Subglottic stenosis
Subglottic stenosis is a congenital or acquired narrowing of the subglottic airway.[1] Although it is relatively rare, it is the third most common congenital airway problem (after laryngomalacia and vocal cord paralysis). Subglottic stenosis can present as a life-threatening airway emergency. It is imperative that the otolaryngologist be an expert at dealing with the diagnosis and management of this disorder. Subglottic stenosis can affect both children and adults.
| Subglottic stenosis | |
|---|---|
.jpg.webp) | |
| Neck AP x-ray of patient with post-intubation subglottic stenosis, as shown by the narrowing in the tracheal lumen marked by the arrow. | |
| Specialty | Pulmonology |
Types
Subglottic stenosis can be of three forms, namely congenital subglottic stenosis, idiopathic subglottic stenosis (ISS) and acquired subglottic stenosis. As the name suggests, congenital subglottic stenosis is a birth defect. Idiopathic subglottic stenosis is a narrowing of the airway due to an unknown cause. Acquired subglottic stenosis generally follows as an after-effect of airway intubation, and in extremely rare cases as a result of gastroesophageal reflux disease (GERD).
Diagnosis
Subglottic stenosis is graded according to the Cotton-Myer classification system from one to four based on the severity of the blockage.[2]
Grade 1 – <50% obstruction
Grade 2 – 51–70% obstruction
Grade 3 – 71–99% obstruction
Grade 4 – no detectable lumen
Management
Treatments to alleviate the symptoms of subglottic stenosis includes a daily dose of steroids such as prednisone, which reduces the inflammation of the area for better breathing. Other medications such as Methotrexate is also being tested by patients but results are pending.
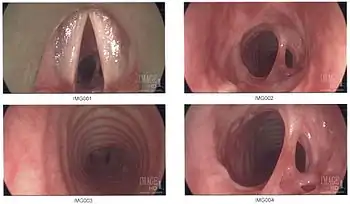
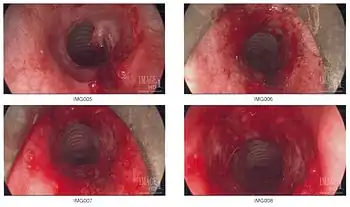
Additional images
References
- "Subglottic Stenosis in Adults: Problem, Etiology, Pathophysiology". 2017-06-21. Cite journal requires
|journal=(help) - Myer Cm, 3rd; O'Connor, D. M.; Cotton, R. T. (April 1994). "Proposed grading system for subglottic stenosis based on endotracheal tube sizes". The Annals of Otology, Rhinology, and Laryngology. 103 (4 Pt 1): 319–23. doi:10.1177/000348949410300410. PMID 8154776. S2CID 12782910.