Avulsion fracture
An avulsion fracture is a bone fracture which occurs when a fragment of bone tears away from the main mass of bone as a result of physical trauma. This can occur at the ligament by the application of forces external to the body (such as a fall or pull) or at the tendon by a muscular contraction that is stronger than the forces holding the bone together. Generally muscular avulsion is prevented by the neurological limitations placed on muscle contractions. Highly trained athletes can overcome this neurological inhibition of strength and produce a much greater force output capable of breaking or avulsing a bone.
| Avulsion fracture | |
|---|---|
 | |
| Avulsion fracture of the proximal middle phalanx on the palm side | |
| Specialty | Orthopedic |
Types
Dental avulsion
Traumatic complete displacement of a tooth from its socket in alveolar bone. It is a serious dental emergency in which prompt management (within 20–40 minutes of injury) affects the prognosis of the tooth.[1]
Tuberocity avulsion of the 5th metatarsal
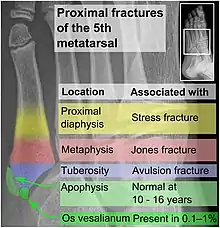
The tuberosity avulsion fracture (also known as pseudo-Jones fracture or dancer's fracture[2] is a common fracture of the fifth metatarsal (the bone on the outside edge of the foot extending to the little toe).[3] This fracture is likely caused by the lateral band of the plantar aponeurosis (tendon).[4] Most of these fractures are treated with a hard-soled shoe or walking cast. This is needed until the pain goes away and then the patient can return to normal activities.[3] Healing is usually completed within eight weeks.[5]
Tibial tuberosity avulsion

A tibial tuberosity avulsion fracture is an incomplete or complete separation of the tibial tuberosity from the tibia. This occurs as a result of a violent contraction of the quadriceps muscles, most often as a result of a high-power jump. Incomplete fractures are usually treatable with the traditional RICE (rest, ice, compression, elevation) method, but complete/displaced fractures will most often require surgery to pin the tuberosity back in place. Tibial tuberosity avulsions occur most often in teenagers that engage in a large amount of sporting activities, and many studies have shown a history with Osgood-Schlatter's disease to be linked to the fracture.
Treatment
If the fracture is small, it is usually sufficient to treat with rest and support bandage, but in more severe cases, surgery may be required. Ice may be used to relieve swelling.[6]
Displaced avulsion fractures are best managed by either open reduction and internal fixation or closed reduction and pinning. Open reduction (using surgical incision) and internal fixation is used when pins, screws, or similar hardware is needed to fix the bone fragment.
Other animals
Dinosaurs
In 2001, Bruce Rothschild and other paleontologists published a study examining evidence for tendon avulsions in theropod dinosaurs. Among the dinosaurs studied, avulsion injuries were only noted among Tyrannosaurus and Allosaurus. Scars from these sorts of injuries were limited to the humerus and scapula. A divot on the humerus of Sue the T. rex was one such avulsion. The divot appears to be located at the origin of the deltoid or teres major muscles. The localization in theropod scapulae as evidenced by the tendon avulsion in Sue suggests that theropods may have had a musculature more complex and functionally different from those of their descendants, the birds.[7]
See also
References
- Zadik Y (December 2008). "Algorithm of first-aid management of dental trauma for medics and corpsmen". Dent Traumatol. 24 (6): 698–701. doi:10.1111/j.1600-9657.2008.00649.x. PMID 19021668.
- Robert Silbergleit. "Foot Fracture". Medscape. Retrieved October 19, 2011.
- Gary A. Rosenberg & James J. Sferra (September–October 2000). "Treatment Strategies for Acute Fractures and Nonunions of the Proximal Fifth Metatarsal". Journal of the American Academy of Orthopaedic Surgeons. 8 (5): 332–338. doi:10.5435/00124635-200009000-00007.
- Richli WR, Rosenthal DI (October 1984). "Avulsion fracture of the fifth metatarsal: experimental study of pathomechanics". American Journal of Roentgenology. 143 (4): 889–91. doi:10.2214/ajr.143.4.889. PMID 6332501.
- JC DeLee (1993). RA Mann; MJ Coughlin (eds.). Fractures and dislocations of the foot. Surgery of the Foot and Ankle. 2 (6th ed.). St Louis: Mosby-Year Book. pp. 1627–1640.
- "Avulsion fracture: How is it treated?". Mayo Clinic. April 8, 2010. Retrieved April 22, 2010.
- Rothschild, B., Tanke, D. H., and Ford, T. L., 2001, Theropod stress fractures and tendon avulsions as a clue to activity: In: Mesozoic Vertebrate Life, edited by Tanke, D. H., and Carpenter, K., Indiana University Press, p. 331-336.