Sprained ankle
A sprained ankle, also known as a twisted ankle, or rolled ankle is an injury where sprain occurs on one or more ligaments of the ankle.
| Sprained ankle | |
|---|---|
| Other names | Twisted ankle, rolled ankle |
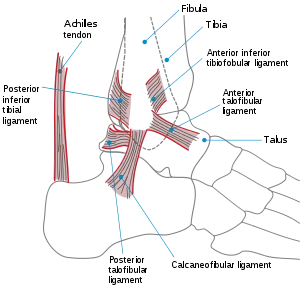 | |
| Lateral view of the human ankle | |
| Specialty | Orthopedics, sports medicine, Physical medicine and rehabilitation, Family medicine |
| Symptoms | Swelling, bruising, pain |
| Diagnostic method | Physical examination |
| Differential diagnosis | Maisonneuve fracture, high ankle sprain |
| Treatment | Physical medicine and rehabilitation |
Signs and symptoms
Knowing the symptoms that can be experienced with a sprain is important in determining that the injury is not really a break in the bone. When a sprain occurs, broken blood vessels will hemorrhage into the tissue that surrounds the joint, causing a visible bruise. White blood cells responsible for inflammation migrate to the area, and blood flow increases as well.[1] Along with this inflammation, swelling and pain is experienced. The nerves in the area become more sensitive when the injury is suffered, so pain is felt as throbbing and will worsen if there is pressure placed on the area. Warmth and redness are also seen as blood flow is increased. Also there is a decreased ability to move the joint.
 Right foot, housed in an air brace, has become swollen as a result of a more severe 2nd degree sprain to the ankle.
Right foot, housed in an air brace, has become swollen as a result of a more severe 2nd degree sprain to the ankle. Right foot. A light 2nd degree sprain, two days after injury.
Right foot. A light 2nd degree sprain, two days after injury. Right foot, 3rd degree sprain. One day after injury.
Right foot, 3rd degree sprain. One day after injury.
Cause
Movements – especially turning, and rolling of the foot – are the primary cause of an ankle sprain.[2]
The risk of a sprain is greatest during activities that involve explosive side-to-side motion, such as tennis, skateboarding or basketball. Sprained ankles can also occur during normal daily activities such as stepping off a curb or slipping on ice. Returning to activity before the ligaments have fully healed may cause them to heal in a stretched position, resulting in less stability at the ankle joint. This can lead to a condition known as Chronic Ankle Instability (CAI), and an increased risk of ankle sprains.
The following factors can contribute to an increased risk of ankle sprains:
- Weak muscles/tendons that cross the ankle joint, especially the muscles of the lower leg that cross the outside, or lateral aspect of the ankle joint (i.e. peroneal or fibular muscles);
- Weak or lax ligaments that join together the bones of the ankle joint – this can be hereditary or due to overstretching of ligaments as a result of repetitive ankle sprains;
- Inadequate joint proprioception (i.e., sense of joint position);
- Slow neuron muscular response to an off-balance position;
- Running on uneven surfaces;
- Shoes with inadequate heel support; and
- Wearing high-heeled shoes – due to the weak position of the ankle joint with an elevated heel, and a small base of support.
Ankle sprains occur usually through excessive stress on the ligaments of the ankle. This can be caused by excessive external rotation, inversion or eversion of the foot caused by an external force. When the foot is moved past its range of motion, the excess stress puts a strain on the ligaments. If the strain is great enough to the ligaments past the yield point, then the ligament becomes damaged, or sprained.[3][4]
Diagnosis
The diagnosis of a sprain relies on the medical history, including symptoms, as well as making a differential diagnosis, mainly in distinguishing it from strains or bone fractures. The Ottawa ankle rule is a simple, widely used rule to help differentiate fractures of the ankle or mid-foot from other ankle injuries that do not require x-ray radiography. It has a sensitivity of nearly 100%, meaning that a patient who tests negative, according to the rule almost certainly does not have an ankle fracture.[5] If ankle pain is persistent 6-8 weeks after initial sprain, MRI imaging of the joint can be considered to rule out peroneal tendon, osteochondral, or syndesmotic injury.
Classification of severity
Ankle sprains are classified grade 1, 2, and 3.[6] Depending on the amount of damage or the number of ligaments that are damaged, each sprain is classified from mild to severe. A grade 1 sprain is defined as mild damage to a ligament or ligaments without instability of the affected joint. A grade 2 sprain is considered a partial tear to the ligament, in which it is stretched to the point that it becomes loose. A grade 3 sprain is a complete tear of a ligament, causing instability in the affected joint.[7] Bruising may occur around the ankle.[8]
Inversion (lateral) ankle sprain
The most common type of ankle sprain occurs when the foot has a force, typically body weight, causing it to internally rotated to a higher degree than it is supposed to, affecting the lateral side of the foot. When this type of ankle sprain happens, the outer, or lateral, ligaments are stretched too much. The anterior talofibular ligament is one of the most commonly involved ligaments in this type of sprain, followed by the calcaneofibular ligament[9] and posterior talofibular ligament[9] respectively, the later found in more severe ankle sprains. Approximately 70–85% of ankle sprains are inversion injuries.

When the ankle becomes inverted, the anterior talofibular and calcaneofibular ligaments are damaged. This is the most common ankle sprain.
Eversion (medial) ankle sprain
A less common type of ankle sprain is called an eversion injury, affecting the medial side of the foot. This happens when, instead of the ankle rotating medially resulting in an inversion injury (the foot rolling too much to the inside), the ankle rotates laterally resulting in an eversion injury (when the foot rolls too much to the outside). When this occurs, the medial, or deltoid, ligament is strained.
High (syndesmotic) ankle sprain
A high ankle sprain is an injury to the large ligaments above the ankle that join together the two long bones of the lower leg, called the tibia and fibula. High ankle sprains commonly occur from a sudden and forceful outward twisting of the foot. This commonly occurs in contact and cutting sports such as football, rugby, ice hockey, roller derby, basketball, volleyball, lacrosse, softball, baseball, track, ultimate frisbee, soccer, tennis and badminton and horse riding.
Treatment
Initial treatment commonly consists of rest, icing, compression and elevation (which is often referred to by the mnemonic RICE or sometimes PRICE with P being "protection"). These elements have been recommended by physicians for decades for the treatment of soft tissue damage, and sprained ankles, one of the most common soft tissue injuries. RICE helps limit the amount of swelling to the area, and "facilitates venous and lymphatic drainage".[10] While nearly universally accepted as a treatment, there is insufficient evidence to determine its relative effectiveness as therapy for acute ankle sprains in adults,[11] and the National Athletic Trainers Association notes that most of the rationale for using RICE or individual components is based largely on low-quality clinical trials and laboratory studies with uninjured participants or animal models[12]
Conservative measures

Ice is often used to reduce swelling in cycles of 15–20 minutes on and 20–30 minutes off. Icing an ankle too long can cause cold injuries, which is indicated by the area turning white.[13] Also, it is often recommended that ice not be applied directly to the skin, but should have a thin buffer between the ice and the affected area, and some professionals think ice need not be applied at all. Recently, Gabe Mirkin, MD, who coined and popularized the acronym RICE in his The Sports Medicine Book in 1978, now has some issues with the "i" in RICE. After reviewing modern studies, he notes that because ice closes off the blood vessels, "ice doesn’t increase healing—it delays it." and now advises skipping ice altogether unless needed to reduce pain from swelling.[14] Still, it is widely accepted and, although the clinical evidence is sparse, cryotherapy (ice) has been a mainstay of clinical practice for rehabilitation specialists.
In uncomplicated lateral ankle sprains, swelling of the soft tissue can be prevented with compression around both malleoli, elevation of the injured ankle higher than the heart, and pain-free exercises.[15]
An orthopedic walking boot is often used for the treatment of a sprained ankle injury. Braces and crutches are also used to help alleviate the pain so the injured ankle can heal as quickly and painlessly as possible.
Although found to be less effective than casts, compression bandages are used to provide support and compression for sprained ankles. Wrapping is started at the ball of the foot and slowly continued up to the base of the calf muscle; this allows the swelling to travel up toward the center of the body so that it does not gather in the foot.
Rehabilitation and recovery
Many different types of rehabilitation exercises can be done to aid an ankle sprain regardless of the severity of the injury. The purpose of rehabilitation gives the ability for the ankle to regain strength and flexibility. A sprained ankle becomes swollen due to the increased amount of edema within the tissue, since this physiological effect is the foundation of the pain the decline of edema is the main goal during the beginning of rehabilitation.[16] This can be done instantly by implementing the RICE mechanism which is resting the ankle, applying ice, compressing, and elevating it.[10] The emphasis of the first week of rehabilitation should be on protecting the ankle to avoid further damage. As the healing progresses, stress can be applied by different mechanisms until the ankle is fully recovered.[17] The key to a fast recovery is to implement all the different types of ankle sprain exercises so that the range of motion will increase while the pain is decreasing.[18]
In cases where the ankle does not heal in an appropriate amount of time, other exercises need to be implemented so that strength and flexibility can be regained. Physical therapists assign different types of ankle sprain exercises that deal with ankle flexibility, strengthening, balance, and agility. If an ankle sprain does not heal properly, the joint may become unstable and may lead to chronic pain.[19] Receiving proper treatment and performing exercises that promote ankle function is important to strengthen the ankle and prevent further injury.
Ankle immobilization
A short period of immobilization in a below-knee cast or in an Aircast leads to a faster recovery at 3 months compared to a tubular compression bandage.[20] In contrast, a randomized controlled trial has concluded that appropriate exercise immediately after a sprain improves function and recovery.[21] These exercises were focused on increasing ankle range of movement, activation and strengthening of ankle musculature, and restoring normal sensorimotor control, and were carried out for 20 minutes, three times a day.[21] After the injury, it is advisable not to walk for a couple of days. Bed rest will help to accelerate the healing process and eliminate the chance of mishandling the affected limb. Driving vehicles or operating machinery should not be attempted.
The amount of therapy that a person can handle will depend on their level of pain and the grade of sprain they experienced. It is not recommended to return to sports or extreme physical activities until hopping on the ankle is possible without pain. Wearing high-top tennis shoes may also help prevent ankle sprains if the shoes used are laced snugly and if the ankle is taped with a wide, nonelastic adhesive tape.[22]
Ankle mobilization/manipulation
For acute ankle sprains, manual joint mobilization/manipulation of the ankle has been found to diminish pain and increase range of motion. For treatment of subacute/chronic lateral ankle sprains, these techniques improved ankle range-of-motion, decreased pain and improved function.[23]
Ankle exercises
To prevent sprains or re-injury from occurring, strengthening and stretching exercises should be done through a full range of ankle motion. To improve ankle mobility, ankle circles can be performed by extending the legs in front of the body and then moving the foot up and down, side to side, or rotating the foot in a circle. Another common exercise to improve mobility, as well as proprioception, is to use the toes to draw the letters of the alphabet in the air. Most importantly, the lateral aspect of the ankle joint should be strengthened with eversion exercises (i.e., underside of the foot is turned outward against resistance) to improve lateral ankle stability.[24] Stretching is also an important component of a strengthening program, to help maintain joint flexibility.
Balance and stability training are especially important to retrain the ankle muscles to work together to support the joint.[25] This includes exercises that are performed by standing on one foot and using the injured ankle to lift the body onto its toes. To further enhance balance and stability, exercise devices such as the wobble board can be used, progressing from double-leg to single-leg stance, first with eyes open and then with eyes closed, for enhanced effectiveness.
Flexibility exercises
An example of a flexibility exercise is a towel stretch [26] and writing the alphabet with toes which will increase the range of motion.
Strengthening exercises
Ankle strengthening exercises are step ups and walking on toes which will strengthen the muscles around the swollen area.
Balance exercises
Balance exercises include the use of a balance board, which helps the whole body function to maintain balance. The use of balance boards has been shown to produce significantly positive results in gaining proper balance.[27]
Agility exercises

Plyometrics exercises such as squat jumps and power skipping should not be implemented until the ankle has regained full agility.
Other strategies that can be used to prevent ankle injury include:
- Ensure proper warm-up prior to stretching and activity;
- When running, choose level surfaces and avoid rocks or holes;
- Ensure that shoes have adequate heel support;
- If high-heeled shoes are worn, ensure that heels are no more than 2 inches in height, and avoid heels with a narrow base.
Prognosis
Most people improve significantly in the first two weeks. However, some still have problems with pain and instability after one year (5–30%). Re-injury is also very common.[28]
Epidemiology

Ankle sprains can occur through either sports or activities of daily living, and individuals can be at higher or lower risk depending on a variety of circumstances including their homeland, race, age, sex, or profession.[29] In addition, there are different types of ankle sprains such as eversion ankle sprains and inversion ankle sprains. Overall, the most common type of ankle sprain to occur is an inversion ankle sprain, where excessive plantar flexion and supination cause the anterior talofibular ligament to be affected. A study showed that for a population of Scandinavians, inversion ankle sprains accounted for 85% of all ankle sprains.[27] Most ankle sprains occur in more active people, such as athletes and regular exercisers.
Previous ankle sprains
When an ankle sprain occurs, subsequent ankle sprains are much more likely to follow.[30] The rate of recurrence is particularly high for athletes in high-risk sports.[31] The most widely recommended preventative measures for recurring sprains are wearing ankle-protective gear[32] (tape, or ankle brace) and implementing exercises designed to strengthen the ankle and improve one's balance (e.g., balance ball exercises). In a review article of ankle sprain prevention research, the authors reference a season-long study on a group of soccer players. 60 players wore ankle-protective (tape or ankle-braces) throughout the soccer season, and another 171 players were enrolled in the control group, as they wore no ankle protective gear. At the end of the season, 17% of the players who did not wear ankle braces/tape sprained their ankles, while only 3% of the players who wore protection incurred the same injury. Amongst the players who sprained their ankles and did not wear ankle-protective gear, 25% had a history of previous ankle sprains.[33] Another peer-reviewed article references a study which concluded that ankle exercising could decrease the risk of recurring sprains by 11%.[34]
Age
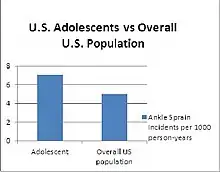
In a study comparing the prevalence of ankle sprains between age, race, and sex, individuals who were aged 10–19 years old had highest instances of ankle sprains.[35] It can be suggested that adolescents are more physically active, which leads to higher chances of ankle sprains. Since sports deal with high utilization of the ankle, over 50% of ankle sprains are due to sport-related injuries.[36]
U.S. military
Moreover, average ankle sprains for the general U.S. population are estimated at 5–7 ankle sprains for every 1000 person-years; however, a study showed that for military cadets, instances for ankle sprains were about 10 times those of the general population [37]
Male vs. female
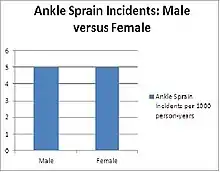
Another study comparing sex influences on ankle sprains found that male and female counterparts had similar incidence rates of ankle sprains. However, at a specific age range of 19–25 years old, males were found to have a substantially greater rate of ankle sprains than females. Furthermore, at ages 30 and over, females showed a higher incidence of ankle sprains than males.[29] From this, it can be said that age and activity levels are better indicators of ankle sprain risks than gender.
References
- Ankle Sprains Symptoms -eMedicineHealth.com, Retrieved on 22 January 2010.
- Sprained Ankle – American Academy of Orthopedic Surgeons, Retrieved on 22 January 2010.
- Wikstrom EA, Wikstrom AM, Hubbard-Turner T (2012). "Ankle sprains: treating to prevent the long-term consequences". JAAPA. 25 (10): 40–2, 44–5. doi:10.1097/01720610-201210000-00009. PMID 23115869.
- Gehring D, Wissler S, Mornieux G, Gollhofer A (2013). "How to sprain your ankle — a biomechanical case report of an inversion trauma". J Biomech. 46 (1): 175–8. doi:10.1016/j.jbiomech.2012.09.016. PMID 23078945.
- Bachmann LM, Kolb E, Koller MT, Steurer J, ter Riet G (February 2003). "Accuracy of Ottawa ankle rules to exclude fractures of the ankle and mid-foot: systematic review". BMJ. 326 (7386): 417. doi:10.1136/bmj.326.7386.417. PMC 149439. PMID 12595378.
- Moreira V, Antunes F (2008). "[Ankle sprains: from diagnosis to management. the physiatric view]". Acta Med Port (in Portuguese). 21 (3): 285–92. PMID 18674420.
- "Sprained Ankle". American Academy of Orthopedic Surgeons. Retrieved 2 November 2011.
- Stanley, James. "Sprained Ankle". North Yorkshire Orthopaedic Specialists. Retrieved 2 November 2012.
- Akbari, Mohammed; Karimi, Hossein; Farahini, Hossein; Fahgihzadeh, Soghrat (November–December 2006). "Balance problems after unilateral ankle sprains". The Journal of Rehabilitation Research and Development. 43 (7): 819–824. doi:10.1682/JRRD.2006.01.0001.
- Wolfe MW, Uhl TL, Mattacola CG, McCluskey LC (2001). "Management of ankle sprains". Am Fam Physician. 63 (1): 93–104. PMID 11195774.
- van den Bekerom MP, Struijs PA, Blankevoort L, Welling L, van Dijk CN, Kerkhoffs GM (2012). "What is the evidence for rest, ice, compression, and elevation therapy in the treatment of ankle sprains in adults?". Journal of Athletic Training. 47 (4): 435–43. doi:10.4085/1062-6050-47.4.14. PMC 3396304. PMID 22889660.
- Kaminski, Thomas W.; Hertel, Jay; Amendola, Ned; Docherty, Carrie L.; Dolan, Michael G.; Hopkins, J. Ty; Nussbaum, Eric; Poppy, Wendy; Richie, Doug (July–August 2013). "National Athletic Trainers' Association Position Statement: Conservative Management and Prevention of Ankle Sprains in Athletes" (PDF). Journal of Athletic Training. 48 (4): 528–545. doi:10.4085/1062-6050-48.4.02. PMC 3718356. PMID 23855363.
- Lifestyle and home remedies, MayoClinic.com. Retrieved 3 May 2010.
- Byrne, Sue (2015). "Why You Should Avoid Ice for a Sprained Ankle". Consumer Reports.
- Aronen JG, Garrick JG (2009). "Acute Ankle Injuries, Part 1: Office Evaluation and Management". Consultant. 49: 413–421.
Aronen JG, Garrick JG (2009). "Acute Ankle Injuries, Part 2: Treatment of Uncomplicated Lateral Ankle Sprains". Consultant. 49: 734–740. - Coté DJ, Prentice WE, Hooker DN, Shields EW (1988). "Comparison of three treatment procedures for minimizing ankle sprain swelling". Phys Ther. 68 (7): 1072–6. doi:10.1093/ptj/68.7.1072. PMID 3133668.
- Mattacola CG, Dwyer MK (2002). "Rehabilitation of the Ankle After Acute Sprain or Chronic Instability". J Athl Train. 37 (4): 413–429. PMC 164373. PMID 12937563.
- Zöch C, Fialka-Moser V, Quittan M (2003). "Rehabilitation of ligamentous ankle injuries: a review of recent studies". Br J Sports Med. 37 (4): 291–5. doi:10.1136/bjsm.37.4.291. PMC 1724658. PMID 12893710.
- Sprained Ankle Overview – Webmd.com, Retrieved on 22 January 2010.
- Lamb SE, Marsh JL, Hutton JL, Nakash R, Cooke MW (February 2009). "Mechanical supports for acute, severe ankle sprain: a pragmatic, multicentre, randomised controlled trial". Lancet. 373 (9663): 575–81. doi:10.1016/S0140-6736(09)60206-3. PMID 19217992.
- Bleakley CM, O'Connor SR, Tully MA, et al. (2010). "Effect of accelerated rehabilitation on function after ankle sprain: randomised controlled trial". BMJ. 340: c1964. doi:10.1136/bmj.c1964. PMID 20457737.
- Ankle Sprains: Healing and Preventing Injury – Family doctor.org, Retrieved on 22 January 2010.
- Loudon JK, Reiman MP, Sylvain J (2013). "The efficacy of manual joint mobilisation/manipulation in treatment of lateral ankle sprains: a systematic review". Br J Sports Med. 48 (5): 365–70. doi:10.1136/bjsports-2013-092763. PMID 23980032.
- Arnold BL, Linens SW, de la Motte SJ, Ross SE (November–December 2009). "Concentric evertor strength differences and functional ankle instability: A meta-analysis". Journal of Athletic Training. 44 (6): 653–662. doi:10.4085/1062-6050-44.6.653. PMC 2775368. PMID 19911093.
- Sprained Ankle: Treatment and Drugs – Mayo clinic.com, Retrieved on 22 January 2010.
- http://www.livestrong.com/article/470163-ankle-towel-stretch// towel stretch
- Wester JU, Jespersen SM, Nielsen KD, Neumann L (1996). "Wobble board training after partial sprains of the lateral ligaments of the ankle: a prospective randomized study". J Orthop Sports Phys Ther. 23 (5): 332–6. doi:10.2519/jospt.1996.23.5.332. PMID 8728532.
- Margo KL (December 2008). "Review: many adults still have pain and subjective instability at 1 year after acute lateral ankle sprain". Evid Based Med. 13 (6): 187. doi:10.1136/ebm.13.6.187. PMID 19043045.
- Waterman BR, Owens BD, Davey S, Zacchilli MA, Belmont PJ (2010). "The epidemiology of ankle sprains in the United States". J Bone Joint Surg Am. 92 (13): 2279–84. doi:10.2106/JBJS.I.01537. PMID 20926721.
- "Chronic Ankle Instability". www.foothealthfacts.org. Foot Health Facts. Retrieved 4 April 2018.
- Gribble PA, Delahunt E, Bleakley CM, Caulfield B, Docherty CL, Fong DT, Fourchet F, Hertel J, Hiller CE, Kaminski TW, McKeon PO, Refshauge KM, van der Wees P, Vicenzino W, Wikstrom EA (2014). "Selection criteria for patients with chronic ankle instability in controlled research: a position statement of the International Ankle Consortium". Journal of Athletic Training (Review). 49 (1): 121–7. doi:10.4085/1062-6050-49.1.14. PMC 3917288. PMID 24377963.
- Stoimenov, Vassil (17 March 2018). "How to Prevent The Injuries Most Likely to Happen to You". PositiveMed. USA: PositiveMed. Retrieved 4 April 2018.
- Gross M, Liu H (2003). "The Role of Ankle Bracing for Prevention of Ankle Sprain Injuries". J Orthop Sports Phys Ther. 33 (10): 572–577. doi:10.2519/jospt.2003.33.10.572. PMID 14620786.
- Hayman J, Prasad S, Stulberg D, Hickner J (2010). "Help patients prevent repeat ankle injury". J Fam Pract. 59 (1): 32–4. PMC 3183932. PMID 20074499.
- Bridgman SA, Clement D, Downing A, Walley G, Phair I, Maffulli N (2003). "Population based epidemiology of ankle sprains attending accident and emergency units in the West Midlands of England, and a survey of UK practice for severe ankle sprains". Emerg Med J. 20 (6): 508–10. doi:10.1136/emj.20.6.508. PMC 1726220. PMID 14623833.
- Yeung MS, Chan K, So CH, Yuan WY (1994). "An epidemiological survey on ankle sprain". Journal of Sports Medicine. 28 (2): 112–6. doi:10.1136/bjsm.28.2.112. PMC 1332043. PMID 7921910.
- Waterman BR, Belmont PJ, Cameron KL, Deberardino TM, Owens BD (2010). "Epidemiology of ankle sprain at the United States Military Academy". Am J Sports Med. 38 (4): 797–803. doi:10.1177/0363546509350757. PMID 20145281.
Further reading
- Doherty C, Bleakley C, Delahunt E, Holden S (January 2017). "Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis". British Journal of Sports Medicine (Review). 51 (2): 113–125. doi:10.1136/bjsports-2016-096178. PMID 28053200.
- McGovern RP, Martin RL (2016). "Managing ankle ligament sprains and tears: current opinion". Open Access Journal of Sports Medicine (Review). 7: 33–42. doi:10.2147/OAJSM.S72334. PMC 4780668. PMID 27042147.
- Kaminski TW, Hertel J, Amendola N, Docherty CL, Dolan MG, Hopkins JT, Nussbaum E, Poppy W, Richie D (2013). "National Athletic Trainers' Association position statement: conservative management and prevention of ankle sprains in athletes". Journal of Athletic Training (Review). 48 (4): 528–45. doi:10.4085/1062-6050-48.4.02. PMC 3718356. PMID 23855363.
- Kerkhoffs GM, van den Bekerom M, Elders LA, van Beek PA, Hullegie WA, Bloemers GM, de Heus EM, Loogman MC, Rosenbrand KC, Kuipers T, Hoogstraten JW, Dekker R, Ten Duis HJ, van Dijk CN, van Tulder MW, van der Wees PJ, de Bie RA (September 2012). "Diagnosis, treatment and prevention of ankle sprains: an evidence-based clinical guideline". British Journal of Sports Medicine. 46 (12): 854–60. doi:10.1136/bjsports-2011-090490. PMID 22522586.
External links
| Classification | |
|---|---|
| External resources |