Food desert
A food desert is an area that has limited access to affordable and nutritious food,[1][2][3] in contrast with an area with higher access to supermarkets or vegetable shops with fresh foods, which is called a food oasis.[4] The designation considers the type and quality of food available to the population, in addition to the accessibility of the food through the size and proximity of the food stores.[5]


In 2010, the United States Department of Agriculture reported that 23.5 million people in the U.S. live in "food deserts", meaning that they live more than one mile from a supermarket in urban or suburban areas and more than 10 miles from a supermarket in rural areas.[6]
Food deserts tend to be inhabited by low-income residents with reduced mobility; this makes them a less attractive market for large supermarket chains.[7] Food deserts lack suppliers of fresh foods, such as meats, fruits, and vegetables. Instead, the available foods are often processed and high in sugar and fats, which are known contributors to the proliferation of obesity in the U.S.[8]
History
By 1973, the term "desert" was ascribed to suburban areas lacking amenities important for community development.[9] A report by Cummins and Macintyre states that a resident of public housing in western Scotland supposedly coined the more specific phrase "food desert" in the early 1990s.[10] The phrase was first officially used in a 1995 document from a policy working group on the Low Income Project Team of the UK's Nutrition Task Force.[10]
Initial research was narrowed to the impact of retail migration from the urban center.[11] More recent studies explored the impact of food deserts in other geographic areas (e.g., rural and frontier) and among specific populations, such as minorities and the elderly. These studies address the relationships between the quality (access and availability) of retail food environments, the price of food, and obesity. Environmental factors can also contribute to people's eating behaviors. Research conducted with variations in methods draws a more complete perspective of "multilevel influences of the retail food environment on eating behaviors (and risk of obesity)."[11]
Definitions
Researchers employ a variety of methods to assess food deserts including directories and census data, focus groups, food store assessments, food use inventories, geographic information system (GIS), interviews, questionnaires and surveys measuring consumers' food access perceptions.[12] Differences in the definition of a food desert vary according to the:
- type of area, urban or rural[13]
- economic barriers and affordability of accessing nutritious foods, including the cost of transportation, price of foods, and incomes of those in the area[10][12][14]
- distance to the nearest supermarket or grocery store[15]
- number of supermarkets in the given area[15]
- type of foods offered, whether it be fresh or prepared[10][12]
- nutritional values of the foods offered[16]
The multitude of definitions that vary by country has fueled controversy over the existence of food deserts.[12]
It should also be noted that because it is too costly to survey the types of foods and prices offered in every store, researchers use the availability of supermarkets and large grocery stores (including discount and super-center stores) as a proxy for the availability of affordable, nutritious food.[17]

Distance
Distance-based measurements are used to measure food accessibility in order to identify food deserts.
The United States Department of Agriculture (USDA) Economic Research Service measures distance by dividing the country into multiple 0.5 km square grids. The distance from the geographic center of each grid to the nearest grocery store gauges food accessibility for the people living in that grid.[18][19] Health Canada divides areas into buffer zones with people's homes, schools or workplaces as the center. The Euclidean distance, another method to measure distance, is the shortest distance between the two points of interest, which is measured for gaining food access data.[20]
Different factors are excluded or included that affect the scale of distance. The USDA maintains an online interactive mapping tool for the United States, the "Food Access Research Atlas," which applies four different measurement standards to identify areas of low food access based on distance from the nearest supermarket.[21]
The first standard uses the original USDA food desert mapping tool "Food Desert Locator" and defines food deserts as having at least 33% or 500 people of a census tract's population in an urban area living 1 mile (10 miles for rural area) from a large grocery store or supermarket.[18][22]
The second and third standards adjust the scale of distance and factor income to define a food desert. In the U.S., a food desert consists of a low-income census tract residing at least 0.5 miles (0.80 km) in urban areas (10 miles (16 km) in rural areas) or 1 mile (1.6 km) away in urban areas (20 miles in rural areas) from a large grocery store.[21] The availability of other fresh food sources like community gardens and food banks are not included in mapping and can change the number of communities that should be classified as food deserts.[23] A 2014 geographical survey found that the average distance from a grocery store was 1.76 kilometers (1.09 miles) in Edmonton, but only 1.44 kilometers (0.89 miles) when farmers' markets and community gardens were included, making it 0.11 miles under the latter definition for an urban food desert.[24]
The fourth standard takes vehicular mobility into account. In the U.S., a food desert exists if 100 households or more with no vehicle access live at least 0.5 miles (0.80 km) from the nearest large grocery store. For populations with vehicle access, the standard changes to 500 households or more living at least 20 miles (32 km) away.[21][25] Travel duration and mode may be other important factors.[26] As of 2011, public transport is not included in mapping tools.[23]
Fresh food availability
A food retailer is typically considered to be a healthful food provider if it sells a variety of fresh food, including fruits and vegetables. Types of fresh food retailers include:
- supermarkets
- local grocery stores
- warehouse clubs
- community gardens
- farmers' markets
Food retailers like fast-food restaurants and convenience stores are not typically in this category as they usually offer a limited variety of foods that could constitute a healthy diet.[18] Frequently, even if there is produce sold at convenience stores it is of poor quality.[27] A "healthy" bodega, as defined by the New York City Department of Health and Mental Hygiene, stocks seven or more varieties of fresh fruits and vegetables and low-fat milk.[28]
Different countries have different dietary models and views on nutrition. These distinct national nutrition guides add to the controversy surrounding the definition of food deserts. Since a food desert is defined as an area with limited access to nutritious foods, a universal identification of them cannot be created without a global consensus on nutrition.
Income and food prices
Other criteria include affordability and income level. According to the USDA, researchers should "consider ... [the] prices of foods faced by individuals and areas" and how "prices affect the shopping and consumption behaviors of consumers."[29] One study maintains that estimates of how many people live in food deserts must include the cost of food in supermarkets that can be reached in relation to their income.[26]
For instance, in 2013, Whole Foods opened a store in Detroit, where one-third of the population lives below the poverty line. Whole Foods is known for its more expensive healthy and organic foods. In order to attract low income residents, the Detroit store offered lower prices compared to other Whole Foods stores.[30] If Whole Foods had not lowered the prices, residents would not be willing to shop there and that area of Detroit would still be considered a food desert.
Rural food deserts
The difference between a rural and an urban food desert is the population density of residents and their distance from the nearest supermarket. Twenty percent of rural areas in the U.S. are classified as food deserts.[31] There are small areas within each state in the U.S. that are classified as rural food deserts, but they occur most prominently in the Midwest[32] Within these counties, approximately 2.4 million individuals have low access to a large supermarket.[21][33] This difference in distance translates into pronounced economic and transportation differences between the rural and urban areas.[34][35] Rural food deserts are mostly the result of large supermarket stores that move into areas and create competition that is impossible for small businesses to keep up with. The competition causes many small grocers to go out of business. This makes the task of getting nutritious, whole ingredients much more difficult for citizens who live far away from large supermarket stores.[36]
In most cases, people who live in rural food deserts are more likely to lack a high school degree or GED, experience increased poverty rates, and have lower median family income. People who live in rural food deserts also tend to be older. This is due to an exodus of young people (ages 20–29) who were born in these areas and decided to leave once they are able.[32]
Based on the 2013 County Health Ratings data, residents who live in rural U.S. food deserts are more likely to have poorer health than those who live in urban food deserts. People who live in rural communities have significantly lower scores in the areas of health behavior, morbidity factors, clinical care, and the physical environment. Research attributes these discrepancies to a variety of factors including limitations in infrastructure, socioeconomic differences, insurance coverage deficiencies, and a higher rate of traffic fatalities and accidents.[37]
In a 2009 study, it was discovered that of the people polled, 64% did not have access to adequate daily amounts of vegetables, and 44.8% did not have access to adequate daily amounts of fruits. Comparatively, only 29.8% of those polled lacked access to adequate protein. This lack of access to fruits and vegetables often results in vitamin deficiencies. This eventually causes health problems for those who live within these areas.[32] When tasked with finding a solution to this problem, research has shown that it will take individual and community actions, as well as public policy improvements, to maintain and increase the capacity of rural grocery stores to provide nutritious, high quality, affordable foods while being profitable enough to stay in business.[32]
Although personal factors do impact eating behavior for rural people, it is the physical and social environments that place constraints on food access, even in civically engaged communities. Food access may be improved in communities where civic engagement is strong, and where local organizations join in providing solutions to help decrease barriers of food access. Some ways communities can do this is by increasing access to the normal and food safety net systems and by creating informal alternatives. Some informal, communal alternatives could be community food gardens and informal transportation networks. Further, existing federal programs could be boosted through greater volunteer involvement.[36]
A 2009 study of rural food deserts found key differences in overall health, access to food, and the social environment of rural residents compared to urban dwellers.[36] Rural residents report overall poorer health and more physical limitations, with 12% rating their health as fair or poor compared to 9% of urban residents.[36] They believed their current health conditions were shaped by their eating behaviors when the future chronic disease risk was affected by the history of dietary intake.[36] Moreover, the 57 recruited rural residents from Minnesota and Iowa in one study perceived that food quality and variety in their area were poor at times.[36] The researchers reached the conclusion that, for a community of people, while food choice which bound by family and household socioeconomic status remained as a personal challenge, social and physical environments played a significant role in stressing and shaping their dietary behaviors.[36]
Urban food deserts
Food deserts occur in poor urban areas when there is limited or no access to healthful, affordable food options.[38] Low income families are more likely to not have access to transportation so tend to be negatively affected by food deserts.[38] An influx of people moving into these urban areas has magnified the existing problems of food access.[39] While urban areas have been progressing in terms of certain opportunities, the poor continue to struggle.[39] As people move to these urban areas they have been forced to adopt new methods for cooking and acquiring food.[39] Adults in urban areas tend to be obese, but they have malnourished and underweight children.[39] For many people, the reason they cannot get nutritious food is because of a lack of supermarkets or grocery stores[26] When supermarkets are inaccessible it has been shown that vegetable and fruit consumption is lower.[38] When prices are high and there is a lack of financial assistance, many living in places with limited grocery stores find themselves in a situation where they are unable to get the food they need.[40] Another domain to food deserts is that they also tend to be found where poor minority communities reside.[40] Sometimes the issue with urban food deserts is not the lack of food in the area, but rather not enough nutritional knowledge about food.[41]
According to research conducted by Tulane University in 2009, 2.3 million Americans lived more than one mile away from a super market and did not own a car.[42] For those that live in these urban food deserts oftentimes they do not have access to culturally appropriate foods.[42] For many people, who have health restrictions and food allergies, the effects of food deserts are further compounded.[42] The time and cost it takes for people to go to the grocery store makes fast food more desirable.[42] There is also a price variance when it comes to small grocery stores that affect people in lower income areas from purchasing healthier food options. Smaller grocery stores can be more expensive than the larger chains.[42]
Oftentimes urban food deserts are applied to North America and Europe, however in recent years the term has been extended to Africa as well. It has taken time for researchers to understand Africa's urban food deserts because the conventional understanding of the term must be reevaluated to fit Africa's unconventional supermarkets.[42] There are three categories for food deserts: ability-related, assets-related, and attitude-related.[42] Ability-related food deserts are “anything that physically prevents access to food which a consumer otherwise has the financial resources to purchase and the mental desire to buy”.[42] An asset-related food desert involves the absence of financial assets, thus preventing consumption of desirable food that is otherwise available.[42] Lastly there are attitude-related food deserts any state of mind that prevents the consumer from accessing foods they can otherwise physically bring into their home and have the necessary assets to procure.[42] In Cape Town, South Africa supermarkets take up a large portion of retail space.[42] While supermarkets are expanding in poor neighborhoods in Cape Town, their food insecurity is growing at an alarming rate.[42] This is one of the biggest road blocks when understanding food deserts. Based on the European or American understanding of food deserts the fact that there is access to supermarkets by definition would mean that Cape Town does not suffer from food deserts.[42] Not only does Africa suffer from food deserts, but there is a direct link between climate change and the rapid growth of food deserts.[42] While supermarkets are expanding to areas that once did not have supermarkets there is still a disparity when it comes to physical access.[42] In the city of Cape Town asset-related urban food deserts are the main reason for the food insecurity, where people in this area are unable to afford the food that they would prefer to eat.[42]
Climate change plays an important role in urban food deserts because it directly affects accessibility. The main way that climate change affects food security and food deserts is that it reduces the production of food.[42] With limited availability of a product the price rises making it unavailable to those that cannot afford more expensive commodities.[42] In Cape Town specifically supermarkets rely directly on fresh produce from the nearby farm area.[42] Not only does climate change affect the production of food, but it can also damage capital assets that affect accessibility and utilization.[42] Specifically in Cape Town the access to food deserts does not change the severity of food deserts.[42] With limited diversity in their diets those that live in Cape Town are highly dependent on foods of low nutritional value and high calorific value.[42] Utilizing the European or American definition of food deserts does not take into account the dynamic market of other cultures and countries.
Crime pays an important role in food deserts. Where businesses cannot operate safely they tend to close, or relocate to more stable areas. Operating a business in a high crime area is more costly than doing so in a stable area, as security can be a significant cost. Periods of civil unrest can accelerate the flight of businesses in areas where the expectation of safe operation is low.[43] Following the 2020 riots, Chicago had more food deserts than before.[44]
Beyond physical access
The primary criterion for a food desert is its proximity to a healthy food market. When such a market is in reach for its residents, a food desert ceases to exist. But this does not mean that residents will now choose to eat healthy. A longitudinal study of food deserts in JAMA Internal Medicine shows that supermarket availability is generally unrelated to fruit and vegetable recommendations and overall diet quality.
The availability of unhealthy foods at supermarkets may affect this relationship because they tempt customers to purchase precooked foods which tend to contain more preservatives. Supermarkets may have such an adverse effect because they put independently owned grocery stores out of business. Independently owned grocery stores have the benefit of being made of the community so they can be more responsive to community needs.[42] Therefore, simply providing healthier food access, according to Janne Boone-Heinonen et al., cannot completely eliminate food deserts, this access must be paired with education.[45][46]
In a 2018 article in Guernica, Karen Washington states that factors beyond physical access suggest the community should reexamine the word food desert itself. She believes "food apartheid" more accurately captures the circumstances surrounding access to affordable nutritious foods. Washington says, "When we say food apartheid the real conversation can begin." [47]
Access to food options is not the only barrier to healthier diets and improved health outcomes. Wrigley et al. collected data before and after a food desert intervention to explore factors affecting supermarket choice and perceptions regarding healthy diet in Leeds, United Kingdom. Pretests were administered prior to a new store opening and post-tests were delivered 2 years after the new store had opened. The results showed that nearly half of the food desert residents began shopping at the newly built store, however, only modest improvements in diet were recorded.[48]
A similar pilot study conducted by Cummins et al. focused on a community funded by the Pennsylvania Fresh Food Financing Initiative. They conducted follow up after a grocery store was built in a food desert to assess the impact. They found that "simply building new food retail stores may not be sufficient to promote behavior change related to diet."[48] Studies like these show that living close to a store stocked with fruits and vegetables does not make an impact on food choices.[48]
A separate survey also found that supermarket and grocery store availability did not generally correlate with diet quality and fresh food intake.[42] Pearson et al. further confirmed that physical access is not the sole determinant of fruit and vegetable consumption.[48] Impediments common with places that are not food deserts remain.
Work and family
People who have nonstandard work hours, including rotating or evening shifts may have difficulty shopping at stores that close earlier and instead opt to shop at fast food or convenience stores that are generally open later.[23][48] Under welfare-to-work reforms enacted in 1996, a female adult recipient must log 20 hours a week of "work activity" to receive SNAP benefits.[49] If they live in a food desert and have family responsibilities, working as well may limit time to travel to obtain nutritious foods as well as prepare healthful meals and exercise.[49]
Safety and store appearance
Additional factors may include how different stores welcome different groups of people[23] and nearness to liquor stores.[50] Residents in a 2010 Chicago survey complained that in-store issues like poor upkeep and customer service were also impediments.[50] Safety can also be an issue for those in high crime areas, especially if they have to walk carrying food and maybe also with a child or children.[50]
Fast food
A possible factor affecting obesity and other "diet-related diseases" is the proximity of fast-food restaurants and convenience stores compared to "full-access" grocery stores.[18] Proximity to fast-food restaurants correlates with a higher BMI, while proximity to a grocery store correlates with a lower BMI, according to one study.[18]
A 2011 review used fifteen years of data from the Coronary Artery Risk Development in Young Adults (CARDIA) study to examine the fast-food consumption of more than 5,000 young American adults aged 18–30 years in different geographic environments.[42] The study found that fast-food consumption was directly related to the proximity of fast food restaurants among low-income participants. The research team concluded that "alternative policy options such as targeting specific foods or shifting food costs (subsidization or taxation)" may be complementary and necessary to promote healthy eating habits while increasing the access to large food stores in specific regions and limit the availability of fast-food restaurants and small food stores.[42] Some cities already restrict the location of fast-food and other food retailers that do not provide healthy food.[51]
Fast-food restaurants are disproportionately placed in low-income and minority neighborhoods and are often the closest and cheapest food options.[42] "People living in the poorest SES areas have 2.5 times the exposure to fast-food restaurants as those living in the wealthiest areas".[52] Multiple studies were also done in the US regarding racial/ethnic groups and the exposure to fast-food restaurants. One study in South Los Angeles, where there is a higher percentage of African Americans, found that there was less access to healthier stores and more access to fast food compared to West Los Angeles, which has a lower African American population. In another study in New Orleans, it was found that communities that were predominantly African American had 2.4 fast-food restaurants per square mile while predominantly white neighborhoods had 1.5 fast-food restaurants per square mile.[53] Researchers found that fast-food companies purposely target minority neighborhoods when conducting market research to open new fast-food restaurants. Existing segregation makes it easier for fast-food companies to identify these target neighborhoods. This practice increases the concentration of fast-food restaurants in minority neighborhoods.[54]
Behavior and social and cultural barriers
The likelihood of being food insecure for Latinos is 22.4%, for African Americans 26.1% and for whites, 10.5%.[55] People who are food insecure often will find themselves having to cut back more at the end of the month when their finances or food stamps run out. Month to month, there are other special occasions that may warrant higher spending on food such as birthdays, holidays, or and unplanned events.[56] Because people who are food insecure are still fundamentally involved in society, so they are faced with the other stressors of life as well as the additional frustration or guilt that comes with not being able to feed themselves or their family.[56]
Other studies have documented a sense of loyalty towards the owners of neighborhood convenience stores as an explanation as to why residents may not change their shopping behaviors.[12]
Steven Cummins also proposed that food availability is not the problem: it is eating habits.[57] Pearson et al. urge food policy to focus on the social and cultural barriers to healthy eating.[58] For instance, New York City's public-private Healthy Bodegas Initiative has aimed to encourage bodegas to carry milk and fresh produce and residents to purchase and consume them.[59]
Pharmacies
In addition to the close proximity of fast-food restaurants and convenience stores, many lower-income communities contain a higher prevalence of pharmacies when compared to medium or high-income communities. [60] These stores often contain a high number of snack foods, such as candy, sugary beverages, and salty snacks that are within arms reach of a cash register in 96% of pharmacies. [61] While pharmacies are important in these communities, they act as yet another convenience store, further exposing low-income residents to non-nutritional food.
Nutrition
| Age Group | Gender | Recommended Calories |
|---|---|---|
| Young Children | Boy/Girl | 1000-2000 |
| Adolescent | Boy/Girl | 1400-3200 (depending on physical activity) |
| Adult | Female | 1600-2400 |
| Adult | Male | 2000-3200 |
Regardless of daily caloric intake, if a person does not eat foods that are rich in vitamins and nutrients they are susceptible to diseases related to malnutrition. These diseases include scurvy which results from low vitamin C levels, rickets from low vitamin D levels, and pellagra from insufficient nicotinic acid.[63] Nutrient imbalances can affect a person, especially a developing child in a multitude of ways. Studies show that malnutrition in children can cause problems with academic performance, attention span, and motivation.[64]
Since 2006, the United States has seen an increase in cases of obesity.[65] There are not accessible grocery stores in many food deserts, so people do not have the option of eating fresh produce. Instead, they have access to cheap, fast, and easy food which typically contains excess fats, sugars, and carbohydrates. Examples of such foods include chips, candy, and soda. Several diseases can result from consuming large amounts of these unhealthy food options, including cardiovascular disease, hypertension, diabetes, osteoporosis ,and even cancer.[66]
Fresh produce provides the body with nutrients that help it function effectively. Vegetables are good sources of fiber, potassium, folate, iron, manganese, choline, and vitamins A, C, K, E, B6 and many more.[62] Fruits are good sources of fiber, potassium, and vitamin C. The USDA recommends eating the whole fruit instead of fruit juice because juice itself has less fiber and added sugars.[62] Dairy products contain nutrients such as calcium, phosphorus, riboflavin, protein, and vitamins A, D and B-12. Protein, a good source of vitamin B and lasting energy, can be found in both plant and animal products.[62] The USDA also suggests to limit the percentage of daily calories for sugars (<10%), saturated fats (<10%) and sodium (<2300 mg).[62] Although small amounts of sugars, fats, and sodium are necessary for the body, they can lead to various diseases when consumed in large amounts.
Processed foods
Even knowing the importance of nutrition, an additional barrier people may face is whether they even have the choice. Corner stores often only carry processed food, eliminating the choice of eating fresh. Processed food encompasses any type of food that has been modified from its original state whether from washing, cooking, or adding preservative or other additives. Because it is such a general category, processed foods can be broken down into four more specific groups: "unprocessed or minimally processed foods, processed culinary ingredients, processed foods (PFs), and ultra-processed foods and drinks (UPFDs)."[67]
The original motivation for processing foods was to preserve them so there would be less food waste and there would be enough food to feed the population.[65] By canning or drying fruits and vegetables to try and preserve them, some of the nutrients are lost and oftentimes sugar is added, making the product less healthy than when it was fresh. Similarly, with meats that are dried, there is salt added to help in preservation but results in the meat has a higher sodium content.[65] The ultra-processed foods were not made to be nutrient-rich, but rather to satisfy cravings with high amounts of salts or sugars, so they result in people eating more than they should of food that has no nutritional value.[67] Processed foods may also be made rich with nutrients that many people are lacking in their diets, making up for the lack of fresh food.[68] Some nutritionists may recommend eliminating processed foods from diets, while others see it as a way to reduce food scarcity and malnutrition.[65] In 1990 the Nutrition Labeling and Education Act required nutrition labels on food, making it so people could see what and how much of something they were consuming. With that labeling what some companies did was list things that were not added on the front, but rarely did they add information about nutrients they added.[65] Scientists and nutritionists are looking into ways to create affordably, processed food that is high in essential nutrients and vitamins that also taste good so the consumer is inclined to buy them.[65]
Alcohol
Many areas that are food deserts have disproportionately high numbers of liquor stores. For example, East Oakland has 4 supermarkets and 40 liquor stores.[69] These communities are also often predominantly populated by ethnic minorities. Both Latinos and African Americans are predisposed to disease resulting from alcohol consumption. Some alcohol-related illnesses include stroke, hypertension, diabetes, colon and GI cancer, and obesity. Some studies show that moderating one's alcohol consumption can reduce one's chance of getting cardiovascular disease and even extend one's mental stability into old age.[66]
Implications for self care
Self-care is an essential component in the management of chronic conditions and for those who are healthy. Self-care is greatly influenced by food choices and dietary intake.[66] Limited access to nutritious foods in food deserts can greatly impact one's ability to engage in healthy practices. Access, affordability, and health literacy are all social determinants of health, which are accentuated by living in a food desert.[12] There are two main health implications for those living in food deserts: overnutrition or undernutrition.[66] The community may be undernourished, due to no access to food stores. The community may be over-nourished due to a lack of affordable supermarkets with whole foods and a higher concentration of convenience stores and fast-food restaurants that offer prepackaged foods often high in sugar, fat, and salt.[66] Food-insecurity remains a problem for many low-income families, but the greatest challenge to living in a food desert is poor diet quality. Living in a food desert contributes to a higher prevalence of chronic diseases associated with being overweight.[66] Persons living in a food desert often face barriers to self-care, particularly in accessing resources needed to change their dietary habits.
Transportation and geography
People tend to make food choices based on what is available in their neighborhood. In food deserts there is often a high density of fast-food restaurants and corner stores that offer prepared and processed foods.[5]
In rural areas, food security is a major issue. Food security can imply either a complete lack of food, which contributes to undernourishment, or a lack of nutritious food, which contributes to over-nourishment.[5]
According to the United States Department of Agriculture (USDA),[70] community food security "concerns the underlying social, economic, and institutional factors within a community that affect the quantity and quality of available food and its affordability or price relative to the sufficiency of financial resources available to acquire it."[71] Rural areas tend have higher food insecurity than urban areas. This insecurity occurs because food choices in rural areas are often restricted because transportation is needed to access a major supermarket or a food supply that offers a wide, healthy variety of foods, versus smaller convenience stores that do not offer as much produce.[71]
It is critical to look at car ownership in relation to the distance and number of stores in the area. Distance from shops influences the quality of food eaten.[5] A vehicle or access to public transportation is often needed to go to a grocery store. When neither a car nor public transportation is available, diets are rarely healthy. This is because fast food and convenience stores are easier to access and do not cost much money or time. Further, those who walk to food shops typically have poorer diets, which has been attributed to having to carry shopping bags home.[5]
Adherence
Long-term adherence to a healthful, balanced diet is essential to promote the well-being of individuals and society. Many approaches to helping people eat a healthy, balanced diet are ineffective because of "adherence problems" with behavior changes.[72] Dietary adherence is influenced by habits that develop over a lifetime.[8]
It is especially difficult to "adhere" to a prescribed diet and lifestyle (ex. low-salt diet, low-fat diet, low-carbohydrate diet, low-sugar diet) when living in a food desert without enough access to items needed. When high-sugar, high-fat, and high-salt items are the only foods available to people living in a food desert, dietary adherence requires (a) shift in lifestyle/eating habits and (b) access to fresh, healthy, affordable foods.[8]
Decision-making
Decision-making is an important component of self-care that is affected by food deserts. People employ both rational and naturalistic decision-making processes on a routine basis. Naturalistic decisions occur in situations where time is limited, stakes are high, needed information is missing, the situation is ambiguous and the decision-maker is uncertain. Rational decisions are more likely when people have time to weigh options and consider the consequences.[73]
The way individuals living in a food desert make decisions about healthy eating is influenced by a variety of factors. Communities with higher than state average poverty statistics often report low access to affordable food, thus limiting their ability to maintain a healthy diet.[15] For these families living in poverty, many people work multiple jobs with rotating or evening shifts that make it difficult to find time to shop for food.[7][74] Time constraints affect decision-making and people often choose to go to a closer convenience store rather than travel farther for fresh food.[75] Families in urban food deserts may lack access to a car, which adds to the time needed to shop for groceries.[8] Additionally, convenience stores and corner stores are typically open later hours than traditional grocery stores, making them more accessible.[76]
Another factor that impacts those living in a food desert is safety. High rates of crime are a barrier for those living in food deserts.[77] If people feel unsafe traveling farther to a grocery store, they are more likely to decide to purchase less healthy options at a closer location. In this way, people prioritize their safety over fresh, healthy foods.[77]
Proximity to fast-food restaurants also influences decisions made when choosing meals. How close an individual is to a fast food restaurant is correlated to having a higher BMI, while proximity to a grocery store is associated with a lower BMI.[78] One study found that people living in the poorest areas of the country have more than twice the exposure to fast-food restaurants compared to people living in wealthy areas.[79] Another study used 15 years of data from the Coronary Artery Risk Development in Young Adults (CARDIA) study to examine the fast-food consumption of more than 5,000 young American adults aged 18–30 years in different geographic areas of the US.[45] Proximity to fast food or a supermarket/grocery store was used to predict the type of food consumed.[45] In low-income study participants, the type of food consumed was directly related to the proximity of fast food restaurants.[45] These results suggest that low-income persons living in a food desert make decisions to consume fast-food based on proximity to fast-food restaurants versus distances to a grocery store.[45]
Health literacy
While access poses a major barrier to the practice of self-care in food deserts, health literacy remains a common barrier to nutritional behavioral choices. Health literacy and food deserts can affect all sectors of the population, but it is known that they both disproportionately affect underserved, low-income individuals.[80] Health literacy is the ability to obtain, read, understand, and use health information in order to make appropriate health decisions and follow instructions for treatment.[81] Health literacy affects the ability to perform self-care by influencing decision-making and relationships with health care professionals. Additionally, health literacy and self-efficacy can predict the likelihood of reading food labels, which predicts dietary choices.[82] A study of young adults in a metropolitan area found that those with low health literacy used food labels significantly less than a high health literacy group, suggesting that low health literacy may negatively influence dietary quality.[82] Overall, this data suggests that health literacy is a key factor in explaining differences in dietary habits, as healthy eating is associated with higher nutrition literacy skills.[83][84]
When considering health literacy and dietary self-care behavior, a study of persons with heart failure found that those with low health knowledge had poor self-care behaviors.[85] This study reveals how health literacy influences one's ability to manage a health condition and make healthy choices. Gaining access to fresh and affordable food is essential to improving health and decreasing social disparities in those living in food deserts. Increasing health education and resources to improve health literacy are also vital for individuals to engage in healthy behaviors, adhere to dietary recommendations, and practice self-care.
Impact
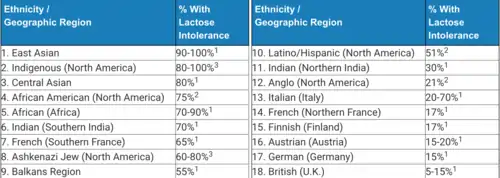
All of the aforementioned limitations to nutritional foods have serious consequences for marginalized groups, as they are disproportionately represented in food deserts. Subsequently, dietary-related diseases continue to have a proportionately large impact in these communities. This can be seen in studies examining diabetes and lactose intolerance. 4.9 million non-Hispanic African Americans aged 20 years or older have diagnosed diabetes, according to the Centers for Disease Control (CDC) national survey data. In the United States, some degree of lactose indigestion occurs in an estimated 15% (6% to 19%) of Caucasians, 53% of Mexican Americans, 62% to 100% of Native Americans, 75-80% of African Americans, and 90% of Asian Americans.[86] Additionally, racial and ethnic minorities have a higher prevalence of diabetes as compared to whites, and have a higher rate of complication post-diabetes diagnosis.[87]

In the long term, this can have crippling effects on the poorest Americans. “Chronic diet-related diseases can cause further financial struggles, producing expensive medical bills and making work difficult. In 2006, people with obesity paid an average of $1,429 more in medical expenses than the average American. Obesity is least prevalent among adults in the highest economic bracket.” [88]
A 2019 study published in The Quarterly Journal of Economics cast doubt on the notion that exposing poor neighborhoods to healthy groceries reduces nutritional inequality.[89] The study found "that exposing low-income households to the same products and prices available to high-income households reduces nutritional inequality by only about 10 percent, while the remaining 90 percent is driven by differences in demand."[89] Another study found that grocery stores are more closely spaced in poor neighborhoods; and that there was no relation between children's food consumption, weight, and the type of food available near their homes.[90] Another study suggested that adding a grocery store near one's home was associated with an average BMI decrease of 0.115, very small compared to the excess BMI of an obese person.[91][92]
Initiatives and resources
Recognition of food deserts as a major public health concern has prompted a number of initiatives to address the lack of resources available for those living in both urban and rural areas. On the larger scale, there have been national public policy initiatives.
Federal and state policy initiatives
The United States government responded to food insecurity with several programs, one of which being the Domestic Nutrition Assistance Programs (DNAPs). Other programs include the Supplemental Nutrition Assistance Program (SNAP), the Special Supplement Nutrition Program for Women, Infants, and Children (WIC), and food pantries and emergency kitchens. However, there is still a significant lack of legislation on local and state levels to adequately address the problem efficiently. As food insecurity has reached drastic levels, significant pressure for the government to qualify the problem as a human rights issue, which has proven futile.[93]
In 2010, the US Department of Health and Human Services, the US Department of Agriculture, and the US Department of the Treasury announced their partnership in the development of the Healthy Food Financing Initiative (HFFI). Intending to expand access to healthy food options in both urban and rural communities across the country, HFFI has helped expand and develop grocery stores, corner stores, and farmers' markets, by providing financial and technical assistance to communities. The creation of these resources provides nutritious food options to those living in food deserts.[94] The HFFI has awarded $195 million to community development organizations in 35 states. Between 2011 and 2015, HFFI created or supported 958 projects aimed at healthy food access.[95]
The HFFI has also supported the development of statewide programs across the country, in California, Colorado, Illinois, Louisiana, Michigan, New Jersey, New York, Ohio, and Pennsylvania.[96] In Pennsylvania, the state program called the Fresh Food Financing Initiative (FFFI) provides grants and loans to healthy food retailers to create or renovate markets, including supermarkets, small stores, and farmers' markets, in low income urban and rural areas across Pennsylvania. Because operating in underserved areas is more financially straining on retailers, the program provides subsidized financing incentives for retailers to open in areas where the need is high. The Pennsylvania program's success influenced many other states to launch similar programs.[97]
Farmers' markets and community gardens
Local and community efforts have made strides in combating a lack of access to nutritious food in food deserts. Farmers' markets provide residents with fresh fruits and vegetables. Usually, in public and central areas of a community, such as a park, farmers' markets are most effective when they are easily accessible. Farmers' markets tend to be more successful in urban than rural areas due to large geographic distances in rural areas that make the markets difficult to access.[98] The expansion of SNAP to farmers' markets also helps make nutritious foods increasingly affordable. Each year, SNAP program participants spend around $70 billion in benefits; as of 2015, more than $19.4 billion were redeemed at farmers' markets.[99] The Double Up Food Bucks program doubles what every Electronic Benefit Transfer (EBT) dollar spent at a farm stand is worth.[100] This incentivizes locals to shop for fresh foods rather than processed foods. Community gardens can play a similar role in food deserts, generating fresh produce by having residents share in the maintenance of food production.[101]
The Food Trust, a nonprofit organization based in Pennsylvania, has 22 farmers' markets in operation throughout Philadelphia. To increase accessibility for healthier food and fresh produce, Food Trust farmers' markets accept SNAP benefits.[102] Customers have reported improved diets with an increase in vegetable intake as well as healthier snacking habits.[103] Community gardens also address fresh food scarcity. The nonprofit group DC Urban Greens operates a community garden in Southeast Washington, D.C., an area labeled by the US Department of Agriculture as a food desert. The garden provides fresh produce to those in the city who do not have easily accessible grocery stores nearby. The organization also sets up farmers' markets in the city.[104] In the food desert of North Las Vegas, a neighborhood with one of the highest levels of food insecurity, another community garden is addressing food scarcity.[105] These community gardens can aid in education and access to new foods. Organizations such as the Detroit Black Community Food Security Network use community-building gardens to promote community around healthy food.[106]
Meal delivery, food trucks, and ride shares
An entrepreneurial solution to food insecurity in food deserts is food trucks. In major urban centers such as Boston, mobile food markets travel to low-income areas with fresh produce. The trucks travel to assisted living communities, schools, workplaces, and health centers.[107] The increased availability of online food retailers and delivery services, such as AmazonFresh and FreshDirect, can also help in food deserts by delivering food straight to residences. The ability of elderly people, disabled people, and those who live geographically far from supermarkets to use SNAP benefits online to order groceries is a major resource.[108] For those who lack transportation options, vehicle for hire services may be vital resources to increase access to nutritious foods in food deserts.[109]
Geisinger Health Services Fresh Food Pharmacy
In central Pennsylvania, an innovative solution to food insecurity for persons with diabetes is the Fresh Food Pharmacy, which considers access to nutritious foods as vital as access to prescription medicine. Free groceries, all compliant with the American Diabetes Association guidelines, are provided to those in this program.[110] This unique program to address food insecurity for those with chronic illnesses is a major resource for promoting self-care in food deserts.
Youth education
Food deserts are a result of lack of access to food and not enough money to afford the available food, which causes many people and especially children to not get enough nutrients their bodies require. Because there is a dominant concern of where the next meal will come from, people do not always care what they are putting in their bodies as long as it will keep them alive. The Grow Hartford Program was implemented in a school in Connecticut to have students address an issue in their community and they chose to focus on food justice.[111] The youth involved worked on farms in the area to learn about the processes of food production and the importance and variety of vegetables. The program even led kids to start a community garden at their school. This program allowed the students to engage in hands-on learning to educate them about agriculture, food scarcity, and nutrition while helping bridge the gap of food access for some of their peers who could now bring home food from the surrounding farms or the school garden.[111]
See also
References
- "The Community for Science-Based Nutrition | American Nutrition Association". americannutritionassociation.org. Retrieved 2017-11-17.
- Story, Mary; Kaphingst, Karen M.; Robinson-O'Brien, Ramona; Glanz, Karen (2008). "Creating healthy food and eating environments: policy and environmental approaches". Annual Review of Public Health. 29: 253–272. doi:10.1146/annurev.publhealth.29.020907.090926. ISSN 0163-7525. PMID 18031223.
- "Food, Conservation, and Energy Act of 2008, 110th Cong, 2nd Sess, HR 6124, Title VII" (PDF). Retrieved November 17, 2017.
- "Food Oasis :: Washington State Department of Health". Archived from the original on 2019-04-21. Retrieved 2018-02-11.
- Coveney, John; O'Dwyer, Lisel A (2009). "Effects of mobility and location on food access". Health & Place. 15 (1): 45–55. doi:10.1016/j.healthplace.2008.01.010. PMID 18396090.
- Diaz de Villegas, Carolina; Rodriguez, Kiara. "Medley Food Desert Project" (PDF). Florida International University Department of Biological Sciences.
- Lee, Courtney Hall (2017-02-23). "Grocery Store Inequity". Sojourners. Retrieved 2017-11-17.
- "Living in a Food Desert: How Lack of Access to Healthy Foods Can Affect Public Health | Notes From NAP". notes.nap.edu. 2011-01-25. Retrieved 2017-11-17.
- Shaw, Hillary John (December 2003). "1.1. Origin of the term `Food Desert'" (PDF). The Ecology of Food Deserts (Thesis). The University of Leeds School of Geography. p. 11. Retrieved August 9, 2017.
- Cummins, S; MacIntyre, S (2002). "'Food deserts'—evidence and assumption in health policy making". BMJ. 325 (7361): 436–8. doi:10.1136/bmj.325.7361.436. PMC 1123946. PMID 12193363.
- Ford, Paula B; Dzewaltowski, David A (2008). "Disparities in obesity prevalence due to variation in the retail food environment: Three testable hypotheses". Nutrition Reviews. 66 (4): 216–28. doi:10.1111/j.1753-4887.2008.00026.x. PMID 18366535. S2CID 14769196.
- Walker, Renee E.; Keane, Christopher R.; Burke, Jessica G. (2010). "Disparities and access to healthy food in the United States: A review of food deserts literature". Health & Place. 16 (5): 876–84. doi:10.1016/j.healthplace.2010.04.013. PMID 20462784.
- Morton, Lois Wright; Blanchard, Troy C. (2007). "Starved for access: life in rural America's food deserts" (PDF). Rural Realities. 1 (4): 1–10. Archived from the original (PDF) on 2013-10-21. Retrieved 2013-07-28.
- Reisig, V.; Hobbiss, A. (2000). "Food deserts and how to tackle them: A study of one city's approach". Health Education Journal. 59 (2): 137–49. CiteSeerX 10.1.1.1005.1078. doi:10.1177/001789690005900203.
- Hendrickson, Deja; Smith, Chery; Eikenberry, Nicole (2006). "Fruit and vegetable access in four low-income food deserts communities in Minnesota". Agriculture and Human Values. 23 (3): 371–83. doi:10.1007/s10460-006-9002-8.
- Larsen, Kristian; Gilliland, Jason (2009). "A farmers' market in a food desert: Evaluating impacts on the price and availability of healthy food". Health & Place. 15 (4): 1158–62. doi:10.1016/j.healthplace.2009.06.007. PMID 19631571.
- "USDA ERS - Access to Affordable, Nutritious Food Is Limited in "Food Deserts"". www.ers.usda.gov. Retrieved 2018-05-23.
- Ver Ploeg, M.; Breneman, V.; Farrigan, T.; Hamrick, K.; Hopkins, D.; Kaufman, P.; Lin, B-H.; Nord, M.; Smith, TA.; Williams, R.; Kinnison, K.; Olander, C.; Singh, A.; Tuckermanty, E. (Jun 2009). "Access to Affordable and Nutritious Food: Measuring and Understanding Food Deserts and Their Consequences: Report to Congress" (PDF). Administrative Publication (AP-036). Retrieved August 6, 2017.
- Liese, Angela D.; Hibbert, James D.; Ma, Xiaoguang; Bell, Bethany A.; Battersby, Sarah E. (2014). "Where Are the Food Deserts? An Evaluation of Policy-Relevant Measures of Community Food Access in South Carolina". Journal of Hunger & Environmental Nutrition. 9 (1): 16–32. doi:10.1080/19320248.2013.873009. PMC 4540074. PMID 26294937.
- "Measuring the Food Environment in Canada". Food and Nutrition. Health Canada. 11 Oct 2013. Retrieved 13 Nov 2016.
- United States Department of Agriculture-Economic Research Service. Food Access Research Atlas (formerly known as the Food desert locator). Available at: http://www.ers.usda.gov/data-products/food-access-research-atlas.aspx.
- Ver Ploeg, M.; Dutko, P.; Breneman, V. (2014). "Measuring Food Access and Food Deserts for Policy Purposes". Applied Economic Perspectives and Policy. 37 (2): 205–25. doi:10.1093/aepp/ppu035.
- Phillips, Anna Lena (2011). "Making Better Maps of Food Deserts: Neighborhoods with little or no access to healthful food can be located and studied using GIS mapping". American Scientist. 99 (3): 209–210. doi:10.1511/2011.90.209. JSTOR 23019314.
- Wang, Haoluan; Qiu, Feng; Swallow, Brent (2014). "Can community gardens and farmers' markets relieve food desert problems? A study of Edmonton, Canada". Applied Geography. 55: 127–37. doi:10.1016/j.apgeog.2014.09.010.
- Ploeg, Michele. "Access to Affordable and Nutritious Food: Updated Estimates of Distance to Supermarkets Using 2010 Data" (PDF). A Report from the Economic Research Service. United States Department of Agriculture Economic Research Service. Archived from the original (PDF) on 2017-04-30.
- Jiao, Junfeng; Moudon, Anne V.; Ulmer, Jared; Hurvitz, Philip M.; Drewnowski, Adam (2012). "How to Identify Food Deserts: Measuring Physical and Economic Access to Supermarkets in King County, Washington". American Journal of Public Health. 102 (10): e32–9. doi:10.2105/AJPH.2012.300675. PMC 3490650. PMID 22897554.
- Bauer, Katherine W. (2004, January 201). Price and Availability Matter. From The New York Times: https://www.nytimes.com/roomfordebate/2011/01/23/can-wal-mart-make-us-healthier/access-to-healthy-foods-and-lower-prices-matter
- "Healthy Bodegas Initiative CEO Internal Program Review Report" (PDF). New York, NY: New York City Department of Health and Mental Hygiene. 2008. p. 17. Archived from the original (PDF) on August 23, 2017. Retrieved July 20, 2017.
- Access to affordable and nutritious food: Measuring and understanding food deserts and their consequences: Report to Congress. Washington, D.C.: U.S. Dept. of Agriculture, Economic Research Service. Jun 2009. Web. 10 Nov 2016.
- "What Happened When Whole Foods Tried to Challenge Elitism, Racism, and Obesity in Detroit". Slate Magazine. Retrieved 2017-12-14.
- Treuhaft, Sarah; Karpyn, Allison (2010). "The Grocery Gap" (PDF). PolicyLink.
- Morton, Lois (2007). "Rural Realities" (PDF). Rural Realities.
- United States Department of Agriculture-Economic Research Service. Rural income, poverty, and welfare report. Available at: http://www.ers.usda.gov/topics/rural-economy-population/rural-poverty-well-being.aspx.
- "Food Deserts". Cotati, CA: Food Empowerment Project. Retrieved July 14, 2017.
- "National Poverty Center | University of Michigan". www.npc.umich.edu. Retrieved 2016-11-08.
- Smith, Chery; Morton, Lois W. (2009). "Rural Food Deserts: Low-income Perspectives on Food Access in Minnesota and Iowa". Journal of Nutrition Education and Behavior. 41 (3): 176–87. doi:10.1016/j.jneb.2008.06.008. PMID 19411051.
- Anderson, Timothy J.; Saman, Daniel M.; Lipsky, Martin S.; Lutfiyya, M. Nawal (2015-10-01). "A cross-sectional study on health differences between rural and non-rural U.S. counties using the County Health Rankings". BMC Health Services Research. 15 (1): 441. doi:10.1186/s12913-015-1053-3. ISSN 1472-6963. PMC 4590732. PMID 26423746.
- Caspi, Caitlin E.; Kawachi, Ichiro; Subramanian, S. V.; Adamkiewicz, Gary; Sorensen, Glorian (October 2012). "The relationship between diet and perceived and objective access to supermarkets among low-income housing residents". Social Science & Medicine. 75 (7): 1254–1262. doi:10.1016/j.socscimed.2012.05.014. ISSN 1873-5347. PMC 3739049. PMID 22727742.
- "Food for the Cities: Food security, nutrition and livelihoods". www.fao.org. Retrieved 2018-10-31.
- MacNell, Lillian; Elliott, Sinikka; Hardison-Moody, Annie; Bowen, Sarah (2017-03-13). "Black and Latino Urban Food Desert Residents' Perceptions of Their Food Environment and Factors That Influence Food Shopping Decisions". Journal of Hunger & Environmental Nutrition. 12 (3): 375–393. doi:10.1080/19320248.2017.1284025. ISSN 1932-0248.
- "Stop Blaming Food Deserts for the Nutrition Gap". CityLab. Retrieved 2018-10-04.
- "Food Deserts In America (Infographic)". socialwork.tulane.edu. Retrieved 2018-10-31.
- "Walmart, Target, CVS, Apple closing stores in some locations over George Floyd protests". ABC7 Chicago. June 1, 2020.
- Marissa Parra (7 June 2020). "Chicago's South Side Left With Few Food Options After Weekend Violence". CBS Chicago. Retrieved 7 June 2020.
Chicago now has food deserts in places that weren’t food deserts before. “Bronzeville Mariano’s was looted, the Walmart on 47th was looted
- Boone-Heinonen, Janne; Gordon-Larsen, P; Kiefe, C. I.; Shikany, J. M.; Lewis, C. E.; Popkin, B. M. (2011). "Fast Food Restaurants and Food Stores". Archives of Internal Medicine. 171 (13): 1162–70. doi:10.1001/archinternmed.2011.283. PMC 3178268. PMID 21747011.
- Gilligan, Heather Tirado (2014-02-10). "Food Deserts Aren't the Problem". Slate. ISSN 1091-2339. Retrieved 2016-12-12.
- Brones, Anna (May 7, 2018). "Karen Washington: It's Not a Food Desert, It's Food Apartheid". Guernica. Retrieved May 25, 2018.
- Wrigley, Neil; Warm, Daniel; Margetts, Barrie (2003). "Deprivation, Diet, and Food-Retail Access: Findings from the Leeds 'Food Deserts' Study". Environment and Planning A. 35: 151–88. doi:10.1068/a35150.
- Correll, Michael (2010). "Getting Fat on Government Cheese: The Connection Between Social Welfare Participation, Gender, and Obesity in America". Duke Journal of Gender Law & Policy. 18: 45–77. SSRN 1921920.
- Illinois Advisory Committee to the United States Commission on Civil Rights (October 2011). "Food Deserts in Chicago" (PDF). Washington, DC: United States Commission on Civil Rights. p. 7.
- Unger, Serena; Wooten, Heather (June 21, 2009). A Food Systems Assessment for Oakland, CA: Toward a Sustainable Food Plan (PDF). Oakland, CA: Oakland Mayor's Office of Sustainability, University of California, Berkeley, Department of City and Regional Planning. pp. 65–66. Archived from the original (PDF) on August 4, 2016.
- Ming-Chen Yeh and David L. Katz. "Food, Nutrition, and the Health of Urban Populations". In Cities and the Health of the Public (Nicholas Freudenberg, Sandro Galea, and David Vlahov, eds.). Vanderbilt University Press (2006), pp. 106-127. ISBN 0-8265-1512-6.
- Hilmers, Angela; Hilmers, David; Dave, Jayna (2012). "Neighborhood Disparities in Access to Healthy Foods and Their Effects on Environmental Justice". American Journal of Public Health. 102 (9): 1644–1654. doi:10.2105/AJPH.2012.300865. PMC 3482049. PMID 22813465.
- Kwate, Naa Oyo A (2008). "Fried chicken and fresh apples: Racial segregation as a fundamental cause of fast food density in black neighborhoods". Health & Place. 14 (1): 32–44. doi:10.1016/j.healthplace.2007.04.001. PMID 17576089.
- Sharma, Shreela V. "Multidisciplinary approaches to address food insecurity and nutrition among youth and their families". Journal of Applied Research on Children: Informing Policy for Children at Risk. 6 (2).
- Messer, Ellen; Ross, Elizabeth M (2002). "Talking to Patients About Food Insecurity". 5 (2). Cite journal requires
|journal=(help) - "Why it takes more than a grocery store to eliminate a 'food desert'". PBS NewsHour. Retrieved 2017-03-21.
- Pearson, Tim; Russell, Jean; Campbell, Michael J.; Barker, Margo E. (2005). "Do 'food deserts' influence fruit and vegetable consumption?—a cross-sectional study". Appetite. 45 (2): 195–197. doi:10.1016/j.appet.2005.04.003. PMID 15927303.
- Dannefer, Rachel; Williams, Donya A; Baronberg, Sabrina; Silver, Lynn (2012). "Healthy Bodegas: Increasing and Promoting Healthy Foods at Corner Stores in New York City". Am J Public Health. 102 (10): e27–e31. doi:10.2105/AJPH.2011.300615. PMC 3490666. PMID 22897534.
- Ohri-Vachaspati, Punam; DeWeese, Robin S.; Acciai, Francesco; DeLia, Derek; Tulloch, David; Tong, Daoqin; Lorts, Cori; Yedidia, Michael J. (July 2019). "Healthy Food Access in Low-Income High-Minority Communities: A Longitudinal Assessment—2009–2017". International Journal of Environmental Research and Public Health. 16 (13). doi:10.3390/ijerph16132354. ISSN 1661-7827. PMC 6650883. PMID 31277250.
- Whitehouse, Anne; Simon, Anna; French, Simone A.; Wolfson, Julian (June 2012). "Availability of snacks, candy and beverages in hospital, community clinic and commercial pharmacies". Public Health Nutrition. 15 (6): 1117–1123. doi:10.1017/S1368980011003600. ISSN 1475-2727. PMID 22277097.
- DIETARY GUIDELINES FOR AMERICANS 2015-2020 Eight Edition (PDF). U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015.
- Evan Grivetti, Louis (March 1978). "Culture, Diet, and Nutrition: Selected Themes and Topics". BioScience. 28 (3): 171–177. doi:10.2307/1307345. JSTOR 1307345.
- Alaimo, Katherine (July 2001). "Food Insufficiency and American School-Aged Children's Cognitive, Academic, and Psychosocial Development". Pediatrics. 108 (1): 44–53. PMID 11433053.
- Weaver, Connie M; Dwyer, Johanna; Fulgoni, Victor L; King, Janet C; Leveille, Gilbert A; MacDonald, Ruth S; Ordovas, Jose; Schnakenberg, David (2014). "Processed foods: Contributions to nutrition". The American Journal of Clinical Nutrition. 99 (6): 1525–42. doi:10.3945/ajcn.114.089284. PMC 6410904. PMID 24760975.
- Dietary Guidelines for Americans 2010 (PDF). Washington DC: U.S. Department of Agriculture and U.S. Department of Health and Human Services. 2010.
- Gibney, Michael J; Forde, Ciarán G; Mullally, Deirdre; Gibney, Eileen R (2017). "Ultra-processed foods in human health: A critical appraisal". The American Journal of Clinical Nutrition. 106 (3): 717–24. doi:10.3945/ajcn.117.160440. PMID 28793996.
- "The Debate Over the Health Effects of Food Processing | American Society for Nutrition". American Society for Nutrition. 2017-09-11. Retrieved 2018-03-12.
- Alkon, Alison Hope; Block, Daniel; Moore, Kelly; Gillis, Catherine; Dinuccio, Nicole; Chavez, Noel (2013). "Foodways of the urban poor". Geoforum. 48: 126–135. doi:10.1016/j.geoforum.2013.04.021.
- "USDA". www.usda.gov. Retrieved 2017-11-18.
- "Rural Hunger and Access to Healthy Food Introduction - Rural Health Information Hub". www.ruralhealthinfo.org. Retrieved 2017-11-18.
- Middleton, Kathryn R; Anton, Stephen D; Perri, Michal G (2013). "Long-Term Adherence to Health Behavior Change". American Journal of Lifestyle Medicine. 7 (6): 395–404. doi:10.1177/1559827613488867. PMC 4988401. PMID 27547170.
- Broadstock, Marita; Michie, Susan (2000). "Processes of patient decision making: Theoretical and methodological issues". Psychology & Health. 15 (2): 191–204. doi:10.1080/08870440008400300.
- Phillips, Anna Lena (2011). "Making Better Maps of Food Deserts". American Scientist. 99 (3): 209. doi:10.1511/2011.90.209.
- Correll, Michael (2010). "Getting Fat on Government Cheese: The Connection Between Social Welfare Participation, Gender, and Obesity in America" (PDF). Duke Journal of Gender Law & Policy. 18: 45–77.
- Coleman-Jensen, Alisha J (2010). "Working for Peanuts: Nonstandard Work and Food Insecurity Across Household Structure". Journal of Family and Economic Issues. 32: 84–97. doi:10.1007/s10834-010-9190-7.
- Food Deserts in Chicago (PDF). Illinois Advisory Committee to the United States Commission on Civil Rights. October 2011.
- "USDA ERS - Access to Affordable and Nutritious Food-Measuring and Understanding Food Deserts and Their Consequences: Report to Congress". www.ers.usda.gov. Retrieved 2017-11-17.
- Cities and the health of the public. Freudenberg, Nicholas., Galea, Sandro., Vlahov, David. (1st ed.). Nashville [Tenn.]: Vanderbilt University Press. 2006. ISBN 978-0826515124. OCLC 558991544.CS1 maint: others (link)
- Rodriguez, Judith C (2011). "Serving the Public: Health Literacy and Food Deserts". Journal of the American Dietetic Association. 111 (1): 14. doi:10.1016/j.jada.2010.11.009. PMID 21185958.
- Facilitating state health exchange communication through the use of health literate practices : workshop summary. Hewitt, Maria Elizabeth., Institute of Medicine (U.S.). Roundtable on Health Literacy., Institute of Medicine (U.S.). Board on Population Health and Public Health Practice. Washington, D.C.: National Academies Press. 2012. ISBN 9780309220293. OCLC 785387000.CS1 maint: others (link)
- Cha, Eunseok; Kim, Kevin H; Lerner, Hannah M; Dawkins, Colleen R; Bello, Morenike K; Umpierrez, Guillermo; Dunbar, Sandra B (2014). "Health Literacy, Self-efficacy, Food Label Use, and Diet in Young Adults". American Journal of Health Behavior. 38 (3): 331–9. doi:10.5993/ajhb.38.3.2. PMC 4039409. PMID 24636029.
- Silk, Kami J; Sherry, John; Winn, Brian; Keesecker, Nicole; Horodynski, Mildred A; Sayir, Aylin (2008). "Increasing Nutrition Literacy: Testing the Effectiveness of Print, Web site, and Game Modalities". Journal of Nutrition Education and Behavior. 40 (1): 3–10. doi:10.1016/j.jneb.2007.08.012. PMID 18174098.
- Carbone, Elena T; Zoellner, Jamie M (2012). "Nutrition and Health Literacy: A Systematic Review to Inform Nutrition Research and Practice". Journal of the Academy of Nutrition and Dietetics. 112 (2): 254–65. doi:10.1016/j.jada.2011.08.042. PMID 22732460.
- Matsuoka, Shiho; Tsuchihashi-Makaya, Miyuki; Kayane, Takahiro; Yamada, Michiyo; Wakabayashi, Rumi; Kato, Naoko P; Yazawa, Miyuki (2016). "Health literacy is independently associated with self-care behavior in patients with heart failure". Patient Education and Counseling. 99 (6): 1026–32. doi:10.1016/j.pec.2016.01.003. PMID 26830514.
- Miller, Gregory D., et al. “Dairy Foods and Hypertension.” Handbook of Dairy Foods and Nutrition, Second Edition, 1999, p. 327., doi:10.1201/9781420050189.ch3.
- Edward A. Chow, MD, Henry Foster, MD, Victor Gonzalez, MD and LaShawn McIver, MD, MPH.Clinical Diabetes 2012 Jul; 30(3): 130-133.
- “The Food Gap: Income Inequality and Disease Disparity.” Harvard Political Review The Food Gap Income Inequality and Disease Disparity Comments, harvardpolitics.com/culture/food-gap/.
- Allcott, Hunt; Diamond, Rebecca; Dubé, Jean-Pierre; Handbury, Jessie; Rahkovsky, Ilya; Schnell, Molly (2019-05-20). "Food Deserts and the Causes of Nutritional Inequality". The Quarterly Journal of Economics. 134 (4): 1793–1844. doi:10.1093/qje/qjz015. ISSN 0033-5533.
- Lee, Helen (2012). "The role of local food availability in explaining obesity risk among young school-aged children". Social Science & Medicine. 74 (8): 1193–203. doi:10.1016/j.socscimed.2011.12.036. PMID 22381683.
- Cowen, Tyler (2013-04-04). "Are there "food deserts" as a dietary problem?". Marginal REVOLUTION. Retrieved 2020-04-04.
- Hattori, Aiko; An, Ruopeng; Sturm, Roland (2013-03-14). "Neighborhood Food Outlets, Diet, and Obesity Among California Adults, 2007 and 2009". Preventing Chronic Disease. Centers for Disease Control and Prevention (CDC). 10. doi:10.5888/pcd10.120123. ISSN 1545-1151. PMID 23489640.
- Elsheikh, Elsadig. “Structural Racialization and Food Insecurity in the United States.” Haas Institute for a Fair and Inclusive Society, 2013, p. 2.
- "Healthy Food Financing Initiative". US Department of Health & Human Services. Retrieved November 17, 2017.
- "The Food Trust | The Success of HFFI". thefoodtrust.org. Retrieved 2017-11-17.
- "Healthy Food Financing Initiatives Across the Country" (PDF). The Food Trust. Retrieved November 17, 2017.
- "The Pennsylvania Fresh Food Financing Initiative" (PDF). American Heart Association. Archived from the original (PDF) on 2018-05-09. Retrieved November 17, 2017.
- McCracken, Vicki. "Do Farmers' Markets Ameliorate Food Deserts?" (PDF). University of Wisconsin. Retrieved November 17, 2017.
- "SNAP - Farmers Market Coalition". Farmers Market Coalition. Retrieved 2017-11-17.
- "How it works at Farmers Markets – Double Up Food Bucks". www.doubleupfoodbucks.org. Retrieved 2017-11-17.
- "Food Desert | Gateway to Health Communication | CDC". www.cdc.gov. 2017-09-15. Retrieved 2017-11-17.
- "The Food Trust | At Farmers Markets". thefoodtrust.org.
- Institute of Medicine and National Research Council (2009). The Public Health Effects of Food Deserts: Workshop Summary. Washington, DC: The National Academies Press. ISBN 978-0-309-14068-3.
- "D.C. urban gardens bring low-cost, fresh produce to city's food deserts". PBS NewsHour. 2016-11-24. Retrieved 2017-11-17.
- "Community Garden is Oasis in Middle of Food Desert in Las Vegas | NRCS Nevada". www.nrcs.usda.gov. Retrieved 2017-11-17.
- White, Monica M (2011). "Sisters of the Soil: Urban Gardening as Resistance in Detroit". Race/Ethnicity: Multidisciplinary Global Contexts. 5 (1): 13–28. doi:10.2979/racethmulglocon.5.1.13.
- Field, Anne. "In Boston, A Mobile Market For Food Deserts". Forbes. Retrieved 2017-11-17.
- West, Jack Karsten and Darrell (2017-08-29). "How the Amazon-Whole Foods merger shrinks food deserts". Brookings. Retrieved 2017-11-17.
- Lowenstein, Mark (May 8, 2017). "Uber needs a win. It could start by helping people in 'food deserts' access healthy foods". Recode.
- "Fresh Food By Prescription: This Health Care Firm Is Trimming Costs — And Waistlines". NPR.org. Retrieved 2017-11-17.
- Roselle, René; Connery, Chelsea (2016). "Food Justice: Access, Equity, and Sustainability for Healthy Students and Communities". Kappa Delta Pi Record. 52 (4): 174–7. doi:10.1080/00228958.2016.1223993.