Perineal massage
Antenatal perineal massage (APM) or birth canal widening (BCW) is the massage of a pregnant woman's perineum around the opening to the vagina, performed anywhere in the 4 to 6 weeks before childbirth and usually on 4-6 separate occasions. The practice aims to more gently mimic the massaging action of a baby's head on the opening to the birth canal prior to birth, which enables some of the hard work of labour to be done before the start of labour. The intention is to attempt to prevent tearing of the perineum during birth, and reduce the need for an episiotomy or an instrument (forceps or vacuum extraction) delivery.
Description
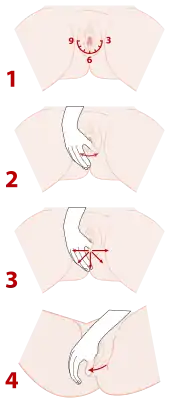
The Oxford Radcliffe NHS Trust Document "Antenatal Perineal Massage" 2011 describes the use of the pregnant mother's thumbs being placed just inside the birth canal, whilst she stands with one foot supported on the toilet.[1][2] She pulls backwards towards her spine, whilst relaxing her pelvic floor, progressively increasing the pressure under her finger tips until this starts to feel uncomfortable. On the next occasion she uses both thumbs pulling backwards and then sideways, thumbs away from each other, to enlarge the 2 cm diameter opening of the birth canal progressively over time to 10 cm. by progressing to use the four fingers of both hands pulling away from each other, painlessly- to avoid causing tearing. It is not possible to stretch this opening further, because this will be limited by the distance between the bony walls of the pelvis.
Purposes
The goal of APM is to prevent the baby's head from undergoing excessive strain during the last 30 minutes of labour. It seeks to train the mother to relax her pelvic floor to allow the baby's head to pass through the opening, to stretch the two fibrous layers within the Uro-Genital Membrane, a triangular shaped muscular shelf at the front half of the opening of the bony pelvis, through which the 2 cm diameter birth canal and urethra pass, and to transform the fat packed rigid skin at the opening to the birth canal into paper thin stretchy elastic skin, all without using the baby's head.[3]
If the external skin (perineal skin) opening has been stretched before birth, to 10 cm, then there is no reason to perform an episiotomy to increase the diameter of the opening of the birth canal. Tearing is less likely as the external skin at the opening has been stretched already and is lax, whilst the underlying muscular pelvic floor has not been damaged. Episiotomy permanently damages the pelvic floor muscle, as the episiotomy cuts through the nerve supply to this muscle, so the larger part of the pelvic floor muscles atrophies and becomes replaced by scar tissue, increasing the mother's chance of developing a prolapse in the future. Antenatal Perineal Massage does not damage the pelvic floor, so protects against a prolapse.[4]
History
Antenatal perineal massage or pre-birth obstetric massage (birth canal widening) was reportedly used by African tribal people.[5] The German obstetrician Mr Welheim Horkel, when visiting a medical mission in the mid-1980s, learned that African tribes used gourds of increasing sizes to stretch the perineum.[5] He replicated this in a hospital setting using an inflatable silicone balloon.[5]
West Berkshire England performed an Antenatal Massage trial in 1984, and many small trials have been performed worldwide since. Cochrane Collaborate Reports since 2006 have advised that women should be informed that episiotomy is avoidable if they employ digital Antenatal Perineal Massage.[6]
Effectiveness

A randomized clinical trials of perineal massage (only) during the second stage of labour found similar results in the massage and control groups. They found a tendency for reduced third degree tears, but did not study enough women to be able to determine whether this tendency was statistically meaningful because such tears are generally not very frequent. No meaningful differences were found for intact perineums, first and second degree tears, the risk of pain, urinary or fecal incontinence, or dyspareunia.[7]
For the trial titled 'The possibility of antepartal prevention of episiotomy and perineal tears during delivery', 315 primiparous women were questioned between February 2014 and November 2015 after a vaginal delivery, on the use of methods of birth injury prevention: vaginal dilatators EPI-NO and Aniball, perineal massage, natural methods (raspberry-leaf tea or linseed). The authors concluded that 'There was a significantly higher number of women with intact perineum after the use of vaginal dilatators (43.1% vs.14.1% in control group (p < 0.001)' and 'We also found a significant reduction of episiotomies in this group (29.3% vs. 57.7%, p < 0.001).[8]
Antenatal Perineal Massage affords mothers worldwide, irrespective of income, the opportunity to shorten the critical last 30 minutes of labour.[9] Mothers with a narrowed opening in their bony pelvis, whether from being born with an abnormally narrow pelvis, from previous fracture or from deformity secondary to infection in the bone (osteomyelitis), may need surgical intervention, as indicated by a failure to progress either when the baby's head fails to enter the bony pelvis or develops fetal distress.
References
- "Promoting Effective Recovery from Labor".
- "The Oxford Radcliffe NHS Trust Document "Antenatal Perineal Massage" information document for women" (PDF).
- "Pelvic Floor Part2".
- Avery M (1986). "Effect of Perineal Massage on the incidence of episiotomy and perineal laceration 1986". Journal of Nurse-Midwifery. 31 (3): 128–134. doi:10.1016/0091-2182(86)90148-5. PMID 3635585.
- "Epi-no story Inspired by an African experience". Archived from the original on 2010.
- Beckmann, Michael M; Stock, Owen M (2013-04-30). "Antenatal perineal massage for reducing perineal trauma". Cochrane Database of Systematic Reviews (4): CD005123. doi:10.1002/14651858.CD005123.pub3. ISSN 1465-1858. PMID 23633325.
- Stamp, Georgina; Kruzins, Gillian; Crowther, Caroline (2001-05-26). "Perineal massage in labour and prevention of perineal trauma: randomised controlled trial". BMJ : British Medical Journal. 322 (7297): 1277–1280. doi:10.1136/bmj.322.7297.1277. ISSN 0959-8138. PMC 31922. PMID 11375230.
- 'Retrospective study at Nemocnice Český Krumlov: Dostálek L, Bohatá P (2016-08-01). "'Antepartální možnosti prevence epiziotomie a ruptury hráze při porodu': Randomised control trial". Čes. Gynek 81, č. 3, S. 192–201. – The Journal of Obstetrics and Gynaecology of Czechoslovakia
- Geranmayeh, Mehrnaz; Rezaei Habibabadi, Zahra; Fallahkish, Bijan; Farahani, Mahdi Azizabadi; Khakbazan, Zohreh; Mehran, Abbas (2011-05-26). "Reducing perineal trauma through perineal massage with vaseline in second stage of labor". Archives of Gynecology and Obstetrics. 285 (1): 77–81. doi:10.1007/s00404-011-1919-5. ISSN 0932-0067. PMID 21614497. S2CID 19063469.