Axonotmesis
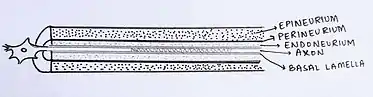
Axonotmesis is an injury to the peripheral nerve of one of the extremities of the body. The axons and their myelin sheath are damaged in this kind of injury, but the endoneurium, perineurium and epineurium remain intact. Motor and sensory functions distal to the point of injury are completely lost over time leading to Wallerian degeneration due to ischemia, or loss of blood supply. Axonotmesis is usually the result of a more severe crush or contusion than neurapraxia.[1]
Axonotmesis mainly follows a stretch injury. These stretch injuries can either dislocate joints or fracture a limb, due to which peripheral nerves are severed. If the sharp pain from the exposed axon of the nerve is not observed, one can identify a nerve injury from abnormal sensations in their limb. A doctor may ask for a nerve conduction velocity (NCV) test to completely diagnose the issue. If diagnosed as nerve injury, electromyography performed after 3 to 4 weeks shows signs of denervations and fibrillations, or irregular connections and contractions of muscles.[2]
Injury classification
There are two kinds of nerve injury classifications:[3]
| Seddon | Sunderland |
|---|---|
| Neurapraxia | Grade I |
| Axonotmesis | Grade II |
| Axonotmesis | Grade III |
| Axonotmesis | Grade IV |
| Neurotmesis | Grade V |
Sunderland's Stage II Classification
- Endoneurial tube remains intact
- Emergence of Wallerian degeneration
- Can be detected with Tinel's sign
Sunderland's Stage III Classification
- Endoneurial tube is damaged
- Perineurium remains intact
- Scarring occurs
- Intrafascicular fibrosis occurs due to edema
Sunderland's Stage IV Classification
- Perineurium is damaged
- Epineurium remains intact
- Neuroma could occur
- Surgery is required for treatment
Assessment
A nerve contains sensory fibers, motor fibers, or both. Sensory fibers lesions cause the sensory problems below to the site of injury. Motor fibers injuries may involve lower motor neurons, sympathetic fibers, and or both.
Assessment items include:
- Sensory fibers that send sensory information to the central nervous system.
- Motor fibers that allow movement of skeletal muscle.
- Sympathetic fibers that innervate the skin and blood vessels of the four extremities.
In assessment, sensory-motor defects may be mild, moderate, or severe. Damage to motor fibers results in paralysis of the muscles. Nervous plexus injuries create more signs and symptoms from sensory-motor problems (such as brachial plexus injuries). In these cases, the prognosis depends on the amount of damage and the degree of functional impairment.
EMG and NCV findings
Changes in EMG
Electromyography (EMG) is a medical test performed to evaluate and record the electrical activity (electromyogram) produced by skeletal muscles using an instrument called electromyograph. In axonotmesis, EMG changes (2 to 3 weeks after injury) in the denervated muscles include:
- Fibrillation potentials (FP)
- Positive sharp waves
Changes in NCV (nerve conduction velocity)
EMG test is often performed together with another test called nerve conduction study, which measures the conducting function of nerves. NCV study shows loss of nerve conduction in the distal segment (3 to 4 days after injury). According to NCV study, in axonotmesis there is an absence of distal sensory-motor responses.
Treatment
Schwann cells provide the nerve with protection through the production of Nerve Growth Factors, and because these cells are intact this kind of nerve injury can be cured and normal feeling and sensations can be restored. Surgery can be done in order to help the nerve heal. The surgery will help with nerve regeneration, providing guidance to the nerve sprouts on where to attach on the proximal side of the injury. Damaged nerve axons can reattach themselves after surgery.[3] Treatment of axonotmesis also consists of:
- Physical therapy or Occupational Therapy. Physical or Occupational therapy aims include:
- Pain relief
- Maintain range of motion
- Reducing muscular atrophy
- Patient education
- Use of assistive devices (Orthotic needs)
Prognosis
The prognosis is usually good in terms of recovery. Rate of recovery depends on the distance from the site of injury, and axonal regeneration can go up to 1 inch per month. Complete recovery can take anywhere from 6 months to a year[6]
See also
References
- Saidoff, David C.; McDonough, Andrew (2002). Critical Pathways in Therapeutic Intervention. Missouri: Mosby Inc. p. 262. ISBN 0-323-00105-X.
- "Nerve Injury (Neuropraxia, Axonotmesis, Neurotmesis) and Healing | Healthhype.com". www.healthhype.com. Retrieved 2017-05-03.
- Menorca, Ron M. G.; Fussell, Theron S.; Elfar, John C. (2017-05-05). "Peripheral Nerve Trauma: Mechanisms of Injury and Recovery". Hand clinics. 29 (3): 317–330. doi:10.1016/j.hcl.2013.04.002. ISSN 0749-0712. PMC 4408553. PMID 23895713.
- Prince, Jim McMorran, Damian Crowther, Stew McMorran, Steve Youngmin, Ian Wacogne, Jon Pleat, Clive. "Sunderland classification of nerve injuries - General Practice Notebook". www.gpnotebook.co.uk. Retrieved 2017-05-05.
- Goubier, Jean-Noel (2015). Nerve and Nerve Injuries, 1st Edition. Vol 2: Pain, Treatment, Injury, Disease and Future Directions. London: Academic Press. p. 604. ISBN 9780128026533.
- Otto D. Payton & Richard P. Di Fabio et al. Manual of physical therapy. Churchill Livingstone Inc. Page 24. ISBN 0-443-08499-8
