Trastuzumab
Trastuzumab, sold under the brand name Herceptin among others, is a monoclonal antibody used to treat breast cancer and stomach cancer.[3][4][5][6] It is specifically used for cancer that is HER2 receptor positive.[3] It may be used by itself or together with other chemotherapy medication.[3] Trastuzumab is given by slow injection into a vein and injection just under the skin.[3][7]
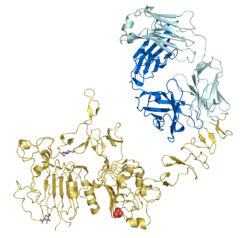 Trastuzumab Fab region (cyan) binding HER2/neu (gold) | |
| Monoclonal antibody | |
|---|---|
| Type | Whole antibody |
| Source | Humanized (from mouse) |
| Target | HER2/neu |
| Clinical data | |
| Trade names | Herceptin, Herzuma, Ogivri, others[1] |
| Other names | trastuzumab-anns, trastuzumab-dkst, trastuzumab-dttb, trastuzumab-pkrb, trastuzumab-qyyp |
| AHFS/Drugs.com | Monograph |
| License data |
|
| Pregnancy category |
|
| Routes of administration | Intravenous, subcutaneous |
| Drug class | Antineoplastic agent |
| ATC code | |
| Legal status | |
| Legal status | |
| Pharmacokinetic data | |
| Metabolism | Unknown, possibly reticuloendothelial system. |
| Elimination half-life | 2-12 days |
| Identifiers | |
| CAS Number | |
| PubChem SID | |
| DrugBank | |
| ChemSpider |
|
| UNII | |
| KEGG | |
| ChEMBL | |
| ECHA InfoCard | 100.224.377 |
| Chemical and physical data | |
| Formula | C6470H10012N1726O2013S42 |
| Molar mass | 145531.86 g·mol−1 |
| | |
Common side effects include fever, infection, cough, headache, trouble sleeping, and rash.[3] Other severe side effects include heart failure, allergic reactions, and lung disease.[3] Use during pregnancy may harm the baby.[2] Trastuzumab works by binding to the HER2 receptor and slowing down cell duplication.[3]
Trastuzumab was approved for medical use in the United States in September 1998, and in the European Union in August 2000.[8][6] It is on the World Health Organization's List of Essential Medicines.[9] A biosimilar was approved in the European Union in November 2017, and in the United States in December 2018.[10][11][12]
Medical uses
The safety and efficacy of trastuzumab-containing combination therapies (with chemotherapy, hormone blockers, or lapatinib) for the treatment of metastatic breast cancer. The overall hazard ratios for overall survival and progression free survival were 0.82 and 0.61, respectively. It was difficult to accurately ascertain the true impact of trastuzumab on survival, as in three of the seven trials, over half of the patients in the control arm were allowed to cross-over and receive trastuzumab after their cancer began to progress.[13] Thus, this analysis likely underestimates the true survival benefit associated with trastuzumab treatment in this population.[14] In these trials, trastuzumab also increased the risk of heart problems, including heart failure and left ventricular ejection fraction decline.
In early-stage HER2-positive breast cancer, trastuzumab-containing regimens improved overall survival (HR = 0.66) and disease-free survival (HR = 0.60). Increased risk of heart failure (RR = 5.11) and decline in left ventricular ejection fraction (RR = 1.83) were seen in these trials as well. Two trials involving shorter term treatment with trastuzumab did not differ in efficacy from longer trials, but produced less cardiac toxicity.[15]
The original studies of trastuzumab showed that it improved overall survival in late-stage (metastatic) HER2-positive breast cancer from 20.3 to 25.1 months.[16] In early-stage HER2-positive breast cancer, it reduces the risk of cancer returning after surgery. The absolute reduction in the risk of cancer returning within 3 years was 9.5%, and the absolute reduction in the risk of death within 3 years was reduced by 3%. However, it increases serious heart problems by an absolute risk of 2.1%, though the problems may resolve if treatment is stopped.[17]
Trastuzumab has had a "major impact in the treatment of HER2-positive metastatic breast cancer."[18] The combination of trastuzumab with chemotherapy has been shown to increase both survival and response rate, in comparison to trastuzumab alone.[19]
It is possible to determine the "erbB2 status" of a tumor, which can be used to predict efficacy of treatment with trastuzumab. If it is determined that a tumor is overexpressing the erbB2 oncogene and the patient has no significant pre-existing heart disease, then a patient is eligible for treatment with trastuzumab.[20] It is surprising that although trastuzumab has great affinity for HER2 and high doses can be administered (because of its low toxicity), 70% of HER2+ patients do not respond to treatment. In fact resistance to the treatment develops rapidly, in virtually all patients. A mechanism of resistance involves failure to downregulate p27 (Kip1) [21] as well as suppressing p27 translocation to the nucleus in breast cancer, enabling cdk2 to induce cell proliferation.[22]
Duration of treatment
The optimal duration of add-on trastuzumab treatment after surgery for early breast cancer is currently unknown. One year of treatment is generally accepted based on current clinical trial evidence that demonstrated the superiority of one-year treatment over none.[23][24] However, a small Finnish trial also showed similar improvement with nine weeks of treatment over no therapy.[25] Because of the lack of direct head-to-head comparison in clinical trials, it is unknown whether a shorter duration of treatment may be just as effective (with fewer side effects) than the currently accepted practice of treatment for one year. Debate about treatment duration has become a relevant issue for many public health policy makers because administering trastuzumab for a year is very expensive. Consequently, some countries with a taxpayer-funded public health system, such as New Zealand, chose to fund limited adjuvant therapy.[26] However, subsequently New Zealand has revised its policy and now funds trastuzumab treatment for up to 12 months.[27]
Adverse effects
Some of the common side effects of trastuzumab are flu-like symptoms (such as fever, chills and mild pain), nausea and diarrhea.[28]
Cardiac toxicity
One of the more serious complications of trastuzumab is its effect on the heart, although this is rare.[28] In 2-7% of cases,[29] trastuzumab is associated with cardiac dysfunction, which includes congestive heart failure. As a result, regular cardiac screening with either a MUGA scan or echocardiography is commonly undertaken during the trastuzumab treatment period. The decline in ejection fraction appears to be reversible.[30]
Trastuzumab downregulates neuregulin-1 (NRG-1), which is essential for the activation of cell survival pathways in cardiomyocytes and the maintenance of cardiac function. NRG-1 activates the MAPK pathway and the PI3K/AKT pathway as well as focal adhesion kinases (FAK). These are all significant for the function and structure of cardiomyocytes. Trastuzumab can therefore lead to cardiac dysfunction.[31]
Approximately 10% of people are unable to tolerate the drug because of pre-existing heart problems; physicians are balancing the risk of recurrent cancer against the higher risk of death due to cardiac disease in this population. The risk of cardiomyopathy is increased when trastuzumab is combined with anthracycline chemotherapy (which itself is associated with cardiac toxicity).
Mechanism of action
The HER2 gene (also known as HER2/neu and ErbB2 gene) is amplified in 20–30% of early-stage breast cancers.[21] Trastuzumab is a monoclonal antibody targeting HER2, inducing an immune-mediated response that causes internalization and downregulation of HER2. It may also upregulate cell cycle inhibitors such as p21Waf1 and p27Kip1.[33]
The HER2 pathway promotes cell growth and division when it is functioning normally; however, when it is overexpressed, cell growth accelerates beyond its normal limits. In some types of cancer, the pathway is exploited to promote rapid cell growth and proliferation and hence tumor formation.[34] The EGF pathway includes the receptors HER1 (EGFR), HER2, HER3, and HER4; the binding of ligands (e.g. EGF etc.) to HER receptors is required to activate the pathway.[34] The pathway initiates the MAP kinase pathway as well as the PI3 kinase/AKT pathway, which in turn activates the NF-κB pathway.[35] In cancer cells the HER2 protein can be expressed up to 100 times more than in normal cells (2 million versus 20,000 per cell).[36] This overexpression leads to strong and constant proliferative signaling and hence tumor formation. Overexpression of HER2 also causes deactivation of checkpoints, allowing for even greater increases in proliferation.
The HER receptors are proteins that are embedded in the cell membrane and communicate molecular signals from outside the cell (molecules called EGFs) to inside the cell, and turn genes on and off. The HER (human epidermal growth factor receptor) protein, binds to human epidermal growth factor, and stimulates cell proliferation. In some cancers, notably certain types of breast cancer, HER2 is over-expressed and causes cancer cells to reproduce uncontrollably.[16]
HER2 extends across the cell membrane, and carries signals from outside the cell to the inside. Signaling compounds called mitogens (specifically EGF in this case) arrive at the cell membrane, and bind to the extracellular domain of the HER family of receptors. Those bound proteins then link (dimerize), activating the receptor. HER2 sends a signal from its intracellular domain, activating several different biochemical pathways. These include the PI3K/Akt pathway and the MAPK pathway. Signals on these pathways promote cell proliferation and the growth of blood vessels to nourish the tumor (angiogenesis).[37]
Normal cell division—mitosis—has checkpoints that keep cell division under control. Some of the proteins that control this cycle are called cdk2 (CDKs). Overexpression of HER2 sidesteps these checkpoints, causing cells to proliferate in an uncontrolled fashion.[22] This is caused by phosphorylation by Akt.
Trastuzumab binds to domain IV of the[38] extracellular segment of the HER2/neu receptor. Monoclonal antibodies that bind to this region have been shown to reverse the phenotype of HER2/neu expressing tumor cells.[39] Cells treated with trastuzumab undergo arrest during the G1 phase of the cell cycle so there is reduced proliferation. It has been suggested that trastuzumab does not alter HER-2 expression, but downregulates activation of AKT.[22] In addition, trastuzumab suppresses angiogenesis both by induction of antiangiogenic factors and repression of proangiogenic factors. It is thought that a contribution to the unregulated growth observed in cancer could be due to proteolytic cleavage of HER2/neu that results in the release of the extracellular domain. One of the most relevant proteins that trastuzumab activates is the tumor suppressor p27 (kip1), also known as CDKN1B.[21] Trastuzumab has been shown to inhibit HER2/neu ectodomain cleavage in breast cancer cells.[40]
Experiments in laboratory animals indicate that antibodies, including trastuzumab, when bound to a cell, induce immune cells to kill that cell, and that such antibody-dependent cell-mediated cytotoxicity is another important mechanism of action.[41]
There may be other undiscovered mechanisms by which trastuzumab induces regression in cancer.
Predicting response
Trastuzumab inhibits the effects of overexpression of HER2. If the breast cancer does not overexpress HER2, trastuzumab will have no beneficial effect (and may cause harm). Doctors use laboratory tests to discover whether HER2 is overexpressed. In the routine clinical laboratory, the most commonly employed methods for this are immunohistochemistry (IHC) and either silver, chromogenic or fluorescent in situ hybridisation (SISH/CISH/FISH). HER2 amplification can be detected by virtual karyotyping of formalin-fixed paraffin embedded tumor. Virtual karyotyping has the added advantage of assessing copy number changes throughout the genome, in addition to detecting HER-2 amplification (but not overexpression). Numerous PCR-based methodologies have also been described in the literature.[42] It is also possible to estimate HER2 copy number from microarray data.[43]
There are two FDA-approved commercial kits available for HER2 IHC; Dako HercepTest[44] and Ventana Pathway.[45] These are highly standardised, semi-quantitative assays which stratify expression levels into; 0 (<20,000 receptors per cell, no visible expression), 1+ (~100,000 receptors per cell, partial membrane staining, < 10% of cells overexpressing HER-2), 2+ (~500,000 receptors per cell, light to moderate complete membrane staining, > 10% of cells overexpressing HER-2), and 3+ (~2,000,000 receptors per cell, strong complete membrane staining, > 10% of cells overexpressing HER-2). The presence of cytoplasmic expression is disregarded. Treatment with trastuzumab is indicated in cases where HER2 expression has a score of 3+. However, IHC has been shown to have numerous limitations, both technical and interpretative, which have been found to impact on the reproducibility and accuracy of results, especially when compared with ISH methodologies. It is also true, however, that some reports have stated that IHC provides excellent correlation between gene copy number and protein expression.
Fluorescent in situ hybridization (FISH) is viewed as being the "gold standard" technique in identifying patients who would benefit from trastuzumab, but it is expensive and requires fluorescence microscopy and an image capture system. The main expense involved with CISH is in the purchase of FDA-approved kits, and as it is not a fluorescent technique it does not require specialist microscopy and slides may be kept permanently. Comparative studies of CISH and FISH have shown that these two techniques show excellent correlation. The lack of a separate chromosome 17 probe on the same section is an issue with regards to acceptance of CISH. As of June 2011 Roche has obtained FDA approval for the INFORM HER2 Dual ISH DNA Probe cocktail [46] developed by Ventana Medical Systems.[45] The DDISH (Dual-chromagen/Dual-hapten In-situ hybridization) cocktail uses both HER2 and Chromosome 17 hybridization probes for chromagenic visualization on the same tissue section. The detection can be achieved by using a combination of ultraView SISH(silver in-situ hybridization) and ultraView Red ISH for deposition of distinct chromgenic precipitates at the site of DNP or DIG labeled probes.[47]
Currently the recommended assays are a combination of IHC and FISH, whereby IHC scores of 0 and 1+ are negative (no trastuzumab treatment), scores of 3+ are positive (trastuzumab treatment), and score of 2+ (equivocal case) is referred to FISH for a definitive treatment decision. Industry best practices indicate the use of FDA-cleared Automated Tissue Image Systems by laboratories for automated processing of specimens, thereby reducing process variability, avoiding equivocal cases, and ensuring maximum efficacy of trastuzumab therapy.
Resistance
One of the challenges in the treatment of breast cancer patients by herceptin is our understanding towards herceptin resistance. In the last decade, several assays have been performed to understand the mechanism of Herceptin resistance with/without supplementary drugs. Recently, all this information has been collected and compiled in form of a database HerceptinR.[48] This database HerceptinR is a collection of assays performed to test sensitivity or resistance of Herceptin Antibodies towards breast cancer cell lines. This database provides comprehensive information about experimental data perform to understanding factors behind herceptin resistance as well as assays performed for improving Herceptin sensitivity with the help of supplementary drugs. This is the first database developed to understand herceptin resistance that can be used for designing herceptin sensitive biomarkers.
History
The drug was first discovered by scientists including Dr. Axel Ullrich and Dr. H. Michael Shepard at Genentech, Inc. in South San Francisco, CA.[49] Earlier discovery about the neu oncogene by Robert Weinberg's lab [50] and the monoclonal antibody recognizing the oncogenic receptor by Mark Greene's lab [51] also contributed to the establishment of HER2 targeted therapies. Dr. Dennis Slamon subsequently worked on trastuzumab's development. A book about Dr. Slamon's work was made into a television film called Living Proof, that premiered in 2008. Genentech developed trastuzumab jointly with UCLA, beginning the first clinical trial with 15 women in 1992.[52] By 1996, clinical trials had expanded to over 900 women, but due to pressure from advocates based on early success, Genentech worked with the FDA to begin a lottery system allowing 100 women each quarter access to the medication outside the trials.[53] Herceptin was Fast-tracked by the FDA and gained approval in September 1998.
Biocon Ltd and its partner Mylan obtained regulatory approval to sell a biosimilar in 2014, but Roche contested the legality of the approval; that litigation ended in 2016, and Biocon and Mylan each introduced their own branded biosimilars.[54]
Society and culture
Costs
Trastuzumab costs about US$70,000 for a full course of treatment,[55] Trastuzumab brought in $327 million in revenue for Genentech in the fourth quarter of 2007.
Australia has negotiated a lower price of A$50,000 per course of treatment.[56]
Since October 2006, trastuzumab has been made available for Australian women and men with early-stage breast cancer via the Pharmaceutical Benefits Scheme. This is estimated to cost the country over A$470 million for 4–5 years supply of the drug.[57]
Roche has agreed with Emcure in India to make an affordable version of this cancer drug available to the Indian market.[58]
Roche has changed the trade name of the drug and has re-introduced an affordable version of the same in the Indian market. The new drug named Herclon would cost approximately RS75,000 INR (US$1,200) in the Indian market.
On September 16, 2014, Genentech notified hospitals in the United States that, as of October, trastuzumab could only be purchased through their selected specialty drugs distributors not through the usual general line wholesalers. By being forced to purchase through specialty pharmacies, hospitals lost rebates from the big wholesalers and the ability to negotiate cost-minus discounts with their wholesalers.[59]
Biosimilars
By 2014, around 20 companies, particularly from emerging markets, were developing biosimilar versions of trastuzumab after Roche/Genentech's patents expired in 2014 in Europe, and in 2019 in the United States.[60] In 2013, Roche/Genentech relinquished its patent right for the drug in India because of the difficult IP environment there.
In January 2015, BIOCAD announced the first trastuzumab biosimilar approved by the Ministry of Health of the Russian Federation. Iran also approved its own version of the monoclonal antibody in January 2016, as AryoTrust, and announced its readiness to export the drug to other countries in the Middle-East and Central Asia when trade sanctions were lifted.[1][61]
In 2016, the investigational biosimilar MYL-1401O has shown comparable efficacy and safety to the Herceptin branded trastuzumab.[62]
Trastuzumab-dkst (Ogivri, Mylan GmbH) was approved in the United States in December 2017, to "treat patients with breast cancer or gastric or gastroesophageal junction adenocarcinoma whose tumors overexpress the HER-2 gene."[63][64] Ogivri was approved for medical use in the European Union in December 2018.[65]
In November 2017, the European Commission approved Ontruzant, a biosimilar-trastuzumab from Samsung Bioepis Co., Ltd, for the treatment of early breast cancer, metastatic breast cancer and metastatic gastric cancer.[10] Ontruzant is the first trastuzumab biosimilar to receive regulatory approval in Europe.[66]
Herzuma was approved for medical use in the European Union in February 2018.[67] Herzuma, a trastuzumab biosimilar, was approved in the United States in December 2018.[12][68][11] The approval was based on comparisons of extensive structural and functional product characterization, animal data, human pharmacokinetic, clinical immunogenicity, and other clinical data demonstrating that Herzuma is biosimilar to US Herceptin.[11] Herzuma has been approved as a biosimilar, not as an interchangeable product.[11]
Kanjinti was approved for medical use in the European Union in May 2018.[69]
Trazimera was approved for medical use in the European Union in July 2018.[70]
Zercepac was approved for medical use in the European Union in July 2020.[71]
Related conjugates
Apart from the biosimilars noted above, trastuzumab is also a component of some antibody-drug conjugates, such as trastuzumab emtansine. Another ADC, trastuzumab deruxtecan was approved for use in the United States in December 2019.[72]
References
- "Trastuzumab - Drugs.com". www.drugs.com. Archived from the original on 7 April 2017. Retrieved 21 December 2016.
- "Trastuzumab Pregnancy and Breastfeeding Warnings". Drugs.com. Archived from the original on 3 December 2019. Retrieved 3 December 2019.
- "Trastuzumab". The American Society of Health-System Pharmacists. Archived from the original on 21 December 2016. Retrieved 8 December 2016.
- "Herceptin- trastuzumab kit Herceptin- trastuzumab injection, powder, lyophilized, for solution". DailyMed. 30 September 2019. Retrieved 28 July 2020.
- "FDA approves first biosimilar for the treatment of certain breast and stomach cancers". U.S. Food and Drug Administration (FDA) (Press release). 10 September 2019. Retrieved 18 February 2020.
- "Herceptin EPAR". European Medicines Agency (EMA). Retrieved 28 July 2020.
- British national formulary : BNF 69 (69 ed.). British Medical Association. 2015. p. 626. ISBN 9780857111562.
- "Trastuzumab Product Approval Information - Licensing Action 9/25/98". U.S. Food and Drug Administration (FDA). 18 December 2015. Archived from the original on 28 January 2017. Retrieved 3 December 2019.
 This article incorporates text from this source, which is in the public domain.
This article incorporates text from this source, which is in the public domain. - World Health Organization (2019). World Health Organization model list of essential medicines: 21st list 2019. Geneva: World Health Organization. hdl:10665/325771. WHO/MVP/EMP/IAU/2019.06. License: CC BY-NC-SA 3.0 IGO.
- "Ontruzant EPAR". European Medicines Agency (EMA). Retrieved 28 July 2020.
- "FDA approves Herzuma as a biosimilar to Herceptin". U.S. Food and Drug Administration (FDA) (Press release). 18 December 2018. Archived from the original on 13 December 2019. Retrieved 12 December 2019. This article incorporates text from this source, which is in the public domain.
- "Drug Approval Package: Herzuma". U.S. Food and Drug Administration (FDA). 7 February 2019. Retrieved 28 July 2020.
- Balduzzi S, Mantarro S, Guarneri V, Tagliabue L, Pistotti V, Moja L, D'Amico R (2014). "Trastuzumab-containing regimens for metastatic breast cancer" (PDF). Cochrane Database Syst Rev. 6 (6): CD006242. doi:10.1002/14651858.CD006242.pub2. PMC 6464904. PMID 24919460.
- Wilcken, Nicholas (2014). Tovey, David (ed.). "Treating metastatic breast cancer: The evidence for targeted therapy". The Cochrane Database of Systematic Reviews (6): ED000083. doi:10.1002/14651858.ED000083. PMID 25032250.
- Moja L, Tagliabue L, Balduzzi S, Parmelli E, Pistotti V, Guarneri V, D'Amico R (2012). "Trastuzumab containing regimens for early breast cancer". Cochrane Database Syst Rev. 4 (4): CD006243. doi:10.1002/14651858.CD006243.pub2. PMC 6718210. PMID 22513938.
- Hudis, CA (2007). "Trastuzumab--mechanism of action and use in clinical practice". N Engl J Med. 357 (1): 39–51. doi:10.1056/NEJMra043186. PMID 17611206.
- Moja L, Tagliabue L, Balduzzi S, et al. (2012). "Trastuzumab containing regimens for early breast cancer". Cochrane Database Syst Rev. 4: CD006243. doi:10.1002/14651858.CD006243.pub2. PMC 6718210. PMID 22513938.
- Tan, AR; Swain SM (2002). "Ongoing adjuvant trials with trastuzumab in breast cancer". Seminars in Oncology. 30 (5 Suppl 16): 54–64. doi:10.1053/j.seminoncol.2003.08.008. PMID 14613027.
- Nahta, R; Esteva1 FJ (2003). "HER-2-Targeted Therapy –Lessons Learned and Future Directions". Clinical Cancer Research. 9 (14): 5078–84. PMID 14613984.
- Yu, D; Hung M (2000). "Overexpression of ErbB2 in cancer and ErbB2-targeting strategies". Oncogene. 19 (53): 6115–6121. doi:10.1038/sj.onc.1203972. PMID 11156524.
- XF Le; Franz Pruefer; Robert Bast. (2005). "HER2-targeting antibodies modulate the cyclin-dependent kinase inhibitor p27Kip1 via multiple signaling pathways". Cell Cycle. 4 (1): 87–95. doi:10.4161/cc.4.1.1360. PMID 15611642.
- Kute, T; Lack CM; Willingham M; Bishwokama B; Williams H; Barrett K; Mitchell T; Vaughn JP (2004). "Development of Herceptin resistance in breast cancer cells". Cytometry. 57A (2): 86–93. doi:10.1002/cyto.a.10095. PMID 14750129. S2CID 40236173.
- Romond, EH; Perez EA; Bryant J; et al. (2005). "Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer". New England Journal of Medicine. 353 (16): 1673–1684. doi:10.1056/NEJMoa052122. PMID 16236738.
- Piccart-Gebhart MJ, MJ; Procter M; Leyland-Jones B; et al. (2005). "Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer". New England Journal of Medicine. 353 (16): 1659–1672. doi:10.1056/NEJMoa052306. hdl:10722/251817. PMID 16236737.
- Joensuu H, Kellokumpu-Lehtinen PL, Bono P, et al. (2006). "Adjuvant docetaxel or vinorelbine with or without trastuzumab for breast cancer". N Engl J Med. 354 (8): 809–20. doi:10.1056/NEJMoa053028. PMID 16495393. S2CID 25832514.
- Metcalfe, S; Evans J; Priest G. (2007). "PHARMAC funding of 9-week concurrent trastuzumab (Herceptin) for HER2-positive early breast cancer". N Z Med J. 120 (1256): 1U2593. PMID 17589560.
- "12-month Herceptin treatment now available". New Zealand Government. Archived from the original on 20 January 2017. Retrieved 2 May 2017.
- "Breast Cancer Care Trastuzumab factsheet" (PDF). Breast Cancer Care. Archived (PDF) from the original on 23 October 2013. Retrieved 22 October 2013.
- Seidman, A; et al. (2002). "Cardiac Dysfunction in the Trastuzumab Clinical Trials Experience". Journal of Clinical Oncology. 20 (5): 1215–1221. doi:10.1200/JCO.20.5.1215. PMID 11870163.
- van Hasselt; et al. (2011). "Population pharmacokinetic-pharmacodynamic analysis of trastuzumab-associated cardiotoxicity". Clin Pharmacol Ther. 90 (1): 126–32. doi:10.1038/clpt.2011.74. PMID 21633346. S2CID 27190873.
- Zeglinski, M., Ludke, A., Jassal, D. S. & Singal, P. K. Trastuzumab-induced cardiac dysfunction: A 'dual-hit'. Exp. Clin. Cardiol. 16, 70-74 (2011)
- "Breast Cancer Care Trastuzumab factsheet" (PDF). Archived (PDF) from the original on 23 October 2013. Retrieved 22 October 2013.
- Bange, J; Zwick E; Ullrich A. (2001). "Molecular targets for breast cancer therapy and prevention". Nature Medicine. 7 (5): 548–552. doi:10.1038/87872. PMID 11329054. S2CID 6010551.
- "Targeted Therapies for Breast Cancer Tutorial". National Cancer Institute. Archived from the original on 29 March 2011. Retrieved 19 April 2011.
- Feldman, A M; Koch, W J; Force, T L (28 March 2007). "Developing Strategies to Link Basic Cardiovascular Sciences with Clinical Drug Development: Another Opportunity for Translational Sciences". Clinical Pharmacology & Therapeutics. 81 (6): 887–892. doi:10.1038/sj.clpt.6100160. PMID 17392727. S2CID 34778864.
- Winer, Eric. "HER2 Disease in the Metastatic and Adjuvant Settings". Medscape Education. Archived from the original on 10 April 2011. Retrieved 20 April 2011.
- Ménard, S; Pupa SM; Campiglio M; Tagliabue E (2003). "Biologic and therapeutic role of HER2 in cancer". Oncogene. 22 (42): 6570–6578. doi:10.1038/sj.onc.1206779. PMID 14528282.
- Cho, Hyun-Soo; Mason, Karen; Ramyar, Kasra X.; Stanley, Ann Marie; Gabelli, Sandra B.; Denney, Dan W.; Leahy, Daniel J. (2003). "Structure of the extracellular region of HER2 alone and in complex with the Herceptin Fab". Nature. 421 (6924): 756–760. Bibcode:2003Natur.421..756C. doi:10.1038/nature01392. PMID 12610629. S2CID 2311471.
- Drebin, J. A.; Stern, D. F.; Link, V. C.; Weinberg, R. A.; Greene, M. I. (6–12 December 1984). "Monoclonal antibodies identify a cell-surface antigen associated with an activated cellular oncogene". Nature. 312 (5994): 545–548. Bibcode:1984Natur.312..545D. doi:10.1038/312545a0. ISSN 0028-0836. PMID 6504162. S2CID 4357211.
- Albanell, J; Codony J; Rovira A; Mellado B; Gascon P. (2003). Mechanism of action of anti-HER2 monoclonal antibodies: scientific update on trastuzumab and 2C4. Advances in Experimental Medicine and Biology. 532. pp. 253–268. doi:10.1007/978-1-4615-0081-0_21. ISBN 978-0-306-47762-1. PMID 12908564.
- Clynes, RA; Towers, TL; Presta, LG; Ravetch, JV (2000). "Inhibitory Fc receptors modulate in vivo cytoxicity against tumor targets". Nat Med. 6 (4): 443–6. doi:10.1038/74704. PMID 10742152. S2CID 20629632.
- Jennings, B; Hadfield JE; Worsley SD; Girling A; Willis G. (1997). "A differential PCR assay for the detection of c-erbB 2 amplification used in a prospective study of breast cancer". Molecular Pathology. 50 (5): 254–256. doi:10.1136/mp.50.5.254. PMC 379641. PMID 9497915.
- Curtis, C; Shah, SP; Chin, SF; Turashvili, G; Rueda, OM; Dunning, MJ; Speed, D; Lynch, AG; Samarajiwa, S; Yuan, Y; Gräf, S; Ha, G; Haffari, G; Bashashati, A; Russell, R; McKinney, S; METABRIC, Group; Langerød, A; Green, A; Provenzano, E; Wishart, G; Pinder, S; Watson, P; Markowetz, F; Murphy, L; Ellis, I; Purushotham, A; Børresen-Dale, AL; Brenton, JD; Tavaré, S; Caldas, C; Aparicio, S (18 April 2012). "The genomic and transcriptomic architecture of 2,000 breast tumours reveals novel subgroups". Nature. 486 (7403): 346–52. Bibcode:2012Natur.486..346.. doi:10.1038/nature10983. PMC 3440846. PMID 22522925.
- "Archived copy". Archived from the original on 23 May 2009. Retrieved 24 June 2008.CS1 maint: archived copy as title (link)
- "ventanamed.com". ventanamed.com. 25 May 2012. Archived from the original on 27 November 2011. Retrieved 16 June 2013.
- "Ventana Medical Systems, Inc. Receives FDA Approval for the First Fully Automated Diagnostic Assay for HER2 Gene Status Determination in Breast Cancer Patients". BioPortfolio.com. 14 June 2011. Archived from the original on 25 March 2012. Retrieved 6 January 2013.
- "Dual color dual hapten HER2 genotyping for breast biopsy specimens (DDISH): Concordance with fluorescence in situ hybridization (FISH)". ASCO. 6 October 2009. Archived from the original on 23 March 2012. Retrieved 6 January 2013.
- Ahmad S (2014). "Herceptin Resistance Database for Understanding Mechanism of Resistance in Breast Cancer Patients". Nature. 4: 4483. Bibcode:2014NatSR...4E4483A. doi:10.1038/srep04483. PMC 3967150. PMID 24670875.
- "cancer.ucla.edu". cancer.ucla.edu. Archived from the original on 11 June 2013. Retrieved 16 June 2013.
- Schechter, A. L.; Stern, D. F.; Vaidyanathan, L.; Decker, S. J.; Drebin, J. A.; Greene, M. I.; Weinberg, R. A. (6–12 December 1984). "The neu oncogene: an erb-B-related gene encoding a 185,000-Mr tumour antigen". Nature. 312 (5994): 513–516. Bibcode:1984Natur.312..513S. doi:10.1038/312513a0. ISSN 0028-0836. PMID 6095109. S2CID 4357655.
- Drebin, J. A.; Link, V. C.; Weinberg, R. A.; Greene, M. I. (December 1986). "Inhibition of tumor growth by a monoclonal antibody reactive with an oncogene-encoded tumor antigen". Proceedings of the National Academy of Sciences of the United States of America. 83 (23): 9129–9133. Bibcode:1986PNAS...83.9129D. doi:10.1073/pnas.83.23.9129. ISSN 0027-8424. PMC 387088. PMID 3466178.
- "Biotechnology Breakthrough In Breast Cancer Wins FDA Approval". Genentech. 25 September 1998. Archived from the original on 1 July 2016. Retrieved 30 May 2016.
- Altman, Lawrence (18 May 1998). "Drug Is Shown to Shrink Tumors in Breast Cancer Characterized by Gene Defect". New York Times. Archived from the original on 30 June 2016. Retrieved 30 May 2016.
- Palmer, Eric (3 March 2017). "Mylan and Biocon finally win right to sell Herceptin biosim in India even as they have taken it to U.S. and EU". FiercePharma. Archived from the original on 8 September 2017.
- Fleck L (2006). "The costs of caring: Who pays? Who profits? Who panders?". Hastings Cent Rep. 36 (3): 13–7. doi:10.1353/hcr.2006.0040. PMID 16776017. S2CID 7873442.
- "Listing of Herceptin on PBS". Australian Government, Dept of Health and Ageing. 1 October 2006. Archived from the original on 12 September 2009. Retrieved 6 August 2009.
- Australian Government, Dept of Health and Ageing "Listing of Herceptin on PBS", 2006-10-1. "Pharmaceutical Benefits Scheme (PBS) | Listing of Herceptin on the PBS". Archived from the original on 23 October 2013. Retrieved 20 October 2013.
- "Emcure signs deal to manufacture Roche's anti-cancer drugs". The Times Of India. 2 March 2012.
- Saporito, Bill (27 October 2014). "Hospitals Furious at Cancer-Drug Price Hikes". Time. Archived from the original on 20 October 2015. Retrieved 26 October 2015.
- Cynthia A. Challener (1 April 2014). Monoclonal Antibodies Key to Unlocking the Biosimilars Market Archived 2016-03-01 at the Wayback Machine. BioPharm international.com 27 (4).
- Dominik Feldges (February 2016). Brustkrebspräparat Herceptin im Fokus Archived 2016-03-02 at the Wayback Machine (in German). Neue Zürcher Zeitung (Wirtschaft). Retrieved 19 February 2016.
- Biosimilar Matches Trastuzumab in Metastatic HER2-Positive Breast Cancer. June 2016 Archived 2016-06-11 at the Wayback Machine
- "FDA approves Ogivri as a biosimilar to Herceptin". U.S. Food and Drug Administration (FDA). 1 December 2017. Archived from the original on 3 December 2019. Retrieved 2 December 2019. This article incorporates text from this source, which is in the public domain.
- FDA approves Ogivri, first biosimilar for certain breast, stomach cancers. December 2017
- "Ogivri EPAR". European Medicines Agency (EMA). Retrieved 28 July 2020.
- Samsung Bioepis Receives Regulatory Approval for Europe's First Trastuzumab Biosimilar. Nov 2017
- "Herzuma EPAR". European Medicines Agency (EMA). Retrieved 28 July 2020.
- "Herzuma" (PDF). U.S. Food and Drug Administration (FDA). Retrieved 21 December 2018.
- "Kanjinti EPAR". European Medicines Agency (EMA). Retrieved 28 July 2020.
- "Trazimera EPAR". European Medicines Agency (EMA). Retrieved 28 July 2020.
- "Zercepac EPAR". European Medicines Agency (EMA). Retrieved 28 July 2020.
- "FDA approves new treatment option for patients with HER2-positive breast cancer who have progressed on available therapies". U.S.Food and Drug Administration (FDA) (Press release). 20 December 2019. Archived from the original on 20 December 2019. Retrieved 20 December 2019.
Further reading
- Bazell, Robert. Her-2: the making of Herceptin, a revolutionary treatment for breast cancer. Random House, 1998. 214 pages. ISBN 0-679-45702-X.
- Boseley, Sarah (29 March 2006). "The selling of a wonder drug". The Guardian.
- Dent S, Verma S, Latreille J, Rayson D, Clemons M, Mackey J, Verma S, Lemieux J, Provencher L, Chia S, Wang B, Pritchard K (2009). "The role of her2-targeted therapies in women with her2-overexpressing metastatic breast cancer". Curr Oncol. 16 (4): 25–35. doi:10.3747/co.v16i4.469. PMC 2722050. PMID 19672422.
- Dean L (2015). "Trastuzumab (Herceptin) Therapy and ERBB2 (HER2) Genotype". In Pratt VM, McLeod HL, Rubinstein WS, et al. (eds.). Medical Genetics Summaries. National Center for Biotechnology Information (NCBI). PMID 28520362. Bookshelf ID: NBK310376.
External links
| Look up trastuzumab in Wiktionary, the free dictionary. |
- "Trastuzumab". Drug Information Portal. U.S. National Library of Medicine.
- "Trastuzumab". National Cancer Institute.
