Ethinylestradiol sulfonate
Ethinylestradiol sulfonate (EES), sold under the brand names Deposiston and Turisteron among others, is an estrogen medication which has been used in birth control pills for women and in the treatment of prostate cancer in men.[1][5][2][3][6] It has also been investigated in the treatment of breast cancer in women.[4][7] The medication was combined with norethisterone acetate in birth control pills.[1] EES is taken by mouth once per week.[1][5][2][3]
 | |
 | |
| Clinical data | |
|---|---|
| Trade names | Deposiston, Turisteron[1] |
| Other names | EES; Turisteron; J96; Ethinylestradiol 3-isopropylsulfonate; Ethinylestradiol 3-(2-propanesulfonate); 17α-Ethynyl-3-isopropyl-sulfonyloxyestradiol |
| Routes of administration | By mouth[2][3] |
| Drug class | Estrogen; Estrogen ester |
| Pharmacokinetic data | |
| Metabolites | • Ethinylestradiol[2][3] |
| Elimination half-life | Oral: 6 days[4] |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| CompTox Dashboard (EPA) | |
| Chemical and physical data | |
| Formula | C23H30O4S |
| Molar mass | 402.55 g·mol−1 |
| 3D model (JSmol) | |
| |
| |
Side effects of EES in men include breast tenderness, gynecomastia, feminization, sexual dysfunction, and cardiovascular complications, among others.[5][2] EES is a synthetic estrogen and hence is an agonist of the estrogen receptor, the biological target of estrogens like estradiol.[2][3] It is an estrogen ester and a long-lasting prodrug of ethinylestradiol in the body.[2][3] EES is rapidly taken up into fat and slowly released from it, resulting in a biological half-life of about 6 days with the oral route and allowing the medication to be taken only once per week.[2][4]
EES was first synthesized in 1967, was first introduced as a birth control pill in 1978, and was introduced for the treatment of prostate cancer in 1980.[1][3] It has been marketed in Germany, but may no longer be available.[8][9][10]
Medical uses
EES has been used in combination with norethisterone acetate as a once-a-week birth control pill and by itself as a form of high-dose estrogen therapy in the treatment of prostate cancer.[1][5][3][6][11] It has also been assessed in the treatment of breast cancer.[4][7] The medication is used at a dosage of 1 mg once per week in birth control pills and 1 to 2 mg once per week in the treatment of prostate cancer.[12][5][2] The 1 week and 2 mg/week dosages of EES are equivalent to daily doses of 0.143 mg and 0.285 mg EES, respectively.[13]
EES has been used in combination with antiandrogens such as flutamide, bicalutamide, and cyproterone acetate as a form of combined androgen blockade and as an alternative to the combination of an antiandrogen and surgical or medical castration in the treatment of prostate cancer.[13]
Available forms
EES was available alone for the treatment of prostate cancer in men in the form of 1 mg oral tablets[14][15] and in combination with norethisterone acetate in the form of oral tablets containing 1 mg EES and 5 mg norethisterone acetate for use as a birth control pill for women.[15][16][1]
Side effects
Side effects of EES in men include breast tenderness, gynecomastia, feminization, sexual dysfunction, shortness of breath (6.8%), increased prolactin levels, and cardiovascular toxicity.[5][2] The cardiovascular complications of EES in men with prostate cancer specifically include edema (4.5 to 26%), blood clots like deep vein thrombosis (4.1 to 15%) and pulmonary embolism, heart attack (2.3 to 18%), stroke (2.3 to 3.0%), and coronary artery disease (3.3%).[5][2]
EES has been described as having good tolerability compared to EE in the treatment of prostate cancer, a property that has been described as "remarkable".[2] The unique C3 sulfonate ester of EES seems to reduce its hepatic estrogenicity, which in turn reduces its adverse effects on liver protein synthesis.[2] In particular, EES is said to have considerably reduced cardiovascular side effects relative to EE when used as a form of high-dose estrogen therapy in the treatment of prostate cancer.[2] This may in part be related to the greatly reduced oral dosing frequency of EES relative to EE, as parenteral EE, which bypasses the first pass through the liver that occurs with oral EE, has been found to have a 5-fold lower impact on liver protein synthesis by weight than oral EE.[2] Conversely however, studies with EE-containing contraceptive vaginal rings and contraceptive patches have shown similar metabolic effects and VTE risk as combined birth control pills containing EE.[17][18][19]
Pharmacology
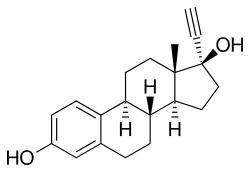
EES is an estrogen ester and long-acting prodrug of ethinylestradiol (EE) which is taken orally.[2][3] The molecular weight of EES is about 136% of that of EE due to the presence of its C3 isopropylsulfonate ester, and hence EES contains about 74% of the amount of EE of an equal dose of EE.[20][8] EES is more lipophilic than EE, and this results in a depot effect in which EES is taken up into fat and then slowly released from it.[2] Following its release from fat, EES is hydrolyzed into EE.[2] As a result of this depot effect, EES has a very long elimination half-life of about 6 days.[4] This allows it to be taken once per week.[3][2] Both EES and the related medication quinestrol have been described as depot oral estrogens.[1][12][2]
EES is a powerful antigonadotropin, and is capable of suppressing circulating total testosterone levels in men to concentrations comparable to those seen with castration (less than 1 to 3% of initial values).[6][21][11] In addition, EES can strongly increase sex hormone-binding globulin (SHBG) levels, thereby additionally decreasing free testosterone levels.[5][22][23][21] As such, EES is a powerful functional antiandrogen, which makes it useful for treating prostate cancer.[24][21]
The biological half-life of EES in blood has been reported to be 3 hours.[14]
Chemistry
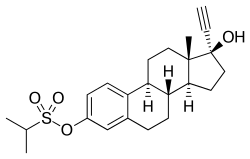
EES, also known as ethinylestradiol 3-isopropylsulfonate or ethinylestradiol 3-(2-propanesulfonate), is a synthetic estrane steroid and a derivative of estradiol. Specifically, it is the C3 isopropylsulfonate ester of ethinylestradiol (17α-ethynylestradiol).[20][8][2] EES is similar to quinestrol (EE 3-cyclopentyl ether), which is a C3 ether of EE and is a long-lasting oral depot estrogen similarly.[2]
Analogues of EES include ethinylestradiol N,N-diethylsulfamate (J271) and ethinylestradiol pyrrolidinosulfamate (J272).[3] These analogues are rapidly taken up by erythrocytes in the blood of the hepatic portal vein during the first pass with oral administration, and have been found to be much stronger oral estrogens than EE or EES.[3] EE and EES themselves do not have affinity for erythrocytes.[3] EES and related C3 sulfur-containing esters of EE led to the development of estrogen sulfamates like estradiol 3-sulfamate (J995), estriol 3-sulfamate (J1034), and estradiol 17β-(1-(4-(aminosulfonyl)benzoyl)-L-proline) (EC508), which are highly potent oral estradiol prodrugs that bind to erythrocytes similarly and are under investigation for potential clinical use.[1][2][3][25][26]
History
EES was first synthesized in 1967 at Jenapharm.[1][3] It was first introduced for use in combination with norethisterone acetate under the brand name Deposiston as a once-a-week birth control pill for women in 1978.[1] The medication was subsequently introduced by itself under the brand name Turisteron for the treatment of prostate cancer in men in 1980.[1]
Society and culture
Generic names
Ethinylestradiol sulfonate is the generic name of the drug, but it is also commonly known by its brand names Deposiston and Turisteron.[1][20][8] It does not appear to have an INN or other such designations.[20][8] EES has also been known by its former developmental code name J96.[3]
Brand names
EES has been marketed in combination with norethisterone acetate under the brand name Deposiston for use as a birth control pill in women and under the brand name Turisteron for use in prostate cancer in men.[1][20][8]
References
- Schwarz S, Onken D, Schubert A (July 1999). "The steroid story of Jenapharm: from the late 1940s to the early 1970s". Steroids. 64 (7): 439–45. doi:10.1016/S0039-128X(99)00003-3. PMID 10443899. S2CID 40156824.
6.2. New estrogens. In 1967, Jenapharm, in conjunction with the Academy of Sciences (Kurt Ponsold, Gu¨nter Bruns, and Kurt Schubert in Jena and Hans Schick and Bernard Lu¨cke in Berlin), started a program of searching for new estrogens. [...] orally administered, strongly active estrogens with a depot effect. [...] the second objective was successfully attained. The rationale that an a-branched alkanesulfonic acid ester of ethinyl estradiol with a medium chain length should lead to a depot effect without the danger of active ingredient accumulation on longer usage [15] led in 1978 to the first once-a-week oral contraceptive (DEPOSISTONt), a combination of ethinylestradiol 3-isopropylsulfonate (17) and norethisterone acetate [16]. TURISTERONt, an estrogenic monotherapy with compound 17 that can still justify its position today [17], followed in 1980, as a therapy of prostate cancer. [...]
- Michael Oettel; Ekkehard Schillinger (6 December 2012). Estrogens and Antiestrogens II: Pharmacology and Clinical Application of Estrogens and Antiestrogen. Springer Science & Business Media. pp. 248, 277, 369, 540, 542. doi:10.1007/978-3-642-60107-1. ISBN 978-3-642-60107-1. S2CID 35733673.
- Elger W, Palme HJ, Schwarz S (April 1998). "Novel oestrogen sulfamates: a new approach to oral hormone therapy". Expert Opin Investig Drugs. 7 (4): 575–89. doi:10.1517/13543784.7.4.575. PMID 15991994.
- Gürtler R, Tanneberger S, Bodek B, Morack G (1982). "[Clinical experience with the depot estrogen Turisteron in the treatment of metastatic breast cancer (author's transl)]". Arch. Geschwulstforsch. (in German). 52 (2): 129–39. PMID 7103689.
- Höfling, G.; Heynemann, H. (1998). "Die orale Östrogentherapie des fortgeschrittenen Prostatakarzinoms — Anlaß für eine Neubewertung?" [Oral Estrogen Therapy for Advanced Prostate Cancer — Reason for Revaluation?]. Der Urologe B. 38 (2): 165–170. doi:10.1007/s001310050185. ISSN 0042-1111.
- Dörner G, Schnorr D, Stahl F, Rohde W (December 1985). "Successful treatment of prostatic cancer with the orally active depot estrogen ethinylestradiol sulfonate (Turisteron)". Exp. Clin. Endocrinol. 86 (2): 190–6. doi:10.1055/s-0029-1210486. PMID 3912197.
- S. Monfardini; K. Brunner; D. Crowther; S. Eckhardt; D. Olive; S. Tanneberger; A. Veronesi; J.M.A. Whitehouse; R. Wittes (1987). Manual of Adult and Paediatric Medical Oncology. Springer Science & Business Media. pp. 196–. doi:10.1007/978-3-642-82489-0. ISBN 978-3-642-82489-0. S2CID 35835002.
- Index Nominum 2000: International Drug Directory. Taylor & Francis. January 2000. pp. 412–. ISBN 978-3-88763-075-1.
- Sweetman, Sean C., ed. (2009). "Sex hormones and their modulators". Martindale: The Complete Drug Reference (36th ed.). London: Pharmaceutical Press. p. 2102. ISBN 978-0-85369-840-1.
- https://www.drugs.com/international/turisteron.html
- Stahl F, Schnorr D, Bär CM, Fröhlich G, Dörner G (1989). "Suppression of plasma androgen levels with a combination therapy of depot-estrogen (Turisteron) and Dexamethasone in patients with prostatic cancer". Exp. Clin. Endocrinol. 94 (3): 239–43. doi:10.1055/s-0029-1210905. PMID 2630306.
- Göretzlehner G, Köhler G (1990). "Charakteristik der Estrogene und Gestagene" [Characteristics of estrogens and gestagens]. Z Arztl Fortbild (Jena) (in German). 84 (1–2): 7–12. ISSN 0012-0219. PMID 2184606.
- Wolfgang Hinkelbein; Kurt Miller; Thomas Wiegel (7 March 2013). Prostatakarzinom — urologische und strahlentherapeutische Aspekte: urologische und strahlentherapeutische Aspekte [Prostate carcinoma — urological and radiotherapeutic aspects: urological and radiotherapeutic aspects]. Springer-Verlag. pp. 92–93, 99. ISBN 978-3-642-60064-7.
- Benno Runnebaum; Thomas Rabe (17 April 2013). Gynäkologische Endokrinologie und Fortpflanzungsmedizin: Band 1: Gynäkologische Endokrinologie. Springer-Verlag. pp. 88–. ISBN 978-3-662-07635-4.
- Freimut A. Leidenberger (2 July 2013). Klinische Endokrinologie für Frauenärzte. Springer-Verlag. pp. 542, 644–. ISBN 978-3-662-08108-2.
- Muller (19 June 1998). European Drug Index: European Drug Registrations, Fourth Edition. CRC Press. pp. 338–. ISBN 978-3-7692-2114-5.
- Pfeifer, Samantha; Butts, Samantha; Dumesic, Daniel; Fossum, Gregory; Gracia, Clarisa; La Barbera, Andrew; Mersereau, Jennifer; Odem, Randall; Penzias, Alan; Pisarska, Margareta; Rebar, Robert; Reindollar, Richard; Rosen, Mitchell; Sandlow, Jay; Sokol, Rebecca; Vernon, Michael; Widra, Eric (January 2017). "Combined hormonal contraception and the risk of venous thromboembolism: a guideline". Fertil. Steril. 107 (1): 43–51. doi:10.1016/j.fertnstert.2016.09.027. PMID 27793376.
- Plu-Bureau G, Maitrot-Mantelet L, Hugon-Rodin J, Canonico M (February 2013). "Hormonal contraceptives and venous thromboembolism: an epidemiological update". Best Pract. Res. Clin. Endocrinol. Metab. 27 (1): 25–34. doi:10.1016/j.beem.2012.11.002. PMID 23384743.
- Sitruk-Ware R, Nath A (June 2011). "Metabolic effects of contraceptive steroids". Rev Endocr Metab Disord. 12 (2): 63–75. doi:10.1007/s11154-011-9182-4. PMID 21538049. S2CID 23760705.
- J. Elks (14 November 2014). The Dictionary of Drugs: Chemical Data: Chemical Data, Structures and Bibliographies. Springer. pp. 523–. ISBN 978-1-4757-2085-3.
- Guddat HM, Schnorr D, Dörner G, Stahl F, Rohde W (December 1987). "[Behavior of LH, FSH, total testosterone, free testosterone and SHBG serum levels in the therapy of prostatic cancer with Turisteron (ethinyl estradiol sulfonate)]". Z Urol Nephrol (in German). 80 (12): 665–8. PMID 3126615.
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans; World Health Organization; International Agency for Research on Cancer (2007). Combined Estrogen-progestogen Contraceptives and Combined Estrogen-progestogen Menopausal Therapy. World Health Organization. pp. 157–. ISBN 978-92-832-1291-1.
- Stephen J. Winters; Ilpo T. Huhtaniemi (25 April 2017). Male Hypogonadism: Basic, Clinical and Therapeutic Principles. Humana Press. pp. 307–. ISBN 978-3-319-53298-1.
- Schnorr D, Dörner G, Stahl F, Rohde W, Guddat HM (1987). "[Conservative therapy of prostate cancer using Turisteron]". Z Urol Nephrol (in German). 80 (3): 149–57. PMID 3111122.
- Elger W, Barth A, Hedden A, Reddersen G, Ritter P, Schneider B, Züchner J, Krahl E, Müller K, Oettel M, Schwarz S (2001). "Estrogen sulfamates: a new approach to oral estrogen therapy". Reprod. Fertil. Dev. 13 (4): 297–305. doi:10.1071/RD01029. PMID 11800168.
- Elger W, Wyrwa R, Ahmed G, Meece F, Nair HB, Santhamma B, Killeen Z, Schneider B, Meister R, Schubert H, Nickisch K (January 2017). "Estradiol prodrugs (EP) for efficient oral estrogen treatment and abolished effects on estrogen modulated liver functions". J. Steroid Biochem. Mol. Biol. 165 (Pt B): 305–311. doi:10.1016/j.jsbmb.2016.07.008. PMID 27449818. S2CID 26650319.
Further reading
- Höfling, G.; Heynemann, H. (2014). "Die orale Östrogentherapie des fortgeschrittenen Prostatakarzinoms — Anlaß für eine Neubewertung?" [Oral Estrogen Therapy for Advanced Prostate Cancer — Reason for Revaluation?]. Der Urologe B. 38 (2): 165–170. doi:10.1007/s001310050185. ISSN 0042-1111.