Colles' fracture
A Colles' fracture is a type of fracture of the distal forearm in which the broken end of the radius is bent backwards.[2] Symptoms may include pain, swelling, deformity, and bruising.[2] Complications may include damage to the median nerve.[1]
| Colles' fracture | |
|---|---|
| Other names | Colles fracture, Pouteau fracture[1] |
 | |
| An X-ray showing a Colles' fracture | |
| Specialty | Emergency medicine, orthopedics |
| Symptoms | Pain, swelling, deformity, bruising[2] |
| Usual onset | Sudden[2] |
| Causes | Fall on an outstretched hand[2] |
| Risk factors | Osteoporosis[2] |
| Diagnostic method | X-rays[2] |
| Treatment | Cast, surgery[3] |
| Prognosis | Recovery over 1 to 2 years[2] |
| Frequency | ~15% lifetime risk[3] |
It typically occurs as a result of a fall on an outstretched hand.[2] Risk factors include osteoporosis.[2] The diagnosis may be confirmed with X-rays.[2] The tip of the ulna may also be broken.[4]
Treatment may include casting or surgery.[3] Surgical reduction and casting is possible in the majority of cases in people over the age of 50.[5] Pain management can be achieved during the reduction with procedural sedation and analgesia or a hematoma block.[5] A year or two may be required for healing to occur.[2]
About 15% of people have a Colles' fracture at some point in time.[3] They occur more commonly in young adults and older people than in children and middle-aged adults.[3] Women are more frequently affected than men.[3] The fracture is named after Abraham Colles who described it in 1814.[3]
Causes
The fracture is most commonly caused by people falling onto a hard surface and breaking their fall with outstretched hand (FOOSH)–falling with wrists flexed would lead to a Smith's fracture. Originally it was described in elderly and/or post-menopausal women. It usually occurs about three to five centimetres proximal to the radio-carpal joint with posterior and lateral displacement of the distal fragment resulting in the characteristic "dinner fork" or "bayonet" like deformity. Colles fracture is a common fracture in people with osteoporosis, second only to vertebral fractures.
Diagnosis
Diagnosis can be made upon interpretation of anteroposterior and lateral views alone.[6]
The classic Colles fracture has the following characteristics:[7]
- Transverse fracture of the radius
- 2.5 cm (0.98 inches) proximal to the radio-carpal joint
- dorsal displacement and dorsal angulation, together with radial tilt[8]
- Radial shortening
- Loss of ulnar inclination≤
- Radial angulation of the wrist
- Comminution at the fracture site
- Associated fracture of the ulnar styloid process in more than 60% of cases.
Classification
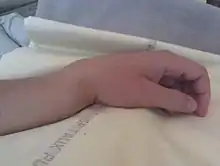
The term Colles fracture is classically used to describe a fracture at the distal end of the radius, at its cortico-cancellous junction. However, the term now tends to be used loosely to describe any fracture of the distal radius, with or without involvement of the ulna, that has dorsal displacement of the fracture fragments. Colles himself described it as a fracture that “takes place at about an inch and a half (38mm) above the carpal extremity of the radius” and “the carpus and the base of metacarpus appears to be thrown backward”.[10] The fracture is sometimes referred to as a "dinner fork" or "bayonet" deformity due to the shape of the resultant forearm.
Colles' fractures can be categorized according to several systems including Frykman, Gartland & Werley, Lidström, Nissen-Lie and the Older's classifications.
Treatment
Management depends on the severity of the fracture. An undisplaced fracture may be treated with a cast alone. The cast is applied with the distal fragment in palmar flexion and ulnar deviation. A fracture with mild angulation and displacement may require closed reduction. There is some evidence that immobilization with the wrist in dorsiflexion as opposed to palmarflexion results in less redisplacement and better functional status.[11] Significant angulation and deformity may require an open reduction and internal fixation or external fixation. The volar forearm splint is best for temporary immobilization of forearm, wrist and hand fractures, including Colles fracture. There are several established instability criteria: dorsal tilt >20°, comminuted fracture, abruption of the ulnar styloid process, intraarticular displacement >1mm, loss of radial height >2mm.
A higher amount of instability criteria increases the likelihood of operative treatment.
Treatment modalities differ in the elderly.[12]
Repeat Xrays are recommended at one, two, and six weeks to verify proper healing.[4]
Prognosis
Recovery time depends on the degree of bone displacement, the number of bone fragments, whether or not the break is "intra-articular" (involves the wrist joint), as well as the person's age, gender, and medical history, and may range from two months to a year or more for complete recovery.[2]
Epidemiology
Colles fractures occur in all age groups, although certain patterns follow an age distribution.
- In the elderly, because of the weaker cortex, the fracture is more often extra-articular.
- Younger individuals tend to require a higher energy force to cause the fracture and tend to have more complex intra-articular fractures. In children with open epiphyses, an equivalent fracture is the "epiphyseal slip", as can be seen in other joints, such as a slipped capital femoral epiphysis in the hip. This is a Salter I or II fracture with the deforming forces directed through the weaker epiphyseal plate.
- More common in women because of post-menopausal osteoporosis.
History
The Colles fracture is named after Abraham Colles (1773–1843), an Irish surgeon, from Kilkenny who first described it in 1814 by simply looking at the classical deformity before the advent of X-rays.[13] Ernest Amory Codman was the first to study it using X-rays. His article, published in the Boston Medical and Surgical Journal, now known as The New England Journal of Medicine, also developed the classification system.[14][15]
See also
References
- "Distal forearm 23-A2.2 CRIF". www2.aofoundation.org. Archived from the original on 13 October 2017. Retrieved 13 October 2017.
- "Distal Radius Fractures (Broken Wrist)". orthoinfo.aaos.org. March 2013. Archived from the original on 2 July 2017. Retrieved 12 October 2017.
- Blakeney, WG (18 November 2010). "Stabilization and treatment of Colles' fractures in elderly patients". Clinical Interventions in Aging. 5: 337–44. doi:10.2147/CIA.S10042. PMC 3010169. PMID 21228899.
- Pfenninger, John L.; Fowler, Grant C. (2010). Pfenninger and Fowler's Procedures for Primary Care E-Book: Expert Consult. Elsevier Health Sciences. p. 1292. ISBN 978-1455700929. Archived from the original on 2017-10-13.
- Oussedik, S; Haddad, F (September 2005). "Manipulation and immobilization of Colles' fractures". British Journal of Hospital Medicine. 66 (9): M34-5. doi:10.12968/hmed.2005.66.Sup2.19718. PMID 16200794.
- Adam, Greenspan (2015). Orthopedic imaging : a practical approach. Beltran, Javier (Professor of radiology) (Sixth ed.). Philadelphia. ISBN 978-1451191301. OCLC 876669045.
- GP Notebook. "Colles' fracture". Archived from the original on 2011-06-13. Retrieved 2009-02-21.
- Solomon et al., Apley's system of orthopaedics and fractures, 9th ed., p.772
- Essentials of musculoskeletal care. Sarwark, John F. Rosemont, Ill.: American Academy of Orthopaedic Surgeons. 2010. ISBN 9780892035793. OCLC 706805938.CS1 maint: others (link)
- Colles A 2006 On the fracture of the carpal extremity of the radius. Edinb Med Surg J. 1814;10:181. Clin Orthop Relat Res 445:5-7.
- "Adult Distal Radius Frx: Non Operative Treatment - Wheeless' Textbook of Orthopaedics". Archived from the original on 2011-04-23.
- Blakeney, William (November 2010). "Stabilization and treatment of Colles' fractures in elderly patients". Clinical Interventions in Aging. 5: 337–44. doi:10.2147/CIA.S10042. PMC 3010169. PMID 21228899.
- synd/2152 at Who Named It?
- Mallon, Bill (2000). Ernest Amory Codman : the end result of a life in medicine. Philadelphia: Saunders. ISBN 978-0-7216-8461-1.
- CODMAN, E. A. (1900). "A Study of the X-Ray Plates of One Hundred and Forty Cases of Fracture of the Lower End of the Radius". The Boston Medical and Surgical Journal. 143 (13): 305–308. doi:10.1056/NEJM190009271431301. ISSN 0096-6762. S2CID 57812302.