Meckel–Gruber syndrome
Meckel-Gruber syndrome is a rare, lethal, ciliopathic, genetic disorder, characterized by renal cystic dysplasia, central nervous system malformations (occipital encephalocele), polydactyly (post axial), hepatic developmental defects, and pulmonary hypoplasia due to oligohydramnios. Meckel–Gruber syndrome is named for Johann Meckel and Georg Gruber.[1][2][3]
| Meckel syndrome | |
|---|---|
| Other names | Meckel–Gruber syndrome, Gruber syndrome, Dysencephalia splanchnocystica |
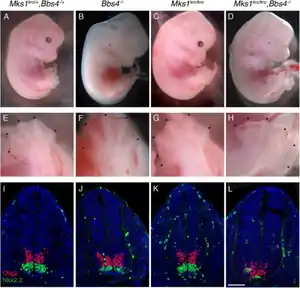 | |
| Embryos with mutation in MKS1KRC, a cause of Meckel syndrome. | |
| Specialty | Medical genetics |
Pathophysiology
Meckel–Gruber syndrome (MKS) is an autosomal recessive lethal malformation. Recently, two MKS genes, MKS1 and MKS3, have been identified. A study done recently has described the cellular, sub-cellular and functional characterization of the novel proteins, MKS1 and meckelin, encoded by these genes.[4] The malfunction of this protein production is mainly responsible for this lethal disorder.
| Type | OMIM | Gene |
|---|---|---|
| MKS1 | 609883 | MKS1 |
| MKS2 | 603194 | TMEM216 |
| MKS3 | 607361 | TMEM67 |
| MKS4 | 611134 | CEP290 |
| MKS5 | 611561 | RPGRIP1L |
| MKS6 | 612284 | CC2D2A |
| MKS7 | 608002 | NPHP3 |
| MKS8 | 613846 | TCTN2 |
| MKS9 | 614144 | B9D1 |
| MKS10 | 611951 | B9D2 |
Relation to other rare genetic disorders
Recent findings in genetic research have suggested that a large number of genetic disorders, both genetic syndromes and genetic diseases, that were not previously identified in the medical literature as related, may be, in fact, highly related in the genetypical root cause of the widely varying, phenotypically-observed disorders. Thus, Meckel–Gruber syndrome is a ciliopathy. Other known ciliopathies include primary ciliary dyskinesia, Bardet–Biedl syndrome, polycystic kidney and liver disease, nephronophthisis, Alström syndrome, and some forms of retinal degeneration.[5] The MKS1 gene has been identified as being associated with a ciliopathy.[6]
Diagnosis
Dysplastic kidneys are prevalent in over 95% of all identified cases. When this occurs, microscopic cysts develop within the kidney and slowly destroy it, causing it to enlarge to 10 to 20 times its original size. The level of amniotic fluid within the womb may be significantly altered or remain normal, and a normal level of fluid should not be criteria for exclusion of diagnosis.
Occipital encephalocele is present in 60% to 80% of all cases, and post-axial polydactyly is present in 55% to 75% of the total number of identified cases. Bowing or shortening of the limbs are also common.
Finding at least two of the three phenotypic features of the classical triad, in the presence of normal karyotype, makes the diagnosis solid. Regular ultrasounds and pro-active prenatal care can usually detect symptoms early on in a pregnancy.
Management
There is no cure to the disease. Treatment is symptomatic and to make the baby as comfortable as possible.[7]
Prognosis
The disease is lethal. Most infants that are not stillborn with Meckel syndrome die within hours to days of birth.[8] The longest survival time reported in medical literature is 28 months.[9]
Incidence
While not precisely known, it is estimated that the general rate of incidence, according to Bergsma,[10] for Meckel syndrome is 0.02 per 10,000 births. According to another study done six years later, the incidence rate could vary from 0.07 to 0.7 per 10,000 births.[11]
This syndrome is a Finnish heritage disease. Its frequency is much higher in Finland, where the incidence is as high as 1.1 per 10,000 births. It is estimated that Meckel syndrome accounts for 5% of all neural tube defects there.[12]The Leicestershire Perinatal Mortality Survey for the years 1976 to 1982 had found high incidences of Meckel syndrome in Gujarati Indian immigrants.[13]
References
- synd/2055 at Who Named It?
- J. F. Meckel. Beschreibung zweier durch sehr ähnliche Bildungsabweichungen entstellter Geschwister. Deutsches Archiv für Physiologie, 1822, 7: 99–172.
- G. B. Gruber. Beiträge zur Frage "gekoppelter" Missbildungen (Akrocephalossyndactylie und Dysencephalia splancnocystica. Beitr path Anat, 1934, 93: 459–476.
- Dawe HR, Smith UM, Cullinane AR, Gerrelli D, Cox P, Badano JL, Blair-Reid S, Sriram N, Katsanis N, Attie-Bitach T, Afford SC, Copp AJ, Kelly DA, Gull K, Johnson CA (2007). "The Meckel–Gruber Syndrome proteins MKS1 and meckelin interact and are required for primary cilium formation". Human Molecular Genetics. 16 (2): 173–186. doi:10.1093/hmg/ddl459. PMID 17185389.
- Badano, Jose L.; Norimasa Mitsuma; Phil L. Beales; Nicholas Katsanis (Sep 2006). "The Ciliopathies : An Emerging Class of Human Genetic Disorders". Annual Review of Genomics and Human Genetics. 7: 125–148. doi:10.1146/annurev.genom.7.080505.115610. PMID 16722803.
- Kyttälä, Mira (May 2006). "Identification of the Meckel Syndrome Gene (MKS1) Exposes a Novel Ciliopathy" (PDF). National Public Health Institute, Helsinki. Archived from the original (PDF) on 2006-07-21. Retrieved 2008-07-06. Cite journal requires
|journal=(help) - "Meckel Syndrome". NORD (National Organization for Rare Disorders). Retrieved 2019-12-02.
- Kheir, Abdelmoneim E. M.; Imam, Abdelmutalab; Omer, Ilham M.; Hassan, Ibtsama M.A.; Elamin, Sara A.; Awadalla, Esra A.; Gadalla, Mohammed H.; Hamdoon, Tagwa A. (2012). "Meckel-Gruber syndrome: A rare and lethal anomaly". Sudanese Journal of Paediatrics. 12 (1): 93–96. ISSN 0256-4408. PMC 4949827. PMID 27493335.
- Barisic, Ingeborg; Boban, Ljubica; Loane, Maria; Garne, Ester; Wellesley, Diana; Calzolari, Elisa; Dolk, Helen; Addor, Marie-Claude; Bergman, Jorieke EH; Braz, Paula; Draper, Elizabeth S (June 2015). "Meckel–Gruber Syndrome: a population-based study on prevalence, prenatal diagnosis, clinical features, and survival in Europe". European Journal of Human Genetics. 23 (6): 746–752. doi:10.1038/ejhg.2014.174. ISSN 1018-4813. PMC 4795048. PMID 25182137.
- Bergsma, D. (1979). "Birth Defects". Atlas and Compendium. London: Macmillan Press.
- Salonen, R.; Norio, R.; Reynolds, James F. (1984). "The Meckel syndrome: Clinicopathological Findings in 67 Patients". American Journal of Medical Genetics. 18 (4): 671–689. doi:10.1002/ajmg.1320180414. PMID 6486167.
- Nyberg, D. A.; et al. (1990). "Meckel–Gruber syndrome; Importance of Prenatal Diagnosis". Journal of Ultrasound in Medicine. 9 (12): 691–696. doi:10.7863/jum.1990.9.12.691. PMID 2277397. S2CID 25658017.
- Young, I. D.; Rickett, A. B.; Clarke, M. (1985-08-01). "High incidence of Meckel's syndrome in Gujarati Indians". Journal of Medical Genetics. 22 (4): 301–304. doi:10.1136/jmg.22.4.301. ISSN 0022-2593. PMC 1049454. PMID 4045959.
External links
| Classification | |
|---|---|
| External resources |