Endometrial hyperplasia
Endometrial hyperplasia is a condition of excessive proliferation of the cells of the endometrium, or inner lining of the uterus.
| Endometrial hyperplasia | |
|---|---|
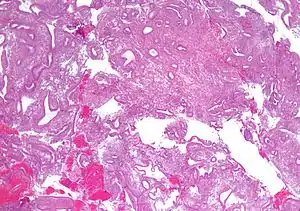 | |
| Micrograph showing simple endometrial hyperplasia, where the gland-to-stroma ratio is preserved but the glands have an irregular shape and/or are dilated. Endometrial biopsy. H&E stain. | |
| Specialty | Gynaecology |
Most cases of endometrial hyperplasia result from high levels of estrogens, combined with insufficient levels of the progesterone-like hormones which ordinarily counteract estrogen's proliferative effects on this tissue. This may occur in a number of settings, including obesity, polycystic ovary syndrome, estrogen producing tumours (e.g. granulosa cell tumour) and certain formulations of estrogen replacement therapy. Endometrial hyperplasia is a significant risk factor for the development or even co-existence of endometrial cancer, so careful monitoring and treatment of women with this disorder is essential.
Classification
Like other hyperplastic disorders, endometrial hyperplasia initially represents a physiological response of endometrial tissue to the growth-promoting actions of estrogen. However, the gland-forming cells of a hyperplastic endometrium may also undergo changes over time which predispose them to cancerous transformation. Several histopathology subtypes of endometrial hyperplasia are recognisable to the pathologist, with different therapeutic and prognostic implications.[3] The most commonly used classification system for endometrial hyperplasia is the World Health Organization system, which has four categories: simple hyperplasia without atypia, complex hyperplasia without atypia, simple atypical hyperplasia and complex atypical hyperplasia.[4]
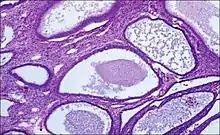
- Endometrial hyperplasia (simple or complex) - Irregularity and cystic expansion of glands (simple) or crowding and budding of glands (complex) without worrisome changes in the appearance of individual gland cells. In one study, 1.6% of patients diagnosed with these abnormalities eventually developed endometrial cancer.[5]
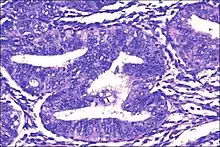
- Atypical endometrial hyperplasia (simple or complex) - Simple or complex architectural changes, with worrisome (atypical) changes in gland cells, including cell stratification, tufting, loss of nuclear polarity, enlarged nuclei, and an increase in mitotic activity. These changes are similar to those seen in true cancer cells, but atypical hyperplasia does not show invasion into the connective tissues, the defining characteristic of cancer. The previously mentioned study found that 22% of patients with atypical hyperplasia eventually developed cancer.[5]
Diagnosis
Diagnosis of endometrial hyperplasia can be made by endometrial biopsy, which is done in the office setting or through curettage of the uterine cavity to obtain endometrial tissue for histopathologic analysis. A workup for endometrial disease may be prompted by abnormal uterine bleeding, or the presence of atypical glandular cells on a pap smear.[6]
Treatment
Treatment of endometrial hyperplasia is individualized, and may include hormonal therapy, such as cyclic or continuous progestin therapy, or hysterectomy.[6]
References
- Rao, Shalinee; Sundaram, Sandhya; Narasimhan, Raghavan (2009). "Biological behavior of preneoplastic conditions of the endometrium: A retrospective 16-year study in south India". Indian Journal of Medical and Paediatric Oncology. 30 (4): 131–135. doi:10.4103/0971-5851.65335. ISSN 0971-5851. PMC 2930300. PMID 20838554.
- Figure- available via license: Creative Commons Attribution 2.0 Generic - Rao, Shalinee; Sundaram, Sandhya; Narasimhan, Raghavan (2009). "Biological behavior of preneoplastic conditions of the endometrium: A retrospective 16-year study in south India". Indian Journal of Medical and Paediatric Oncology. 30 (4): 131–135. doi:10.4103/0971-5851.65335. ISSN 0971-5851. PMC 2930300. PMID 20838554.
- Figure- available via license: Creative Commons Attribution 2.0 Generic - Cote, Richard; Suster, Saul; Weiss, Lawrence; et al., eds. (2002). Modern Surgical Pathology (2 Volume Set). London: W B Saunders. ISBN 0-7216-7253-1.
- Skov, B. G.; Broholm, H; Engel, U; Franzmann, M. B.; Nielsen, A. L.; Lauritzen, A. F.; Skov, T (1997). "Comparison of the reproducibility of the WHO classifications of 1975 and 1994 of endometrial hyperplasia". International Journal of Gynecological Pathology. 16 (1): 33–7. doi:10.1097/00004347-199701000-00006. PMID 8986530. S2CID 26446736.
- Kurman, Robert J.; Kaminski, Paul F.; Norris, Henry J. (1985). "The behavior of endometrial hyperplasia. A long-term study of "untreated" hyperplasia in 170 patients". Cancer. 56 (2): 403–12. doi:10.1002/1097-0142(19850715)56:2<403::AID-CNCR2820560233>3.0.CO;2-X. PMID 4005805.
- Howard A Zacur; Robert L Giuntoli, II; Marcus Jurema. "Endometrial Hyperplasia". UpToDate Online. Retrieved 2007-05-26.
External links
| Classification | |
|---|---|
| External resources |