X-ray image intensifier
An X-ray image intensifier (XRII) is an image intensifier that converts X-rays into visible light at higher intensity than the more traditional fluorescent screens can. Such intensifiers are used in X-ray imaging systems (such as fluoroscopes) to allow low-intensity X-rays to be converted to a conveniently bright visible light output. The device contains a low absorbency/scatter input window, typically aluminum, input fluorescent screen, photocathode, electron optics, output fluorescent screen and output window. These parts are all mounted in a high vacuum environment within glass or more recently, metal/ceramic. By its intensifying effect, It allows the viewer to more easily see the structure of the object being imaged than fluorescent screens alone, whose images are dim. The XRII requires lower absorbed doses due to more efficient conversion of X-ray quanta to visible light. This device was originally introduced in 1948.[1]
Operation
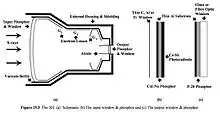
The overall function of an image intensifier is to convert incident x-ray photons to light photons of sufficient intensity to provide a viewable image. This occurs in several stages. The first is conversion of X-ray photons to light photons by the input phosphor. Sodium activated Cesium Iodide is typically used due to its high conversion efficiency thanks to high atomic number and mass attenuation coefficient.[2] The light photons are then converted to electrons by a photocathode. A potential difference (25-35 kilovolts) created between the anode and photocathode then accelerates these photoelectrons while electron lenses focus the beam down to the size of the output window. The output window is typically made of silver-activated zinc-cadmium sulfide and converts incident electrons back to visible light photons.[2] At the input and output phosphors the number of photons is multiplied by several thousands, so that overall there is a large brightness gain. This gain makes image intensifiers highly sensitive to X-rays such that relatively low doses can be used for fluoroscopic procedures.[3][4][5][6]
History
X-ray image intensifiers became available in the early 1950s and were viewed through a microscope.[7]
Viewing of the output was via mirrors and optical systems until the adaption of television systems in the 1960s.[8] Additionally, the output was able to be captured on systems with a 100mm cut film camera using pulsed outputs from an X-ray tube similar to a normal radiographic exposure; the difference being the II rather than a film screen cassette provided the image for the film to record.
The input screens range from 15–57 cm, with the 23 cm, 33 cm and 40 cm being among the most common. Within each image intensifier, the actual field size can be changed using the voltages applied to the internal electron optics to achieve magnification and reduced viewing size. For example, the 23 cm commonly used in cardiac applications can be set to a format of 23, 17, and 13 cm. Because the output screen remains fixed in size, the output appears to "magnify" the input image. High-speed digitalisation with analogue video signal came about in the mid-1970s, with pulsed fluoroscopy developed in the mid-1980s harnessing low dose rapid switching X-ray tubes. In the late 1990s image intensifiers began being replaced with flat panel detectors (FPDs) on fluoroscopy machines giving competition to the image intensifiers.[9]
Clinical applications
"C-arm" mobile fluoroscopy machines are often colloquially referred to as image intensifiers (or IIs),[10] however strictly speaking the image intensifier is only one part of the machine (namely the detector).
Fluoroscopy, using an X-ray machine with an image intensifier, has applications in many areas of medicine. Fluoroscopy allows live images to be viewed so that image-guided surgery is feasible. Common uses include orthopedics, gastroenterology and cardiology.[11] Less common applications can include dentistry.[12]
Configurations

A system containing an image intensifier may be used either as a fixed piece of equipment in a dedicated screening room or as mobile equipment for use in an operating theatre. A mobile fluoroscopy unit generally consists of two units, the X-ray generator and image detector (II) on a moveable C-arm, and a separate workstation unit used to store and manipulate the images.[13] The patient is positioned between the two arms, typically on a radiolucent bed. Fixed systems may have a c-arm mounted to a ceiling gantry, with a separate control area. Most systems arranged as c-arms can have the image intensifier positioned above or below the patient (with the X-ray tube below or above respectively), although some static in room systems may have fixed orientations.[14] From a radiation protection standpoint, under-couch (X-ray tube) operation is preferable as it reduces the amount of scattered radiation on operators and workers.[15][16] Smaller "mini" mobile c-arms are also available, primarily used to image extremities, for example for minor hand surgery.[17]
Flat panel detectors
Flat Detectors are an alternative to Image Intensifiers. The advantages of this technology include: lower patient dose and increased image quality because the X-rays are always pulsed, and no deterioration of the image quality over time. Despite FPD being at a higher cost than II/TV systems, the noteworthy changes in the physical size and accessibility for the patients is worth it, especially when dealing with paediatric patients.[9]
Feature comparison of II/TV and FPD Systems
| Feature[9] | Digital Flat Panel | Conventional II/TV |
| Dynamic range | Wide, about 5,000:1 | Limited by TV, about500:1 |
| Geometric distortion | None | Pin-cushion and ‘S-distortion |
| Detector size (bulk) | Thin profile | Bulky, significant with large FOV |
| Image area FOV | 41 x 41cm | 40cm diameter (25% less area) |
| Image quality | Better at high dose | Better at low dose |
See also
References
- Krestel, Erich (1990). Imaging Systems for Medical Diagnostics. Berlin and Munich: Siemens Aktiengesellschaft. pp. 318–327. ISBN 3-8009-1564-2.
- Wang, Jihong; Blackburn, Timothy J. (September 2000). "The AAPM/RSNA Physics Tutorial for Residents". RadioGraphics. 20 (5): 1471–1477. doi:10.1148/radiographics.20.5.g00se181471. PMID 10992034.
- Hendee, William R.; Ritenour, E. Russell (2002). Medical Imaging Physics (4th ed.). Hoboken, NJ: John Wiley & Sons. p. 237. ISBN 9780471461135.
- Schagen, P. (31 August 1979). "X-Ray Image Intensifiers: Design and Future Possibilities". Philosophical Transactions of the Royal Society A: Mathematical, Physical and Engineering Sciences. 292 (1390): 265–272. Bibcode:1979RSPTA.292..265S. doi:10.1098/rsta.1979.0060.
- Bronzino, edited by Joseph D. (2006). Medical Devices and Systems (3rd ed.). Hoboken: CRC Press. pp. 10–5. ISBN 9781420003864.CS1 maint: extra text: authors list (link)
- Singh, Hariqbal; Sasane, Amol; Lodha, Roshan (2016). Textbook of Radiology Physics. New Delhi: JP Medical. p. 31. ISBN 9789385891304.
- Airth, G. R. (31 August 1979). "X-Ray Image Intensifiers: Applications and Current Limitations". Philosophical Transactions of the Royal Society A: Mathematical, Physical and Engineering Sciences. 292 (1390): 257–263. Bibcode:1979RSPTA.292..257A. doi:10.1098/rsta.1979.0059.
- "Radiography in the 1960s". British Institute of Radiology. Retrieved 5 January 2017.
- Seibert, J. Anthony (22 July 2006). "Flat-panel detectors: how much better are they?". Pediatric Radiology. 36 (S2): 173–181. doi:10.1007/s00247-006-0208-0. PMC 2663651. PMID 16862412.
- Krettek, Christian; Aschemann, Dirk, eds. (2006). "Use of X-rays in the operating suite". Positioning Techniques in Surgical Applications. Berlin: Springer. p. 21. doi:10.1007/3-540-30952-7_4. ISBN 978-3-540-25716-5.
- "Fluoroscopy: Background, Indications, Contraindications". Medscape. 7 April 2016. Retrieved 5 January 2017.
- Uzbelger Feldman, D; Yang, J; Susin, C (2010). "A systematic review of the uses of fluoroscopy in dentistry". Chinese Journal of Dental Research. 13 (1): 23–9. PMID 20936188.
- "Fluoroscopy: Mobile Unit Operation and Safety" (PDF). American Society of Radiologic Technologists. Retrieved 21 May 2017.
- Bushberg, Jerrold T.; Seibert, J. Anthony; Leidholdt, Edwin M.; Boone, John M. The Essential Physics of Medical Imaging. Lippincott Williams & Wilkins. p. 283. ISBN 9781451153941.
- Smith, Arthur D. Smith's Textbook of Endourology. PMPH-USA. p. 13. ISBN 9781550093650.
- Mitchell, Erica L.; Furey, Patricia (January 2011). "Prevention of radiation injury from medical imaging". Journal of Vascular Surgery. 53 (1): 22S–27S. doi:10.1016/j.jvs.2010.05.139. PMID 20843625.
- Athwal, George S.; Bueno, Reuben A.; Wolfe, Scott W. (November 2005). "Radiation Exposure in Hand Surgery: Mini Versus Standard C-Arm". The Journal of Hand Surgery. 30 (6): 1310–1316. doi:10.1016/j.jhsa.2005.06.023. PMID 16344194.
