindications for birth control pills should also be considered.[51]
Side effects
CPA is generally well-tolerated and has a mild side-effect profile regardless of dosage when it is used in combination with an estrogen in women.[140][141] Side effects of CPA in general include hypogonadism (low sex-hormone levels) and associated symptoms such as demasculinization, sexual dysfunction, infertility, and osteoporosis (fragile bones); breast changes such as breast tenderness, breast enlargement, and gynecomastia (breasts in men); emotional changes such as fatigue and depression; and other side effects such as vitamin B12 deficiency, weak glucocorticoid effects, and elevated liver enzymes.[51] Weight gain can occur with CPA when it is used at high doses.[142][48] Some of the side effects of CPA can be improved or fully prevented if it is combined with an estrogen to prevent estrogen deficiency.[67][40] Few quantitative data are available on many of the potential side effects of CPA.[143] Pooled tolerability data for CPA is not available in the literature.[144]
At very high doses in aged men with prostate cancer, CPA can cause cardiovascular side effects. Rarely, CPA can produce blood clots, liver toxicity (including hepatitis, liver failure, and liver cancer), excessively high prolactin levels, and certain benign brain tumors including meningiomas (tumors of the meninges) and prolactinomas (prolactin-secreting tumors of the pituitary gland). Upon discontinuation from high doses, CPA can produce adrenal insufficiency as a withdrawal effect.
Overdose
CPA is relatively safe in acute overdose.[139] It is used at very high doses of up to 300 mg/day by mouth and 700 mg per week by intramuscular injection.[139][145] For comparison, the dose of CPA used in birth control pills is 2 mg/day.[146] There have been no deaths associated with CPA overdose.[139] There are no specific antidotes for CPA overdose, and treatment should be symptom-based.[139] Gastric lavage can be used in the event of oral overdose within the last 2 to 3 hours.[139]
Interactions
Inhibitors and inducers of the cytochrome P450 enzyme CYP3A4 may interact with CPA.[139] Examples of strong CYP3A4 inhibitors include ketoconazole, itraconazole, clotrimazole, and ritonavir, while examples of strong CYP3A4 inducers include rifampicin, rifampin, phenytoin, carbamazepine, phenobarbital, and St. John's wort.[139] Certain anticonvulsant medications can substantially reduce levels of CPA, by as much as 8-fold.[35]
Pharmacology
Pharmacodynamics
CPA has antiandrogenic activity,[1][147] progestogenic activity,[1][147] weak partial glucocorticoid activity,[148] weak steroidogenesis inhibitor activity,[149] and agonist activity at the pregnane X receptor.[150][151][152] It has no estrogenic or antimineralocorticoid activity.[1] In terms of potency, CPA is described as a highly potent progestogen, a moderately potent antiandrogen, and a weak glucocorticoid.[51][142][40] Due to its progestogenic activity, CPA has antigonadotropic effects, and is able to suppress fertility and sex-hormone levels in both males and females.[1][13][51]
Pharmacokinetics
CPA can be taken by mouth or by injection into muscle.[13] It has near-complete oral bioavailability, is highly and exclusively bound to albumin in terms of plasma protein binding, is metabolized in the liver by hydroxylation and conjugation, has 15β-hydroxycyproterone acetate (15β-OH-CPA) as a single major active metabolite, has a long elimination half-life of about 2 to 4 days regardless of route of administration, and is excreted in feces primarily and to a lesser extent in urine.[1][4][12]
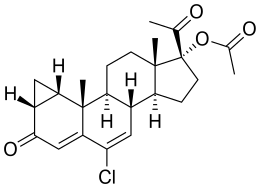
Chemistry
CPA, also known as 1α,2α-methylene-6-chloro-17α-acetoxy-δ6-progesterone or as 1α,2α-methylene-6-chloro-17α-hydroxypregna-4,6-diene-3,20-dione acetate, is a synthetic pregnane steroid and an acetylated derivative of 17α-hydroxyprogesterone.[153][154] It is structurally related to other 17α-hydroxyprogesterone derivatives such as chlormadinone acetate, hydroxyprogesterone caproate, medroxyprogesterone acetate, and megestrol acetate.[154]
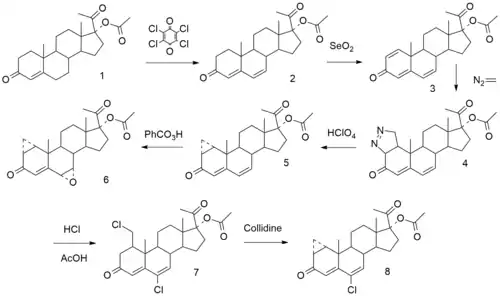
Synthesis
Chemical syntheses of CPA have been published.[133][155][156] The following is one such synthesis:[157][158]
History
CPA was first synthesized in 1961 by Rudolf Wiechert, a Schering employee, and together with Friedmund Neumann in Berlin, they filed for a patent for CPA as "progestational agent" in 1962.[17][159] The antiandrogenic activity of CPA was discovered serendipitously by Hamada, Neumann, and Karl Junkmann in 1963.[160][62] Along with the steroidal antiandrogens benorterone (17α-methyl-B-nortestosterone; SKF-7690), cyproterone, BOMT (Ro 7-2340), and trimethyltrienolone (R-2956) and the nonsteroidal antiandrogens flutamide and DIMP (Ro 7-8117), CPA was one of the first antiandrogens to be discovered and researched.[40][161][162][163]
CPA was initially developed as a progestogen for the prevention of threatened abortion.[62] As part of its development, it was assessed for androgenic activity to ensure that it would not produce teratogenic effects in female fetuses.[62] The drug was administered to pregnant rats and its effects on the rat fetuses were studied.[62] To the surprise of the researchers, all of the rat pups born appeared to be female.[62] After 20 female rat pups in a row had been counted, it was clear that this could not be a chance occurrence.[62] The rat pups were further evaluated and it was found that, in terms of karyotype, about 50% were actually males.[62] The male rat pups had been feminized, and this resultant finding constituted the discovery of the powerful antiandrogenic activity of CPA.[62] A year after patent approval in 1965, Neumann published additional evidence of CPA's antiandrogenic effect in rats; he reported an "organizational effect of CPA on the brain".[18] CPA started being used in animal experiments around the world to investigate how antiandrogens affected fetal sexual differentiation.[164]
The first clinical use of CPA in the treatment of sexual deviance and prostate cancer occurred in 1966.[14][165][166] It was first studied in the treatment of androgen-dependent skin and hair symptoms, specifically acne, hirsutism, seborrhea, and scalp hair loss, in 1969.[167] CPA was first approved for medical use in 1973 in Europe under the brand name Androcur.[155][168] In 1977, a formulation of CPA was introduced for use by intramuscular injection.[169] CPA was first marketed as a birth control pill in 1978 in combination with ethinylestradiol under the brand name Diane.[20] Following phase III clinical trials, CPA was approved for the treatment of prostate cancer in Germany in 1980.[169][170] CPA became available in Canada as Androcur in 1987, as Androcur Depot in 1990, and as Diane-35 in 1998.[171][172][173] Conversely, CPA was never introduced in any form in the United States.[24][27] This was reportedly due to concerns about breast tumors observed with high-dose pregnane progestogens in beagle dogs as well as concerns about potential teratogenicity in pregnant women.[174] Use of CPA in transgender women, an off-label indication, was reported as early as 1977.[175][176] The use of CPA in transgender women was well-established by the early 1990s.[177]
The history of CPA, including its discovery, development, and marketing, has been reviewed.[178][13]
Society and culture
Generic names
The English and generic name of CPA is cyproterone acetate and this is its USAN, BAN, and JAN.[22][23][179][180] The English and generic name of unacetylated cyproterone is cyproterone and this is its INN and BAN,[179][180][181] while cyprotérone is the DCF and French name and ciproterone is the DCIT and Italian name.[22][23] The name of unesterified cyproterone in Latin is cyproteronum, in German is cyproteron, and in Spanish is ciproterona.[22][23] These names of cyproterone correspond for CPA to acétate de cyprotérone in French, acetato de ciproterona in Spanish, ciproterone acetato in Italian, cyproteronacetat in German, cyproteronacetaat in Dutch, and ciproteron acetat in Slavic. CPA is also known by the developmental code names SH-80714 and SH-714, while unacetylated cyproterone is known by the developmental code names SH-80881 and SH-881.[22][23][179][180]
Brand names
CPA is marketed under brand names including Androcur, Androcur Depot, Androcur-100, Androstat, Asoteron, Cyprone, Cyproplex, Cyprostat, Cysaxal, Imvel, and Siterone.[22][23] When CPA is formulated in combination with ethinylestradiol, it is also known as co-cyprindiol, and brand names for this formulation include Andro-Diane, Bella HEXAL 35, Chloe, Cypretil, Cypretyl, Cyproderm, Diane, Diane Mite, Diane-35, Dianette, Dixi 35, Drina, Elleacnelle, Estelle, Estelle-35, Ginette, Linface, Minerva, Vreya, and Zyrona.[22][23] CPA is also marketed in combination with estradiol valerate as Climen, Climene, Elamax, and Femilar.[22]
Availability

CPA is widely available throughout the world, and is marketed in almost every developed country,[182] with the notable major exceptions of the United States and Japan.[22][23][24][183][184] In almost all countries in which CPA is marketed, it is available both alone and in combination with an estrogen in birth control pills.[22][183][184] CPA is marketed widely in combination with both ethinylestradiol and estradiol valerate.[22][23][183][184] CPA-containing birth control pills are available in South Korea, but CPA as a standalone medication is not marketed in this country.[22][23][183][184] In Japan and South Korea, the closely related antiandrogen and progestin chlormadinone acetate, as well as other medications, are used instead of CPA.[185] Specific places in which CPA is marketed include the United Kingdom, elsewhere throughout Europe, Canada, Australia, New Zealand, South Africa, Latin America, and Asia.[22][23][183][184] CPA is not marketed in most of Africa and the Middle East.[22][23][183][184]
It has been said that the lack of availability of CPA in the United States explains why there are relatively few studies of it in the treatment of androgen-dependent conditions such as hyperandrogenism and hirsutism in women.[140]
Generation
Progestins in birth control pills are sometimes grouped by generation.[186][187] While the 19-nortestosterone progestins are consistently grouped into generations, the pregnane progestins that are or have been used in birth control pills are typically omitted from such classifications or are grouped simply as "miscellaneous" or "pregnanes".[186][187] In any case, CPA has been described as a "first-generation" progestin similarly to closely related progestins like chlormadinone acetate, medroxyprogesterone acetate, and megestrol acetate.[21][188]
Research
CPA has been studied and used in combination with low-dose diethylstilbestrol in the treatment of prostate cancer.[105][107][106] The combination results in suppression of testosterone levels into the castrate range, which normally cannot be achieved with CPA alone.[107] CPA has been studied as a form of androgen deprivation therapy for the treatment of benign prostatic hyperplasia (enlarged prostate).[189][190][191] The medication has been studied in the treatment of breast cancer as well.[192][193]
CPA has been studied for use as a potential male hormonal contraceptive both alone and in combination with testosterone in men.[194][195] CPA was under development by Barr Pharmaceuticals in the 2000s for the treatment of hot flashes in prostate cancer patients in the United States.[196] It reached phase III clinical trials for this indication and had the tentative brand name CyPat but development was ultimately discontinued in 2008.[196] CPA is not satisfactorily effective as topical antiandrogen, for instance in the treatment of acne.[153] CPA has been used to treat estrogen hypersensitivity vulvovaginitis in women.[197]
CPA has been investigated for use in reducing aggression and self-injurious behavior via its antiandrogenic effects in conditions like autism spectrum disorders, dementias like Alzheimer's disease, and psychosis.[198][199][200][201] CPA may be effective in the treatment of obsessive–compulsive disorder (OCD).[202][203][204][205] CPA has been studied in the treatment of cluster headaches in men.[206]
References
- Kuhl H (2005). "Pharmacology of estrogens and progestogens: influence of different routes of administration". Climacteric. 8 Suppl 1: 3–63. doi:10.1080/13697130500148875. PMID 16112947. S2CID 24616324.
- Huber J, Zeillinger R, Schmidt J, Täuber U, Kuhnz W, Spona J (November 1988). "Pharmacokinetics of cyproterone acetate and its main metabolite 15 beta-hydroxy-cyproterone acetate in young healthy women". Int J Clin Pharmacol Ther Toxicol. 26 (11): 555–61. PMID 2977383.
- Bińkowska M, Woroń J (June 2015). "Progestogens in menopausal hormone therapy". Przegla̜d Menopauzalny = Menopause Review. 14 (2): 134–43. doi:10.5114/pm.2015.52154. PMC 4498031. PMID 26327902.
- Schindler AE, Campagnoli C, Druckmann R, Huber J, Pasqualini JR, Schweppe KW, Thijssen JH (December 2003). "Classification and pharmacology of progestins" (PDF). Maturitas. 46 Suppl 1: S7–S16. doi:10.1016/j.maturitas.2003.09.014. PMID 14670641.
Since there is no binding of CPA to SHBG and CBG in the serum, 93% of the compound is bound to serum albumin.
- Wakelin SH, Maibach HI, Archer CB (1 June 2002). Systemic Drug Treatment in Dermatology: A Handbook. CRC Press. pp. 32–. ISBN 978-1-84076-013-2.
It is almost exclusively bound to plasma albumin.
- Hammond GL, Lähteenmäki PL, Lähteenmäki P, Luukkainen T (October 1982). "Distribution and percentages of non-protein bound contraceptive steroids in human serum". Journal of Steroid Biochemistry. 17 (4): 375–80. doi:10.1016/0022-4731(82)90629-X. PMID 6215538.
- Dickman A (27 September 2012). Drugs in Palliative Care. OUP Oxford. pp. 137–138. ISBN 978-0-19-966039-1.
- Boarder M, Newby D, Navti P (25 March 2010). Pharmacology for Pharmacy and the Health Sciences: A Patient-centred Approach. OUP Oxford. pp. 632–. ISBN 978-0-19-955982-4.
- Frith RG, Phillipou G (1985). "15-Hydroxycyproterone acetate and cyproterone acetate levels in plasma and urine". J. Chromatogr. 338 (1): 179–86. doi:10.1016/0378-4347(85)80082-7. PMID 3160716.
- Georg F. Weber (22 July 2015). Molecular Therapies of Cancer. Springer. pp. 316–. ISBN 978-3-319-13278-5.
The terminal half-life is about 38 h. A portion of the drug is metabolized by hydrolysis to cyproterone and acetic acid. However, in contrast to many other steroid esters hydrolysis is not extensive, and much of the pharmacological activity is exerted by the acetate form. Excretion is about 70% in the feces, mainly in the form of glucuronidated metabolites, and about 30% in the urine, predominantly as non-conjugated metabolites.
- Barradell LB, Faulds D (July 1994). "Cyproterone. A review of its pharmacology and therapeutic efficacy in prostate cancer". Drugs Aging. 5 (1): 59–80. doi:10.2165/00002512-199405010-00006. PMID 7919640.
- AAPL Newsletter (PDF). The Academy. 1998.
CPA is 100% bioavailable when taken orally with a half life of 38 hours. The injectable form reaches maximum plasma levels in 82 hours and has a half life of about 72 hours.
- Neumann F (1994). "The antiandrogen cyproterone acetate: discovery, chemistry, basic pharmacology, clinical use and tool in basic research". Exp. Clin. Endocrinol. 102 (1): 1–32. doi:10.1055/s-0029-1211261. PMID 8005205.
- Neumann F (January 1977). "Pharmacology and potential use of cyproterone acetate". Horm. Metab. Res. 9 (1): 1–13. doi:10.1055/s-0028-1093574. PMID 66176.
- Neumann F, Töpert M (November 1986). "Pharmacology of antiandrogens". Journal of Steroid Biochemistry. 25 (5B): 885–95. doi:10.1016/0022-4731(86)90320-1. PMID 2949114.
- Jonathan S. Berek (2007). Berek & Novak's Gynecology. Lippincott Williams & Wilkins. p. 1085. ISBN 978-0-7817-6805-4.
- Pucci E, Petraglia F (December 1997). "Treatment of androgen excess in females: yesterday, today and tomorrow". Gynecol. Endocrinol. 11 (6): 411–33. doi:10.3109/09513599709152569. PMID 9476091.
- Neumann F, Elger W (1966). "Permanent changes in gonadal function and sexual behaviour as a result of early feminization of male rats by treatment with an antiandrogenic steroid". Endokrinologie. 50 (5): 209–225. PMID 5989926.
- Sarah H. Wakelin (1 June 2002). Systemic Drug Treatment in Dermatology: A Handbook. CRC Press. p. 32. ISBN 978-1-84076-013-2.
- G. Plewig; A.M. Kligman (6 December 2012). ACNE and ROSACEA. Springer Science & Business Media. pp. 662, 685. ISBN 978-3-642-59715-2.
- Louw-du Toit R, Storbeck KH, Cartwright M, Cabral A, Africander D (February 2017). "Progestins used in endocrine therapy and the implications for the biosynthesis and metabolism of endogenous steroid hormones". Mol. Cell. Endocrinol. 441: 31–45. doi:10.1016/j.mce.2016.09.004. PMID 27616670. S2CID 38582443.
- "Cyproterone".
- Index Nominum 2000: International Drug Directory. Taylor & Francis. January 2000. pp. 289–. ISBN 978-3-88763-075-1.
- Loren S Schechter (22 September 2016). Surgical Management of the Transgender Patient. Elsevier Health Sciences. pp. 26–. ISBN 978-0-323-48408-4.
- J. Larry Jameson; Leslie J. De Groot (25 February 2015). Endocrinology: Adult and Pediatric E-Book. Elsevier Health Sciences. pp. 2293, 2464, 2479, 6225. ISBN 978-0-323-32195-2.
- Mario Maggi (17 November 2011). Hormonal Therapy for Male Sexual Dysfunction. John Wiley & Sons. p. 104. ISBN 978-1-119-96380-6.
- Duker M, Malsch M (28 January 2013). Incapacitation: Trends and New Perspectives. Ashgate Publishing, Ltd. p. 77. ISBN 978-1-4094-7151-6.
- https://www.bayer.ca/omr/online/diane-35-pm-en.pdf
- Fruzzetti F, Trémollieres F, Bitzer J (May 2012). "An overview of the development of combined oral contraceptives containing estradiol: focus on estradiol valerate/dienogest". Gynecol. Endocrinol. 28 (5): 400–8. doi:10.3109/09513590.2012.662547. PMC 3399636. PMID 22468839.
- Fruzzetti F, Bitzer J (2010). "Review of clinical experience with estradiol in combined oral contraceptives". Contraception. 81 (1): 8–15. doi:10.1016/j.contraception.2009.08.010. PMID 20004267.
- Gourdy P, Bachelot A, Catteau-Jonard S, Chabbert-Buffet N, Christin-Maître S, Conard J, Fredenrich A, Gompel A, Lamiche-Lorenzini F, Moreau C, Plu-Bureau G, Vambergue A, Vergès B, Kerlan V (November 2012). "Hormonal contraception in women at risk of vascular and metabolic disorders: guidelines of the French Society of Endocrinology". Ann. Endocrinol. (Paris). 73 (5): 469–87. doi:10.1016/j.ando.2012.09.001. PMID 23078975.
- Van der Spuy ZM, le Roux PA (2003). "Cyproterone acetate for hirsutism". Cochrane Database Syst Rev (4): CD001125. doi:10.1002/14651858.CD001125. PMID 14583927.
- Bitzer J, Römer T, Lopes da Silva Filho A (June 2017). "The use of cyproterone acetate/ethinyl estradiol in hyperandrogenic skin symptoms - a review". Eur J Contracept Reprod Health Care. 22 (3): 172–182. doi:10.1080/13625187.2017.1317339. PMID 28447864.
- Beylot C, Doutre MS, Beylot-Barry M (1998). "Oral contraceptives and cyproterone acetate in female acne treatment". Dermatology (Basel). 196 (1): 148–52. doi:10.1159/000017849. PMID 9557250. S2CID 46763689.
- Miller JA, Jacobs HS (May 1986). "Treatment of hirsutism and acne with cyproterone acetate". Clin Endocrinol Metab. 15 (2): 373–89. doi:10.1016/S0300-595X(86)80031-7. PMID 2941191.
- Ingram JR, Woo PN, Chua SL, Ormerod AD, Desai N, Kai AC, Hood K, Burton T, Kerdel F, Garner SE, Piguet V (October 2015). "Interventions for hidradenitis suppurativa". Cochrane Database Syst Rev (10): CD010081. doi:10.1002/14651858.CD010081.pub2. PMC 6464653. PMID 26443004.
- Ioannides D, Lazaridou E (2015). "Female pattern hair loss". Alopecias - Practical Evaluation and Management. Curr. Probl. Dermatol. Current Problems in Dermatology. 47. pp. 45–54. doi:10.1159/000369404. ISBN 978-3-318-02774-7. PMID 26370643.
- Wiegratz I, Kuhl H (2002). "Managing cutaneous manifestations of hyperandrogenic disorders: the role of oral contraceptives". Treat Endocrinol. 1 (6): 372–86. doi:10.2165/00024677-200201060-00003. PMID 15832490. S2CID 71806394.
- Arowojolu AO, Gallo MF, Lopez LM, Grimes DA (July 2012). Arowojolu AO (ed.). "Combined oral contraceptive pills for treatment of acne". Cochrane Database Syst Rev (7): CD004425. doi:10.1002/14651858.CD004425.pub6. PMID 22786490.
- Diamanti-Kandarakis E (September 1999). "Current aspects of antiandrogen therapy in women". Curr. Pharm. Des. 5 (9): 707–23. PMID 10495361.
- Bettoli V, Zauli S, Virgili A (2015). "Is hormonal treatment still an option in acne today?". Br. J. Dermatol. 172 Suppl 1: 37–46. doi:10.1111/bjd.13681. PMID 25627824. S2CID 35615492.
- Reed MJ, Franks S (September 1988). "Anti-androgens in gynaecological practice". Baillière's Clin Obstet Gynaecol. 2 (3): 581–95. doi:10.1016/S0950-3552(88)80045-2. PMID 2976627.
- Sahin, Yilmaz; Kelestimur, Fahrettin (2004). "Medical treatment regimens of hirsutism". Reproductive BioMedicine Online. 8 (5): 538–546. doi:10.1016/S1472-6483(10)61100-5. ISSN 1472-6483. PMID 15151716.
- Nikolaou D, Gilling-Smith C (2005). "Hirsutism". Current Obstetrics & Gynaecology. 15 (3): 174–182. doi:10.1016/j.curobgyn.2005.03.006. ISSN 0957-5847.
- Rittmaster, Roger S (1997). "Hirsutism". The Lancet. 349 (9046): 191–195. doi:10.1016/S0140-6736(96)07252-2. ISSN 0140-6736. PMID 9111556. S2CID 208789457.
- Azziz R, Carmina E, Sawaya ME (August 2000). "Idiopathic hirsutism". Endocrine Reviews. 21 (4): 347–62. doi:10.1210/edrv.21.4.0401. PMID 10950156.
- Liew SH (June 1999). "Unwanted body hair and its removal: a review". Dermatologic Surgery. 25 (6): 431–9. doi:10.1046/j.1524-4725.1999.08130.x. PMID 10469088.
- Belisle S, Love EJ (December 1986). "Clinical efficacy and safety of cyproterone acetate in severe hirsutism: results of a multicentered Canadian study". Fertility and Sterility. 46 (6): 1015–20. doi:10.1016/S0015-0282(16)49873-0. PMID 2946604.
- Barth JH, Cherry CA, Wojnarowska F, Dawber RP (July 1991). "Cyproterone acetate for severe hirsutism: results of a double-blind dose-ranging study". Clinical Endocrinology. 35 (1): 5–10. doi:10.1111/j.1365-2265.1991.tb03489.x. PMID 1832346. S2CID 27293697.
- Jasonni VM, Bulletti C, Naldi S, Di Cosmo E, Cappuccini F, Flamigni C (April 1991). "Treatment of hirsutism by an association of oral cyproterone acetate and transdermal 17 beta-estradiol". Fertility and Sterility. 55 (4): 742–5. doi:10.1016/S0015-0282(16)54240-X. PMID 1826278.
- Hammerstein, J. (1990). "Antiandrogens: Clinical Aspects". Hair and Hair Diseases. pp. 827–886. doi:10.1007/978-3-642-74612-3_35. ISBN 978-3-642-74614-7.
- Ward A, Brogden RN, Heel RC, Speight TM, Avery GS (July 1984). "Isotretinoin. A review of its pharmacological properties and therapeutic efficacy in acne and other skin disorders". Drugs. 28 (1): 6–37. doi:10.2165/00003495-198428010-00002. PMID 6235105.
- Rasmusson, Gary H. (1986). Chapter 18. Chemical Control of Androgen Action. Annual Reports in Medicinal Chemistry. 21. pp. 179–188. doi:10.1016/S0065-7743(08)61128-8. ISBN 9780120405213. ISSN 0065-7743.
- Cormane, R. H.; van der Meeren, H. L. M. (1981). "Cyproteronacetate in the management of severe acne in males". Archives of Dermatological Research. 271 (2): 183–187. doi:10.1007/BF00412545. ISSN 0340-3696. S2CID 12153042.
- Misch KJ, Dolman WF, Neild V, Rhodes EL (1986). "Response of male acne to antiandrogen therapy with cyproterone acetate". Dermatologica. 173 (3): 139–42. doi:10.1159/000249236. PMID 2945742.
- Simpson, N. B. (1989). "The Effect of Drugs on Hair". Pharmacology of the Skin II. Handbook of Experimental Pharmacology. 87 / 2. pp. 495–508. doi:10.1007/978-3-642-74054-1_37. ISBN 978-3-642-74056-5. ISSN 0171-2004.
- Walter P. Unger (1 February 1995). "Androgenetic alopecia and its treatment. A historical overview". Hair Transplantation, Third Edition. Taylor & Francis. pp. 1–33. ISBN 978-0-8247-9363-0.
- Coskey, Ralph J. (1984). "Dermatologic therapy: December, 1982, through November, 1983". Journal of the American Academy of Dermatology. 11 (1): 25–52. doi:10.1016/S0190-9622(84)80163-2. ISSN 0190-9622. PMID 6376557.
- Neumann F, Kalmus J (1991). "Cyproterone acetate in the treatment of sexual disorders: pharmacological base and clinical experience". Exp. Clin. Endocrinol. 98 (2): 71–80. doi:10.1055/s-0029-1211103. PMID 1838080.
- Giltay EJ, Gooren LJ (2009). "Potential side effects of androgen deprivation treatment in sex offenders". The Journal of the American Academy of Psychiatry and the Law. 37 (1): 53–8. PMID 19297634.
- Lam, Samuel M.; Hempstead, Brian R.; Williams, Edwin F. (2012). "Medical Management Options for Hair Loss". Aesthetic Medicine. pp. 529–535. doi:10.1007/978-3-642-20113-4_41. ISBN 978-3-642-20112-7.
- Neumann, Friedmund (1996). "Pharmacology of Cyproterone Acetate — A Short Review". Antiandrogens in Prostate Cancer. pp. 31–44. doi:10.1007/978-3-642-45745-6_3. ISBN 978-3-642-45747-0.
- Ruan X, Kubba A, Aguilar A, Mueck AO (June 2017). "Use of cyproterone acetate/ethinylestradiol in polycystic ovary syndrome: rationale and practical aspects". Eur J Contracept Reprod Health Care. 22 (3): 183–190. doi:10.1080/13625187.2017.1317735. PMID 28463030.
- Laron Z, Kauli R (July 2000). "Experience with cyproterone acetate in the treatment of precocious puberty". J. Pediatr. Endocrinol. Metab. 13 Suppl 1: 805–10. doi:10.1515/JPEM.2000.13.S1.805. PMID 10969925. S2CID 25398066.
- Catteau-Jonard S, Cortet-Rudelli C, Richard-Proust C, Dewailly D (2012). "Hyperandrogenism in adolescent girls". Pediatric and Adolescent Gynecology. Endocr Dev. Endocrine Development. 22. pp. 181–93. doi:10.1159/000326688. ISBN 978-3-8055-9336-6. PMID 22846529.
- Reismann P, Likó I, Igaz P, Patócs A, Rácz K (August 2009). "Pharmacological options for treatment of hyperandrogenic disorders". Mini Rev Med Chem. 9 (9): 1113–26. doi:10.2174/138955709788922692. PMID 19689407.
- Diamanti-Kandarakis E (October 1998). "How actual is the treatment with antiandrogen alone in patients with polycystic ovary syndrome?". J. Endocrinol. Invest. 21 (9): 623–9. doi:10.1007/BF03350788. PMID 9856417. S2CID 46484837.
- Husmann, Friedrich (1997). "Clinical Experiences with a Combination of Estradiol Valerate and Cyproterone Acetate for Hormone Replacement". Women's Health and Menopause. Medical Science Symposia Series. 11. pp. 257–261. doi:10.1007/978-94-011-5560-1_38. ISBN 978-94-010-6343-2. ISSN 0928-9550.
- Schneider HP (November 2003). "Androgens and antiandrogens". Ann. N. Y. Acad. Sci. 997 (1): 292–306. Bibcode:2003NYASA.997..292S. doi:10.1196/annals.1290.033. PMID 14644837. S2CID 8400556.
- Schneider HP (December 2000). "The role of antiandrogens in hormone replacement therapy". Climacteric. 3 Suppl 2: 21–7. PMID 11379383.
- Gooren LJ, Giltay EJ, Bunck MC (January 2008). "Long-term treatment of transsexuals with cross-sex hormones: extensive personal experience". The Journal of Clinical Endocrinology and Metabolism. 93 (1): 19–25. doi:10.1210/jc.2007-1809. PMID 17986639.
- Hembree WC, Cohen-Kettenis PT, Gooren L, Hannema SE, Meyer WJ, Murad MH, et al. (November 2017). "Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline". The Journal of Clinical Endocrinology and Metabolism. 102 (11): 3869–3903. doi:10.1210/jc.2017-01658. PMID 28945902.
- Chew D, Anderson J, Williams K, May T, Pang K (April 2018). "Hormonal Treatment in Young People With Gender Dysphoria: A Systematic Review". Pediatrics. 141 (4): e20173742. doi:10.1542/peds.2017-3742. PMID 29514975.
- Deutsch M (17 June 2016), Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People (PDF) (2nd ed.), University of California, San Francisco: Center of Excellence for Transgender Health, p. 28
- James Barrett (29 September 2017). Transsexual and Other Disorders of Gender Identity: A Practical Guide to Management. CRC Press. pp. 216–217, 221. ISBN 978-1-315-34513-0.
- Randi Ettner; Stan Monstrey; Eli Coleman (20 May 2016). Principles of Transgender Medicine and Surgery. Routledge. pp. 169, 171, 216. ISBN 978-1-317-51460-2.
- Gianna E. Israel (March 2001). Transgender Care: Recommended Guidelines, Practical Information, and Personal Accounts. Temple University Press. pp. 66–. ISBN 978-1-56639-852-7.
- Winkler-Crepaz K, Mueller A, Boettcher B, Wildt L (2017). "Hormonbehandlung bei Transgenderpatienten" [Hormone treatment of transgender patients]. Gynäkologische Endokrinologie. 15 (1): 39–42. doi:10.1007/s10304-016-0116-9. ISSN 1610-2894. S2CID 12270365.
- Urdl W (2009). "Behandlungsgrundsätze bei Transsexualität" [Therapeutic principles in transsexualism]. Gynäkologische Endokrinologie. 7 (3): 153–160. doi:10.1007/s10304-009-0314-9. ISSN 1610-2894. S2CID 8001811.
- Meyer G, Mayer M, Mondorf A, Fluegel AK, Herrmann E, Bojunga J (November 2019). "Safety and rapid efficacy of guideline-based gender affirming hormone therapy: an analysis of 388 individuals diagnosed with gender dysphoria". European Journal of Endocrinology. 182 (2): 149–156. doi:10.1530/EJE-19-0463. PMID 31751300.
- Fung R, Hellstern-Layefsky M, Lega I (2017). "Is a lower dose of cyproterone acetate as effective at testosterone suppression in transgender women as higher doses?". International Journal of Transgenderism. 18 (2): 123–128. doi:10.1080/15532739.2017.1290566. ISSN 1553-2739. S2CID 79095497.
- Panagiotakopoulos, Leonidas (2018). "Transgender medicine - puberty suppression". Reviews in Endocrine and Metabolic Disorders. 19 (3): 221–225. doi:10.1007/s11154-018-9457-0. ISSN 1389-9155. PMID 30112593. S2CID 52009542.
- Rosenthal SM (December 2014). "Approach to the patient: transgender youth: endocrine considerations". J. Clin. Endocrinol. Metab. 99 (12): 4379–89. doi:10.1210/jc.2014-1919. PMID 25140398.
- Mahfouda S, Moore JK, Siafarikas A, Zepf FD, Lin A (October 2017). "Puberty suppression in transgender children and adolescents". Lancet Diabetes Endocrinol. 5 (10): 816–826. doi:10.1016/S2213-8587(17)30099-2. PMID 28546095.
- Tack LJ, Heyse R, Craen M, Dhondt K, Bossche H, Laridaen J, Cools M (May 2017). "Consecutive Cyproterone Acetate and Estradiol Treatment in Late-Pubertal Transgender Female Adolescents". J Sex Med. 14 (5): 747–757. doi:10.1016/j.jsxm.2017.03.251. PMID 28499525.
- Torri V, Floriani I (June 2005). "Cyproterone acetate in the therapy of prostate carcinoma". Archivio Italiano di Urologia, Andrologia. 77 (3): 157–63. CiteSeerX 10.1.1.663.9458. PMID 16372511.
- Schröder, Fritz H. (1996). "Cyproterone Acetate — Results of Clinical Trials and Indications for Use in Human Prostate Cancer". Antiandrogens in Prostate Cancer. pp. 45–51. doi:10.1007/978-3-642-45745-6_4. ISBN 978-3-642-45747-0.
- Schröder FH (December 1993). "Cyproterone acetate--mechanism of action and clinical effectiveness in prostate cancer treatment". Cancer. 72 (12 Suppl): 3810–5. doi:10.1002/1097-0142(19931215)72:12+<3810::AID-CNCR2820721710>3.0.CO;2-O. PMID 8252496.
- de Voogt HJ (1992). "The position of cyproterone acetate (CPA), a steroidal anti-androgen, in the treatment of prostate cancer". The Prostate. Supplement. 4: 91–5. doi:10.1002/pros.2990210514. PMID 1533452. S2CID 22747185.
- Goldenberg SL, Bruchovsky N (February 1991). "Use of cyproterone acetate in prostate cancer". The Urologic Clinics of North America. 18 (1): 111–22. PMID 1825143.
- Thomas L. Lemke; David A. Williams (2008). Foye's Principles of Medicinal Chemistry. Lippincott Williams & Wilkins. pp. 1288–. ISBN 978-0-7817-6879-5.
- Seidenfeld J, Samson DJ, Hasselblad V, Aronson N, Albertsen PC, Bennett CL, Wilt TJ (April 2000). "Single-therapy androgen suppression in men with advanced prostate cancer: a systematic review and meta-analysis". Annals of Internal Medicine. 132 (7): 566–77. doi:10.7326/0003-4819-132-7-200004040-00009. PMID 10744594. S2CID 23128641.
- Mydlo JH, Godec CJ (29 September 2015). Prostate Cancer: Science and Clinical Practice. Elsevier Science. pp. 516–521, 534–540. ISBN 978-0-12-800592-7. Archived from the original on 8 September 2017.
- Miyamoto H, Messing EM, Chang C (December 2004). "Androgen deprivation therapy for prostate cancer: current status and future prospects". The Prostate. 61 (4): 332–53. doi:10.1002/pros.20115. PMID 15389811. S2CID 22300358.
- Wirth MP, Hakenberg OW, Froehner M (February 2007). "Antiandrogens in the treatment of prostate cancer". European Urology. 51 (2): 306–13, discussion 314. doi:10.1016/j.eururo.2006.08.043. PMID 17007995.
- Singh SM, Gauthier S, Labrie F (February 2000). "Androgen receptor antagonists (antiandrogens): structure-activity relationships". Current Medicinal Chemistry. 7 (2): 211–47. doi:10.2174/0929867003375371. PMID 10637363.
When compared to flutamide, [cyproterone acetate] has significant intrinsic androgenic and estrogenic activities. [...] The effects of flutamide and the steroidal derivatives, cyproterone acetate, chlormadinone acetate, megestrol acetate and medroxyprogesterone acetate were compared in vivo in female nude mice bearing androgen-sensitive Shionogi tumors. All steroidal compounds stimulated tumor growth while flutamide had no stimulatory effect [51]. Thus, CPA due to its intrinsic properties stimulates androgen-sensitive parameters and cancer growth. Cyproterone acetate added to castration has never been shown in any controlled study to prolong disease-free survival or overall survival in prostate cancer when compared with castration alone [152-155].
- Kaliks RA, Del Giglio A (2008). "Management of advanced prostate cancer" (PDF). Revista da Associacao Medica Brasileira. 54 (2): 178–82. doi:10.1590/S0104-42302008000200025. PMID 18506331. Archived (PDF) from the original on 10 May 2017.
- Chabner BA, Longo DL (8 November 2010). Cancer Chemotherapy and Biotherapy: Principles and Practice. Lippincott Williams & Wilkins. pp. 679–680. ISBN 978-1-60547-431-1.
From a structural standpoint, antiandrogens are classified as steroidal, including cyproterone [acetate] (Androcur) and megestrol [acetate], or nonsteroidal, including flutamide (Eulexin, others), bicalutamide (Casodex), and nilutamide (Nilandron). The steroidal antiandrogens are rarely used.
- Alan Horwich (11 February 2010). Systemic Treatment of Prostate Cancer. OUP Oxford. pp. 44–. ISBN 978-0-19-956142-1.
- Anderson J (March 2003). "The role of antiandrogen monotherapy in the treatment of prostate cancer". BJU Int. 91 (5): 455–61. doi:10.1046/j.1464-410X.2003.04026.x. PMID 12603397. S2CID 8639102.
- Dalesio O, van Tinteren H, Clarke M, Peto R, Schroder F, Dechering I, Evans V, Godwin J, Blumenstein B, Crawford E, Denis L, Hall R, Hill C, Iversen P, Shipley W, Soloway M, Sylvester R (2000). "Maximum androgen blockade in advanced prostate cancer: an overview of the randomised trials". The Lancet. 355 (9214): 1491–1498. doi:10.1016/S0140-6736(00)02163-2. ISSN 0140-6736.
- Louis Denis (6 December 2012). Antiandrogens in Prostate Cancer: A Key to Tailored Endocrine Treatment. Springer Science & Business Media. pp. 70–. ISBN 978-3-642-45745-6.
- Schröder, Fritz H.; Radlmaier, Albert (2009). "Steroidal Antiandrogens". In V. Craig Jordan; Barrington J. A. Furr (eds.). Hormone Therapy in Breast and Prostate Cancer. Humana Press. pp. 325–346. doi:10.1007/978-1-59259-152-7_15. ISBN 978-1-60761-471-5.
- Chodak G, Gomella L, Phung de H (September 2007). "Combined androgen blockade in advanced prostate cancer: looking back to move forward". Clin Genitourin Cancer. 5 (6): 371–8. doi:10.3816/CGC.2007.n.019. PMID 17956709.
- Cox RL, Crawford ED (December 1995). "Estrogens in the treatment of prostate cancer". J. Urol. 154 (6): 1991–8. doi:10.1016/S0022-5347(01)66670-9. PMID 7500443.
- Goldenberg SL, Bruchovsky N, Gleave ME, Sullivan LD (June 1996). "Low-dose cyproterone acetate plus mini-dose diethylstilbestrol--a protocol for reversible medical castration". Urology. 47 (6): 882–4. doi:10.1016/S0090-4295(96)00048-9. PMID 8677581.
- Goldenberg SL, Bruchovsky N, Rennie PS, Coppin CM (December 1988). "The combination of cyproterone acetate and low dose diethylstilbestrol in the treatment of advanced prostatic carcinoma". J. Urol. 140 (6): 1460–5. doi:10.1016/S0022-5347(17)42073-8. PMID 2973529.
- Wolfgang Hinkelbein; Kurt Miller; Thomas Wiegel (7 March 2013). Prostatakarzinom — urologische und strahlentherapeutische Aspekte: urologische und strahlentherapeutische Aspekte [Prostate carcinoma — urological and radiotherapeutic aspects: urological and radiotherapeutic aspects]. Springer-Verlag. pp. 99–. ISBN 978-3-642-60064-7.
- Khan O, Ferriter M, Huband N, Powney MJ, Dennis JA, Duggan C (February 2015). "Pharmacological interventions for those who have sexually offended or are at risk of offending". Cochrane Database Syst Rev (2): CD007989. doi:10.1002/14651858.CD007989.pub2. PMC 6544815. PMID 25692326.
- Silvani M, Mondaini N, Zucchi A (September 2015). "Androgen deprivation therapy (castration therapy) and pedophilia: What's new". Arch Ital Urol Androl. 87 (3): 222–6. doi:10.4081/aiua.2015.3.222. PMID 26428645.
- Reilly DR, Delva NJ, Hudson RW (August 2000). "Protocols for the use of cyproterone, medroxyprogesterone, and leuprolide in the treatment of paraphilia". Can J Psychiatry. 45 (6): 559–63. doi:10.1177/070674370004500608. PMID 10986575.
- Freund K (1980). "Therapeutic sex drive reduction". Acta Psychiatr Scand Suppl. 287: 5–38. doi:10.1111/j.1600-0447.1980.tb10433.x. PMID 7006321. S2CID 21981060.
- Codispoti VL (December 2008). "Pharmacology of sexually compulsive behavior". Psychiatr. Clin. North Am. 31 (4): 671–9. doi:10.1016/j.psc.2008.06.002. PMID 18996306.
- Assumpção AA, Garcia FD, Garcia HD, Bradford JM, Thibaut F (June 2014). "Pharmacologic treatment of paraphilias". Psychiatr. Clin. North Am. 37 (2): 173–81. doi:10.1016/j.psc.2014.03.002. PMID 24877704.
- Guay DR (December 2008). "Inappropriate sexual behaviors in cognitively impaired older individuals". Am J Geriatr Pharmacother. 6 (5): 269–88. doi:10.1016/j.amjopharm.2008.12.004. PMID 19161930.
- Clarke DJ (April 1989). "Antilibidinal drugs and mental retardation: a review". Med Sci Law. 29 (2): 136–46. doi:10.1177/002580248902900209. PMID 2526280. S2CID 37808515.
- Hucker SJ (June 1985). "Self-harmful sexual behavior". Psychiatr. Clin. North Am. 8 (2): 323–37. doi:10.1016/s0193-953x(18)30698-1. PMID 3895195.
- Laschet U, Laschet L (June 1975). "Antiandrogens in the treatment of sexual deviations of men". J. Steroid Biochem. 6 (6): 821–6. doi:10.1016/0022-4731(75)90310-6. PMID 1177426.
- Brito VN, Latronico AC, Arnhold IJ, Mendonça BB (February 2008). "Update on the etiology, diagnosis and therapeutic management of sexual precocity". Arq Bras Endocrinol Metabol. 52 (1): 18–31. doi:10.1590/S0004-27302008000100005. PMID 18345393.
- Anupam Sachdeva; AK Dutta (31 August 2012). Advances in Pediatrics. JP Medical Ltd. pp. 1202–. ISBN 978-93-5025-777-7.
- Holland FJ (March 1991). "Gonadotropin-independent precocious puberty". Endocrinol. Metab. Clin. North Am. 20 (1): 191–210. doi:10.1016/s0889-8529(18)30288-3. PMID 1903104.
- Frisk J (January 2010). "Managing hot flushes in men after prostate cancer--a systematic review". Maturitas. 65 (1): 15–22. doi:10.1016/j.maturitas.2009.10.017. PMID 19962840.
- Spetz AC, Zetterlund EL, Varenhorst E, Hammar M (2003). "Incidence and management of hot flashes in prostate cancer". J Support Oncol. 1 (4): 263–6, 269–70, 272–3, discussion 267–8, 271–2. PMID 15334868.
- Radlmaier A, Bormacher K, Neumann F (1990). "Hot flushes: mechanism and prevention". Prog. Clin. Biol. Res. 359: 131–40, discussion 141–53. PMID 2149457.
- Thompson IM (2001). "Flare Associated with LHRH-Agonist Therapy". Rev Urol. 3 Suppl 3: S10–4. PMC 1476081. PMID 16986003.
- Louis J Denis; Keith Griffiths; Amir V Kaisary; Gerald P Murphy (1 March 1999). Textbook of Prostate Cancer: Pathology, Diagnosis and Treatment: Pathology, Diagnosis and Treatment. CRC Press. pp. 308–. ISBN 978-1-85317-422-3.
- Sugiono M, Winkler MH, Okeke AA, Benney M, Gillatt DA (2005). "Bicalutamide vs cyproterone acetate in preventing flare with LHRH analogue therapy for prostate cancer—a pilot study". Prostate Cancer and Prostatic Diseases. 8 (1): 91–4. doi:10.1038/sj.pcan.4500784. PMID 15711607.
- Schulze H, Senge T (October 1990). "Influence of different types of antiandrogens on luteinizing hormone-releasing hormone analogue-induced testosterone surge in patients with metastatic carcinoma of the prostate". J. Urol. 144 (4): 934–41. doi:10.1016/S0022-5347(17)39625-8. PMID 2144596.
- Boccon-Gibod L, Laudat MH, Dugue MA, Steg A (1986). "Cyproterone acetate lead-in prevents initial rise of serum testosterone induced by luteinizing hormone-releasing hormone analogs in the treatment of metastatic carcinoma of the prostate". Eur. Urol. 12 (6): 400–2. doi:10.1159/000472667. PMID 2949980.
- Klosterhalfen, H.; Jacobi, G. H. (1988). "Long-term results of an LH-RH agonist monotherapy in patients with carcinoma of the prostate and reflections on the so-called total androgen blockade with pre-medicated cyproterone acetate". In Klosterhalfen, H. (ed.). Endocrine Management of Prostatic Cancer. De Gruyter. pp. 127–137. doi:10.1515/9783110853674-014. ISBN 9783110853674.
- Bruchovsky N, Goldenberg SL, Akakura K, Rennie PS (September 1993). "Luteinizing hormone-releasing hormone agonists in prostate cancer. Elimination of flare reaction by pretreatment with cyproterone acetate and low-dose diethylstilbestrol". Cancer. 72 (5): 1685–91. doi:10.1002/1097-0142(19930901)72:5<1685::AID-CNCR2820720532>3.0.CO;2-3. PMID 7688656.
- Rabe T, Albring C, Blume-Peytavi U, Egarter C, Geisthövel F, König K, Kuhl H, Merkle E, Mueck AO, Reisch N, Schüring A, Stute P, Toth B, Wildt L, Zouboulis CC (2015). "Hirsutismus – Medikamentöse Therapie Gemeinsame Stellungnahme der Deutschen Gesellschaft für Gynäkologische Endokrinologie und Fortpflanzungsmedizin e.V. und des Berufsverbands der Frauenärzte e.V." [Hirsutism – Medicinal treatment. Joint statement of the German Society of Gynaecological Endocrinology and Reproductive Medicine and the Professional Association of Gynaecologists]. Journal für Reproduktionsmedizin und Endokrinologie (in German). 12 (3): 102–149. ISSN 1810-2107.
- Jürgen Engel; Axel Kleemann; Bernhard Kutscher; Dietmar Reichert (14 May 2014). Pharmaceutical Substances, 5th Edition, 2009: Syntheses, Patents and Applications of the most relevant APIs. Thieme. pp. 351–352. ISBN 978-3-13-179275-4.
- Muller (19 June 1998). European Drug Index: European Drug Registrations, Fourth Edition. CRC Press. pp. 79–. ISBN 978-3-7692-2114-5.
- Jean L. Bolognia; Joseph L. Jorizzo; Julie V. Schaffer (8 June 2012). Dermatology E-Book. Elsevier Health Sciences. pp. 557–. ISBN 978-0-7020-5182-1.
- Peter Altmeyer (2 July 2013). Therapielexikon Dermatologie und Allergologie. Springer-Verlag. pp. 27–. ISBN 978-3-662-10498-9.
- Jerome P. Kassirer; Harry L. Greene (1997). Current Therapy in Adult Medicine. Mosby. p. 174. ISBN 978-0-8151-5480-8.
- "Androcur Label" (PDF).
- "Mylan-Cyproterone Label" (PDF).
- Bachelot A, Chabbert-Buffet N, Salenave S, Kerlan V, Galand-Portier MB (February 2010). "Anti-androgen treatments". Ann. Endocrinol. (Paris). 71 (1): 19–24. doi:10.1016/j.ando.2009.12.001. PMID 20096826.
- Burton JL (December 1979). "Anti-androgen therapy in dermatology: a review". Clin. Exp. Dermatol. 4 (4): 501–7. doi:10.1111/j.1365-2230.1979.tb01648.x. PMID 394887. S2CID 29236094.
- Rittmaster RS (June 1999). "Antiandrogen treatment of polycystic ovary syndrome". Endocrinol. Metab. Clin. North Am. 28 (2): 409–21. doi:10.1016/S0889-8529(05)70077-3. PMID 10352926.
- Guay DR (January 2009). "Drug treatment of paraphilic and nonparaphilic sexual disorders". Clin Ther. 31 (1): 1–31. doi:10.1016/j.clinthera.2009.01.009. PMID 19243704.
No quantitative data on these adverse events are available, even in the product prescribing information and data sheets.
- Migliari R, Muscas G, Murru M, Verdacchi T, De Benedetto G, De Angelis M (December 1999). "Antiandrogens: a summary review of pharmacodynamic properties and tolerability in prostate cancer therapy". Arch Ital Urol Androl. 71 (5): 293–302. PMID 10673793.
- Fabian M. Saleh; Albert J. Grudzinskas; John M. Bradford (11 February 2009). Sex Offenders: Identification, Risk Assessment, Treatment, and Legal Issues. Oxford University Press, USA. pp. 197–. ISBN 978-0-19-517704-6.
- Marc A. Fritz; Leon Speroff (2011). Clinical Gynecologic Endocrinology and Infertility. Lippincott Williams & Wilkins. pp. 1091–. ISBN 978-0-7817-7968-5.
- Figg W, Chau CH, Small EJ (14 September 2010). Drug Management of Prostate Cancer. Springer. p. 71. ISBN 978-1-60327-829-4.
- Honer C, Nam K, Fink C, Marshall P, Ksander G, Chatelain RE, et al. (May 2003). "Glucocorticoid receptor antagonism by cyproterone acetate and RU486". Molecular Pharmacology. 63 (5): 1012–20. doi:10.1124/mol.63.5.1012. PMID 12695529.
- Ayub M, Levell MJ (July 1987). "Inhibition of rat testicular 17 alpha-hydroxylase and 17,20-lyase activities by anti-androgens (flutamide, hydroxyflutamide, RU23908, cyproterone acetate) in vitro". Journal of Steroid Biochemistry. 28 (1): 43–7. doi:10.1016/0022-4731(87)90122-1. PMID 2956461.
- Han C, Davis CB, Wang B (6 January 2010). Evaluation of Drug Candidates for Preclinical Development: Pharmacokinetics, Metabolism, Pharmaceutics, and Toxicology. John Wiley & Sons. pp. 92–. ISBN 978-0-470-57488-1.
- Lehmann JM, McKee DD, Watson MA, Willson TM, Moore JT, Kliewer SA (September 1998). "The human orphan nuclear receptor PXR is activated by compounds that regulate CYP3A4 gene expression and cause drug interactions". The Journal of Clinical Investigation. 102 (5): 1016–23. doi:10.1172/JCI3703. PMC 508967. PMID 9727070.
- Christians U, Schmitz V, Haschke M (December 2005). "Functional interactions between P-glycoprotein and CYP3A in drug metabolism". Expert Opinion on Drug Metabolism & Toxicology. 1 (4): 641–54. doi:10.1517/17425255.1.4.641. PMID 16863430. S2CID 17742146.
- Gräf KJ, Brotherton J, Neumann F (1974). Androgens II and Antiandrogens / Androgene II und Antiandrogene. pp. 485–542. doi:10.1007/978-3-642-80859-3_7. ISBN 978-3-642-80861-6.
- John V. Knaus; John H. Isaacs (6 December 2012). Office Gynecology: Advanced Management Concepts. Springer Science & Business Media. pp. 150–. ISBN 978-1-4612-4340-3.
- William Andrew Publishing (22 October 2013). Pharmaceutical Manufacturing Encyclopedia. Elsevier. pp. 1182–1183. ISBN 978-0-8155-1856-3.
- Duang Buddhasukh, Roland Maier, Aranya Manosroi, Jiradej Manosroi, Pattana Sripalakit, Rolf Werner (29 April 2002). "EP1359154A1 Further syntheses of cyproterone acetate". Google Patents.CS1 maint: uses authors parameter (link)
- "Verfahren zur Herstellung von 1, 2alpha-Methylen-delta-17alpha-hydroxy-progesteronen".
- "6-chloro-1, 2alpha-methylene-delta6-17alpha-hydroxyprogesterone compounds and compositions".
- U.S. Patent 3,234,093
- Hamada H, Neumann F, Junkmann K (November 1963). "Intrauterine Antimaskuline Beeinflussung von Rattenfeten Durch ein Stark Gestagen Wirksames Steroid" [Intrauterine antimasculine influence of Rat Fetuses by Birtue of a Powerful Steroid Acting as a Progestogen]. Acta Endocrinologica (in German). 44 (3): 380–8. doi:10.1530/acta.0.0440380. PMID 14071315.
- T. Mann; C. Lutwak-Mann (6 December 2012). Male Reproductive Function and Semen: Themes and Trends in Physiology, Biochemistry and Investigative Andrology. Springer Science & Business Media. pp. 352–. ISBN 978-1-4471-1300-3.
- Norman AW, Litwack G (28 June 2014). Hormones. Elsevier Science. pp. 508–. ISBN 978-1-4832-5810-2.
- W.I.P. Mainwaring (6 December 2012). The Mechanism of Action of Androgens. Springer Science & Business Media. pp. 53–. ISBN 978-3-642-88429-0.
- Jost A (1971). "Use of androgen antagonists and antiandrogens in studies on sex differentiation". Gynecol Invest. 2 (1): 180–201. doi:10.1159/000301861. PMID 4949979.
- Thibaut F, De La Barra F, Gordon H, Cosyns P, Bradford JM (June 2010). "The World Federation of Societies of Biological Psychiatry (WFSBP) guidelines for the biological treatment of paraphilias". The World Journal of Biological Psychiatry. 11 (4): 604–55. doi:10.3109/15622971003671628. PMID 20459370. S2CID 14949511.
- Namer M (October 1988). "Clinical applications of antiandrogens". Journal of Steroid Biochemistry. 31 (4B): 719–29. doi:10.1016/0022-4731(88)90023-4. PMID 2462132.
- Hammerstein J, Cupceancu B (April 1969). "[Management of hirsutism using cyproterone acetate]" [Management of hirsutism using cyproterone acetate]. Deutsche Medizinische Wochenschrift (in German). 94 (16): 829–34. doi:10.1055/s-0028-1111126. PMID 4304873.
- Tobias JS, Hochhauser D (3 October 2014). Cancer and its Management. Wiley. pp. 379–. ISBN 978-1-118-46871-5.
- Jacobi, GR; Tunn, UW; Senge, TH (1 December 1982). "Clinical experience with cyproterone acetate for palliation of inoperable prostate cancer". In Jacobi, Günther H; Hohenfellner, Rudolf (eds.). Prostate Cancer. Williams & Wilkins. pp. 305–319. ISBN 978-0-683-04354-9.
- Jacobi GH, Altwein JE, Kurth KH, Basting R, Hohenfellner R (June 1980). "Treatment of advanced prostatic cancer with parenteral cyproterone acetate: a phase III randomised trial". British Journal of Urology. 52 (3): 208–15. doi:10.1111/j.1464-410X.1980.tb02961.x. PMID 7000222.
- "Drug Product Database Online Query". 2012-04-25.
- "Drug Product Database Online Query". 2012-04-25.
- "Drug Product Database Online Query". 2012-04-25.
- Kenneth L. Becker (2001). Principles and Practice of Endocrinology and Metabolism. Lippincott Williams & Wilkins. pp. 1004–. ISBN 978-0-7817-1750-2.
- Steinbeck AW (1977). "Of Homosexuality: The Current State of Knowledge". Journal of Christian Education. os-20 (2): 58–82. doi:10.1177/002196577702000204. ISSN 0021-9657. S2CID 149168765.
- Zingg E, König MP, Cornu F, Wildholz A, Blaser A (1980). "Transsexualismus: Erfahrungen mit der operativen Korrektur bei männlichen Transsexuellen" [Transsexualism: Experience with surgical correction in male transsexuals]. Aktuelle Urologie. 11 (2): 67–77. doi:10.1055/s-2008-1062961. ISSN 0001-7868.
- Asscheman H, Gooren LJ (1993). "Hormone Treatment in Transsexuals". Journal of Psychology & Human Sexuality. 5 (4): 39–54. doi:10.1300/J056v05n04_03. ISSN 0890-7064.
- Neumann F, Wiechert R (March 1988). "Das Antiandrogen Cyproteronacetat Seine Geschichte von der Entdeckung bis zur Marktreife" [The antiandrogen cyproterone acetate. Its history from discovery to marketing]. Pharmazie in Unserer Zeit (in German). 17 (2): 33–50. doi:10.1002/pauz.19880170202. ISSN 0048-3664. PMID 2967500.
- Elks J (14 November 2014). The Dictionary of Drugs: Chemical Data: Chemical Data, Structures and Bibliographies. Springer. pp. 339–. ISBN 978-1-4757-2085-3.
- Morton IK, Hall JM (6 December 2012). Concise Dictionary of Pharmacological Agents: Properties and Synonyms. Springer Science & Business Media. pp. 89–. ISBN 978-94-011-4439-1.
- Christoph Zink (1 January 1988). Dictionary of Obstetrics and Gynecology. Walter de Gruyter. pp. 61–. ISBN 978-3-11-085727-6.
- F. William Danby (27 January 2015). Acne: Causes and Practical Management. John Wiley & Sons. pp. 142–. ISBN 978-1-118-23277-4.
- http://www.micromedexsolutions.com/micromedex2/%5B%5D
- Sweetman, Sean C., ed. (2009). "Sex hormones and their modulators". Martindale: The Complete Drug Reference (36th ed.). London: Pharmaceutical Press. p. 2082. ISBN 978-0-85369-840-1.
- Jack H. Mydlo; Ciril J. Godec (11 July 2003). Prostate Cancer: Science and Clinical Practice. Academic Press. pp. 437–. ISBN 978-0-08-049789-1.
- V. Unzeitig; Rick H.W. van Lunsen (15 February 2000). Contraceptive Choices and Realities: Proceedings of the 5th Congress of the European Society of Contraception. CRC Press. pp. 73–. ISBN 978-1-85070-067-8.
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans; World Health Organization; International Agency for Research on Cancer (2007). Combined Estrogen-progestogen Contraceptives and Combined Estrogen-progestogen Menopausal Therapy. World Health Organization. pp. 44, 437. ISBN 978-92-832-1291-1.
- John David Gordon (2007). Obstetrics, Gynecology & Infertility: Handbook for Clinicians. Scrub Hill Press, Inc. pp. 228–. ISBN 978-0-9645467-7-6.
- Matzkin H, Braf Z (January 1991). "Endocrine treatment of benign prostatic hypertrophy: current concepts". Urology. 37 (1): 1–16. doi:10.1016/0090-4295(91)80069-j. PMID 1702565.
- Tenaglia R, Nicolai M, Di Federico G, Iantorno R, Zezza A, Lombardi G (1993). "[Androgen deprivation in benign prostatic hypertrophy]". J Urol (Paris) (in French). 99 (6): 296–8. PMID 7516371.
- Di Silverio F, D'Eramo G, Flammia GP, Buscarini M, Frascaro E, Mariani M, Sciarra A (1993). "[Pharmacological combinations in the treatment of benign prostatic hypertrophy]". J Urol (Paris) (in French). 99 (6): 316–20. PMID 7516378.
- Locker GY (June 1998). "Hormonal therapy of breast cancer". Cancer Treat. Rev. 24 (3): 221–40. doi:10.1016/S0305-7372(98)90051-2. PMID 9767736.
- Willemse PH, Dikkeschei LD, Mulder NH, van der Ploeg E, Sleijfer DT, de Vries EG (March 1988). "Clinical and endocrine effects of cyproterone acetate in postmenopausal patients with advanced breast cancer". Eur J Cancer Clin Oncol. 24 (3): 417–21. doi:10.1016/S0277-5379(98)90011-6. PMID 2968261.
- Nieschlag E (November 2010). "Clinical trials in male hormonal contraception" (PDF). Contraception. 82 (5): 457–70. doi:10.1016/j.contraception.2010.03.020. PMID 20933120.
- Nieschlag, Eberhard; Behre, Hermann M.; Nieschlag, Eberhard; Behre, Hermann M.; Nieschlag, Susan (2012). "The essential role of testosterone in hormonal male contraception". In Nieschlag, Eberhard; Behre, Hermann M; Nieschlag, Susan (eds.). Testosterone. pp. 470–493. doi:10.1017/CBO9781139003353.023. ISBN 9781139003353.
- "Cyproterone acetate - Barr Laboratories - AdisInsight".
- Nguyen Y, Bradford J, Fischer G (February 2018). "Cyproterone acetate in the treatment of oestrogen hypersensitivity vulvovaginitis". The Australasian Journal of Dermatology. 59 (1): 52–54. doi:10.1111/ajd.12657. PMID 28718897. S2CID 22365089.
- Geier DA, Kern JK, King PG, Sykes LK, Geier MR (2012). "An evaluation of the role and treatment of elevated male hormones in autism spectrum disorders". Acta Neurobiol Exp (Wars). 72 (1): 1–17. PMID 22508080.
- Bolea-Alamanac BM, Davies SJ, Christmas DM, Baxter H, Cullum S, Nutt DJ (2011). "Cyproterone to treat aggressivity in dementia: a clinical case and systematic review". J. Psychopharmacol. (Oxford). 25 (1): 141–5. doi:10.1177/0269881109353460. PMID 19942637. S2CID 11479701.
- Albert DJ, Walsh ML, Jonik RH (1993). "Aggression in humans: what is its biological foundation?". Neurosci Biobehav Rev. 17 (4): 405–25. doi:10.1016/S0149-7634(05)80117-4. PMID 8309650. S2CID 28557481.
- Thibaut F, Kuhn JM, Colonna L (August 1991). "A possible antiaggressive effect of cyproterone acetate". Br J Psychiatry. 159 (2): 298–9. doi:10.1192/bjp.159.2.298b. PMID 1837749.
- Nomani H, Mohammadpour AH, Moallem SM, YazdanAbad MJ, Barreto GE, Sahebkar A (December 2019). "Anti-androgen drugs in the treatment of obsessive-compulsive disorder: a systematic review". Curr Med Chem. 27 (40): 6825–6836. doi:10.2174/0929867326666191209142209. PMID 31814547.
- Judith L. Rapoport (1 January 1989). Obsessive-compulsive Disorder in Children and Adolescents. American Psychiatric Pub. pp. 229–231. ISBN 978-0-88048-282-0.
- Kellner M (2010). "Drug treatment of obsessive-compulsive disorder". Dialogues in Clinical Neuroscience. 12 (2): 187–97. doi:10.31887/DCNS.2010.12.2/mkellner. PMC 3181958. PMID 20623923.
- López Ibor JJ, Cercós CL, Masiá CC (2004). Images of Spanish Psychiatry. Editorial Glosa, S.L. pp. 376–. ISBN 978-84-7429-200-8.
- Sicuteri F (1988). "Antiandrogenic medication of cluster headache". Int J Clin Pharmacol Res. 8 (1): 21–4. PMID 3366500.
Further reading
- Neumann F (1971). "Use of cyproterone acetate in animal and clinical trials". Gynecol Invest. 2 (1): 150–79. doi:10.1159/000301860. PMID 4949823.
- Neumann, F.; Steinbeck, H. (1974). Androgens II and Antiandrogens / Androgene II und Antiandrogene. pp. 235–484. doi:10.1007/978-3-642-80859-3_6. ISBN 978-3-642-80861-6.
- Gräf, K.-J.; Brotherton, J.; Neumann, F. (1974). Androgens II and Antiandrogens / Androgene II und Antiandrogene. pp. 485–542. doi:10.1007/978-3-642-80859-3_7. ISBN 978-3-642-80861-6.
- Horn, H. J. (1974). "Administration of Antiandrogens in Hypersexuality and Sexual Deviations". Androgens II and Antiandrogens / Androgene II und Antiandrogene. pp. 543–562. doi:10.1007/978-3-642-80859-3_8. ISBN 978-3-642-80861-6.
- Hammerstein J, Meckies J, Leo-Rossberg I, Moltz L, Zielske F (June 1975). "Use of cyproterone acetate (CPA) in the treatment of acne, hirsutism and virilism". J. Steroid Biochem. 6 (6): 827–36. doi:10.1016/0022-4731(75)90311-8. PMID 126335.
- Neumann F (January 1977). "Pharmacology and potential use of cyproterone acetate". Horm. Metab. Res. 9 (1): 1–13. doi:10.1055/s-0028-1093574. PMID 66176.
- Neumann F (July 1983). "Pharmacological basis for clinical use of antiandrogens". Hormonal Steroids. J. Steroid Biochem. 19. pp. 391–402. doi:10.1016/B978-0-08-030771-8.50055-3. ISBN 9780080307718. PMID 6224971.
- Hammerstein J, Moltz L, Schwartz U (July 1983). "Antiandrogens in the treatment of acne and hirsutism". J. Steroid Biochem. 19 (1B): 591–7. doi:10.1016/0022-4731(83)90223-6. PMID 6224974.
- Miller JA, Jacobs HS (May 1986). "Treatment of hirsutism and acne with cyproterone acetate". Clin Endocrinol Metab. 15 (2): 373–89. doi:10.1016/S0300-595X(86)80031-7. PMID 2941191.
- Neumann F, Wiechert R (March 1988). "Das Antiandrogen Cyproteronacetat: Seine Geschichte von der Entdeckung bis zur Marktreife" [The Antiandrogen Cyproterone Acetate: Its History from Discovery to Marketing]. Pharm Unserer Zeit (in German). 17 (2): 33–50. doi:10.1002/pauz.19880170202. PMID 2967500.
- Tunn UW (1989). "Cyproterone acetate in the management of prostatic cancer". Prog. Clin. Biol. Res. 303: 105–10. PMID 2528734.
- Hammerstein, J. (1990). "Antiandrogens: Clinical Aspects". Hair and Hair Diseases. pp. 827–886. doi:10.1007/978-3-642-74612-3_35. ISBN 978-3-642-74614-7.
- Mowszowicz I (January 1989). "Les antiandrogènes. Mécanismes et effets paradoxaux" [Antiandrogens. Mechanisms and paradoxical effects]. Annales d'Endocrinologie (Paris) (in French). 50 (3): 189–99. ISSN 0003-4266. PMID 2530930.
- Schindler AE (October 1990). "[Anti-androgen therapy in the female]". Geburtshilfe Frauenheilkd (in German). 50 (10): 749–53. doi:10.1055/s-2008-1026359. PMID 1704865.
- de Voogt HJ (1990). "Cyproterone acetate as monotherapy in prospective randomized trials". Prog. Clin. Biol. Res. 359: 85–91, discussion 105–7. PMID 2149459.
- Namer M (October 1988). "Clinical applications of antiandrogens". J. Steroid Biochem. 31 (4B): 719–29. doi:10.1016/0022-4731(88)90023-4. PMID 2462132.
- Goldenberg SL, Bruchovsky N (1991). "Use of cyproterone acetate in prostate cancer". Urol. Clin. North Am. 18 (1): 111–22. PMID 1825143.
- Neumann F, Kalmus J (1991). "Cyproterone acetate in the treatment of sexual disorders: pharmacological base and clinical experience". Exp. Clin. Endocrinol. 98 (2): 71–80. doi:10.1055/s-0029-1211103. PMID 1838080.
- de Voogt HJ (1992). "The position of cyproterone acetate (CPA), a steroidal anti-androgen, in the treatment of prostate cancer". Prostate Suppl. 4: 91–5. doi:10.1002/pros.2990210514. PMID 1533452. S2CID 22747185.
- Schröder FH (1993). "Cyproterone acetate--mechanism of action and clinical effectiveness in prostate cancer treatment". Cancer. 72 (12 Suppl): 3810–5. doi:10.1002/1097-0142(19931215)72:12+<3810::aid-cncr2820721710>3.0.co;2-o. PMID 8252496.
- Barradell LB, Faulds D (1994). "Cyproterone. A review of its pharmacology and therapeutic efficacy in prostate cancer". Drugs Aging. 5 (1): 59–80. doi:10.2165/00002512-199405010-00006. PMID 7919640.
- Neumann F (1994). "The antiandrogen cyproterone acetate: discovery, chemistry, basic pharmacology, clinical use and tool in basic research" (PDF). Exp. Clin. Endocrinol. 102 (1): 1–32. doi:10.1055/s-0029-1211261. PMID 8005205.
- Mahler C, Verhelst J, Denis L (May 1998). "Clinical pharmacokinetics of the antiandrogens and their efficacy in prostate cancer". Clin Pharmacokinet. 34 (5): 405–17. doi:10.2165/00003088-199834050-00005. PMID 9592622. S2CID 25200595.
- Schröder FH (1998). "Antiandrogens as monotherapy for prostate cancer". European Urology. 34 Suppl 3: 12–7. doi:10.1159/000052291. PMID 9854190. S2CID 24831338.
- Diamanti-Kandarakis E (October 1998). "How actual is the treatment with antiandrogen alone in patients with polycystic ovary syndrome?". J. Endocrinol. Invest. 21 (9): 623–9. doi:10.1007/BF03350788. PMID 9856417. S2CID 46484837.
- Diamanti-Kandarakis E (September 1999). "Current aspects of antiandrogen therapy in women". Curr. Pharm. Des. 5 (9): 707–23. PMID 10495361.
- Migliari R, Muscas G, Murru M, Verdacchi T, De Benedetto G, De Angelis M (December 1999). "Antiandrogens: a summary review of pharmacodynamic properties and tolerability in prostate cancer therapy". Arch Ital Urol Androl. 71 (5): 293–302. PMID 10673793.
- Laron Z, Kauli R (2000). "Experience with cyproterone acetate in the treatment of precocious puberty". J. Pediatr. Endocrinol. Metab. 13 Suppl 1: 805–10. doi:10.1515/jpem.2000.13.s1.805. PMID 10969925. S2CID 25398066.
- Reilly DR, Delva NJ, Hudson RW (August 2000). "Protocols for the use of cyproterone, medroxyprogesterone, and leuprolide in the treatment of paraphilia". Can J Psychiatry. 45 (6): 559–63. doi:10.1177/070674370004500608. PMID 10986575.
- Anderson J (March 2003). "The role of antiandrogen monotherapy in the treatment of prostate cancer". BJU Int. 91 (5): 455–61. doi:10.1046/j.1464-410X.2003.04026.x. PMID 12603397. S2CID 8639102.
- Van der Spuy ZM, le Roux PA (2003). "Cyproterone acetate for hirsutism". Cochrane Database Syst Rev (4): CD001125. doi:10.1002/14651858.CD001125. PMID 14583927.
- Zouboulis CC (July 2003). "Therapie der Akne mit Antiandrogenen – Eine evidenzbasierte Übersicht" [Treatment of acne with antiandrogens--an evidence-based review]. J Dtsch Dermatol Ges (in German). 1 (7): 535–46. doi:10.1046/j.1610-0387.2003.03011.x. PMID 16295039. S2CID 71005143.
- Thole Z, Manso G, Salgueiro E, Revuelta P, Hidalgo A (2004). "Hepatotoxicity induced by antiandrogens: a review of the literature". Urol. Int. 73 (4): 289–95. doi:10.1159/000081585. PMID 15604569. S2CID 24799765.
- Sciarra A, Cardi A, Di Silverio F (2004). "Antiandrogen monotherapy: recommendations for the treatment of prostate cancer". Urol. Int. 72 (2): 91–8. doi:10.1159/000075960. PMID 14963347. S2CID 24203925.
- Torri V, Floriani I (2005). "Cyproterone acetate in the therapy of prostate carcinoma". Arch Ital Urol Androl. 77 (3): 157–63. CiteSeerX 10.1.1.663.9458. PMID 16372511.
- Schröder, Fritz H.; Radlmaier, Albert (2009). "Steroidal Antiandrogens". In V. Craig Jordan; Barrington J. A. Furr (eds.). Hormone Therapy in Breast and Prostate Cancer. Humana Press. pp. 325–346. doi:10.1007/978-1-59259-152-7_15. ISBN 978-1-60761-471-5.
- Gillatt D (August 2006). "Antiandrogen treatments in locally advanced prostate cancer: are they all the same?". J. Cancer Res. Clin. Oncol. 132 Suppl 1: S17–26. doi:10.1007/s00432-006-0133-5. PMID 16845534. S2CID 23888640.
- Bachelot A, Chabbert-Buffet N, Salenave S, Kerlan V, Galand-Portier MB (February 2010). "Anti-androgen treatments". Ann. Endocrinol. (Paris). 71 (1): 19–24. doi:10.1016/j.ando.2009.12.001. PMID 20096826.
- Zouboulis CC, Rabe T (March 2010). "Hormonelle Antiandrogene in der Aknetherapie" [Hormonal antiandrogens in acne treatment]. J Dtsch Dermatol Ges (in German). 8 Suppl 1: S60–74. doi:10.1111/j.1610-0387.2009.07171.x. PMID 20482693. S2CID 196375064.
- Bolea-Alamanac BM, Davies SJ, Christmas DM, Baxter H, Cullum S, Nutt DJ (January 2011). "Cyproterone to treat aggressivity in dementia: a clinical case and systematic review". J. Psychopharmacol. (Oxford). 25 (1): 141–5. doi:10.1177/0269881109353460. PMID 19942637. S2CID 11479701.
- Kim JH, Yoo BW, Yang WJ (May 2014). "Hepatic failure induced by cyproterone acetate: A case report and literature review". Can Urol Assoc J. 8 (5–6): E458–61. doi:10.5489/cuaj.1753. PMC 4081269. PMID 25024808.
- Bitzer J, Römer T, Lopes da Silva Filho A (June 2017). "The use of cyproterone acetate/ethinyl estradiol in hyperandrogenic skin symptoms - a review". Eur J Contracept Reprod Health Care. 22 (3): 172–182. doi:10.1080/13625187.2017.1317339. PMID 28447864.
- Ruan X, Kubba A, Aguilar A, Mueck AO (June 2017). "Use of cyproterone acetate/ethinylestradiol in polycystic ovary syndrome: rationale and practical aspects". Eur J Contracept Reprod Health Care. 22 (3): 183–190. doi:10.1080/13625187.2017.1317735. PMID 28463030.
External links
- Die Geschichte des Wirkstoffs Cyproteronazetat: Von der "Pille für den Mann" zum "Hautpflegemittel mit Empfängnisschutz" [The History of Cyproterone Acetate: From the "Pill for Men" to the "Skin Care Product and Contraceptive"] - Arznei-Telegramm (in German) [Google Translate]