Risser sign
The Risser sign is an indirect measure of skeletal maturity, whereby the degree of ossification of the iliac apophysis by x-ray evaluation is used to judge overall skeletal development. Mineralization of the iliac apophyses begins at the anterolateral crest and progresses medially towards the spine. Fusion of the calcified apophyses to the ilium then progresses in opposite direction, from medial-to-lateral.[1]
| Pelvis | |
|---|---|
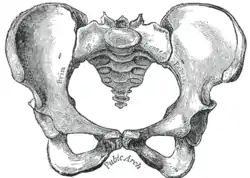 Female type pelvis | |
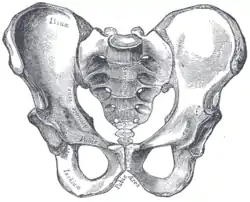 Male type pelvis | |
| Anatomical terms of bone |
A typical five-point grading scale is as follows:
- Grade 1 is given when the ilium (bone) is calcified at a level of 25%; it corresponds to prepuberty or early puberty.
- Grade 2 is given when the ilium (bone) is calcified at a level of 50%; it corresponds to the stage before or during growth spurt.
- Grade 3 is given when the ilium (bone) is calcified at a level of 75%; it corresponds to the slowing of growth.
- Grade 4 is given when the ilium (bone) is calcified at a level of 100%; it corresponds to an almost cessation of growth.
- Grade 5 is given when the ilium (bone) is calcified at a level of 100% and the iliac apophysis is fused to iliac crest; it corresponds to the end of growth.
Risser grading is traditionally used to estimating the future growth potential of the adolescent spine, particularly in the setting of spinal scoliosis. Risser originally recognized that ossification of the iliac apophyses approximately parallels the ossification of the vertebral apophyses. The earlier the stage of growth, the greater the likelihood of a scoliosis progressing and potentially needing intervention.[2] Note that although Risser first described his findings during a 1948 lecture[3] and published the eponymous paper in 1958,[4] formalized staging systems were developed at a later time.
Controversy
The Risser grading system has been criticized as being an inaccurate proxy for skeletal maturity. Comparison of predicted future growth and progression of scoliosis to actual measured changes show that the Risser system is variably accurate.[5] Specifically, because the progression from stages 1 to 4 (apophyseal "excursion") is rapid and only takes an average of approximately 1 year, these stages are of limited value in pinpointing stage of growth. Cessation of trunk growth as predicted by Risser stage is also earlier than actual growth.[5]
In 2008, Sanders et al proposed an alternative system for assessing skeletal maturity, using hand x-rays in a manner similar to "gold standards" (Greulich and Pyle, Tanner-Whitehouse-III) skeletal maturity assessments.[6] Whether the use of the Sanders vs Risser staging for management of scoliosis would lead to different treatment decisions is being debated.[7]
References
- Waldt, Simone; Woertler, Klaus (2014). Measurements and Classifications in Musculoskeletal Radiology. Thieme. pp. 126–127. ISBN 978-3-13-169271-9.
- http://www.aafp.org/afp/2002/0501/p1817.html
- Risser JC. Important practical facts in the treatment of scoliosis. Instr Course Lect 1948;V:248-260.
- Risser, J. C. (1958-01-01). "The Iliac apophysis; an invaluable sign in the management of scoliosis". Clinical Orthopaedics. 11: 111–119. ISSN 0095-8654. PMID 13561591.
- Little, David G.; Sussman, Michael D. (September 1994). "The Risser Sign: A Critical Analysis". Journal of Pediatric Orthopaedics. 14 (5): 569–75. doi:10.1097/01241398-199409000-00003. ISSN 0271-6798. PMID 7962495.
- Sanders, James O.; Khoury, Joseph G.; Kishan, Shyam; Browne, Richard H.; Mooney, James F.; Arnold, Kali D.; McConnell, Sharon J.; Bauman, Jeanne A.; Finegold, David N. (March 2008). "Predicting scoliosis progression from skeletal maturity: a simplified classification during adolescence". The Journal of Bone and Joint Surgery. American Volume. 90 (3): 540–553. doi:10.2106/JBJS.G.00004. ISSN 1535-1386. PMID 18310704.
- Minkara, Anas; Bainton, Nicole; Tanaka, Masashi; Kung, Justin; DeAllie, Christopher; Khaleel, Alexandra; Matsumoto, Hiroko; Vitale, Michael; Roye, Benjamin (2018-01-22). "High Risk of Mismatch Between Sanders and Risser Staging in Adolescent Idiopathic Scoliosis: Are We Guiding Treatment Using the Wrong Classification?". Journal of Pediatric Orthopedics: 1. doi:10.1097/BPO.0000000000001135. ISSN 1539-2570. PMID 29360659.