Epidemiology data for low-linear energy transfer radiation
Epidemiological studies of the health effects of low levels of ionizing radiation, in particular the incidence and mortality from various forms of cancer, have been carried out in different population groups exposed to such radiation. These have included survivors of the atomic bombings of Hiroshima and Nagasaki in 1945, workers at nuclear reactors, and medical patients treated with X-rays.
Life span studies of atomic bomb survivors
Survivors of the atomic bomb explosions at Hiroshima and Nagasaki, Japan have been the subjects of a Life Span Study (LSS), which has provided valuable epidemiological data.
The LSS population went through several changes:
- 1945 - There were some 93,000 individuals, either living in Hiroshima or Nagasaki, Japan.
- 1950 - An additional 37,000 were registered by this time, for a total of 130,000 LSS members.
However, some 44,000 individuals were censured or excluded from the LSS project, so there remained about 86,000 people who were followed through the study. There is a gap in knowledge of the earliest cancer that developed in the first few years after the war, which impacts the assessment of leukemia to an important extent and for solid cancers to a minor extent. Table 1 shows summary statistics of the number of persons and deaths for different dose groups. These comparisons show that the doses that were received by the LSS population overlap strongly with the doses that are of concern to NASA Exploration mission (i.e., 50 to 2,000 milliSieverts (mSv)).
| DS86 Weighted Colon Dose, mSv | ||||||||
|---|---|---|---|---|---|---|---|---|
| Total | 0-50 | 50-100 | 100-200 | 200-500 | 500-1,000 | 1,000-2,000 | >2,000 | |
| No. Subjects | 86,572 | 37,458 | 31,650 | 5,732 | 6,332 | 3,299 | 1,613 | 488 |
| Cancer Deaths | 9,335 | 3,833 | 3,277 | 668 | 763 | 438 | 274 | 82 |
| Non-cancer Deaths | 31,881 | 13,832 | 11,633 | 2,163 | 2,423 | 1,161 | 506 | 163 |
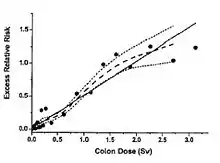
Figure 1 shows the dose response for the excess relative risk (ERR) for all solid cancers from Preston et al.[1] Tables 2 and 3 show several summary parameters for tissue-specific cancer mortality risks for females and males, respectively, including estimates of ERR, excess absolute risk (EAR), and percentage attributable risks. Cancer incidence risks from low-LET radiation are about 60% higher than cancer mortality risks.[3]
| Site/System | Deaths (>0.005Sv) |
ERR/Sva (90% CI) |
EAR/104PYb -Svc (90%CI) |
Attributable risk (%)d |
|---|---|---|---|---|
| All solid cancer | 4,884 (2,948) | 0.63 (0.49; 0.79) | 13.5 (7.4; 16.3) | 9.2 (7.4; 11.0) |
| Oral cavity | 42 (25) | -0.20 (<-0.3; 0.75) | -0.04 (<-0.3; 0.14) | -4.1 (<-6; 14) |
| Digestive System | ||||
| Esophagus | 67 (44) | 1.7 (0.46; 3.8) | 0.51 (0.15; 0.92) | 22 (6.6; 42) |
| Stomach | 1,312 (786) | 0.65 (0.40; 0.95) | 3.3 (2.1; 4.7) | 8.8 (5.5; 12) |
| Colon | 272 (786) | 0.49 (0.11; 1.1) | 0.68 (0.76; 1.3) | 9.0 (4.3; 17) |
| Rectum | 198 (127) | 0.75 (0.16; 1.6) | 0.69 (0.16; 1.3) | 11.3 (2.6; 22) |
| Liver | 514 (291) | 0.35 (0.07; 0.72) | 0.85 (0.18; 1.6) | 6.2 (1.3; 12) |
| Gallbladder | 236 (149) | 0.16 (-0.17; 0.67) | 0.18 (-0.21; 0.71) | 2.6 (-2.9; 10) |
| Pancreas | 244 (135) | -0.01 (-0.28; 0.45) | -0.01 (-0.35; 0.52) | -0.2 (-5.0; 7.6) |
| Respiratory System | ||||
| Lung | 548 (348) | 1.1 (0.678; 1.6) | 2.5 (1.6; 3.5) | 16 (10; 22) |
| Female breast | 272; (173) | 0.79 (0.29; 1.5) | 1.6 (1.2; 2.2) | 24 (18; 32) |
| Uterus | 518 (323) | 0.17 (-0.10; 0.52) | 0.44 (-0.27; 1.3) | 2.7 (-1.6; 7.9) |
| Ovary | 136 (85) | 0.94 (0.07; 2.0) | 0.63 (0.23; 1.2) | 15 (5.3; 28) |
| Urinary System | ||||
| Bladder | 67 (43) | 1.2 (0.10; 3.1) | 0.33 (0.02; 0.74) | 16 (0.9; 36) |
| Kidney | 31 (21) | 0.97 (<-0.3; 3.8) | 0.14 (<-0.1; 0.42) | 14 (<-3; 42) |
| Brain/CNSd | 17 (10) | 0.51 (<-0.3; 3.9) | 0.04 (<-0.02; 0.2) | 11 (<0.05; 57) |
| aERR/SV for age at exposure 30 in an age-constant linear ERR model; bExcess absolute risk per 10,000 persons per year; cAverage EAR computed from ERR model; dAttributable risk among survivors whose estimated dose is at least 0.005 Sv; CNS - central nervous system. | ||||
| Site/System | Deaths (>0.005Sv) |
ERR/Sva (90% CI) |
EAR/104PYb -Svc (90%CI) |
Attributable risk (%)d |
|---|---|---|---|---|
| All solid cancer | 4,451 (2,554) | 0.37 (0.26; 0.49) | .6 (9.4; 16.2) | 6.6 (4.9; 8.4) |
| Oral cavity | 68 (37) | -0.20 (<-0.3; 0.45) | -0.12 (<-0.3; 0.25) | -5.2 (<-6; 11) |
| Digestive System | ||||
| Esophagus | 224 (130) | 0.61 (0.15; 1.2) | 1.1 (0.28; 2.0) | 11.1 (2.8; 21) |
| Stomach | 1,555 (899) | 0.20 (0.04; 0.39) | 2.1 (0.43; 4.0) | 3.2 (0.07; 6.2) |
| Colon | 206 (122) | 0.54 (0.13; 1.2) | 1.1 (0.64; 1.9) | 12 (6.9; 21) |
| Rectum | 172 (96) | -0.25 (<-0.3; 0.15) | -0.41 (<-0.4; 0.22) | -5.4 (<-6; 3.1) |
| Liver | 722 (408) | 0.59 (0.11; 0.68) | 2.4 (1.2; 4.0) | 8.4 (4.2; 14) |
| Gallbladder | 92 (52) | 0.89 (0.22; 1.9) | 0.63 (0.17; 1.2) | 17 (4.5; 33) |
| Pancreas | 163 (103) | -0.11 (<-0.3; 0.44) | -0.15 (<-0.4; 0.58) | --1.9 (<-6; 7.5) |
| Respiratory System | ||||
| Lung | 716 (406) | 0.48 (0.23; 0.78) | 2.7 (1.4; 4.1) | 9.7 (4.9; 15) |
| Urinary System | ||||
| Bladder | 82 (56) | 1.1 (0.2; 2.5) | 0.7 (0.1; 1.4) | 17 (3.3; 34) |
| Kidney | 36 (18) | -0.02 (<-0.3; 1.1) | -0.01 (-0.1; 0.28) | -0.4 (<-5; 22) |
| Brain/CNSd | 14 (9) | 5.3 (1.4; 16) | 0.35 (0.13; 0.59) | 62 (23; 100) |
| aERR/SV for age at exposure 30 in an age-constant linear ERR model; bExcess absolute risk per 10,000 persons per year; cAverage EAR computed from ERR model; dAttributable risk among survivors whose estimated dose is at least 0.005 Sv; CNS - central nervous system. | ||||
Other human studies
The BEIR VII Report[2] contains an extensive review of data sets from human populations, including nuclear reactor workers and patients who were treated with radiation. The recent report from Cardis et al.[4] describes a meta-analysis for reactor workers from several countries. A meta-analysis at specific cancer sites, including breast, lung, and leukemia, has also been performed.[2] These studies require adjustments for photon energy, dose-rate, and country of origin as well as adjustments made in single population studies. Table 4 shows the results that are derived from Preston et al.[5] for a meta-analysis of breast cancer risks in eight populations, including the atomic-bomb survivors. The median ERR varies by slightly more than a factor of two, but confidence levels significantly overlap. Adjustments for photon energy or dose-rate and fractionation have not been made. These types of analysis lend confidence to risk assessments as well as showing the limitations of such data sets.
Of special interest to NASA is the dependence on age at exposure of low-LET cancer risk projections. The BEIR VII report prefers models that show less than a 25% reduction in risk over the range from 35 to 55 years, while NCRP Report No. 132[6] shows about a two-fold reduction over this range.
| Cohort | Reference age for the ERR/Gy estimate |
ERR/Gya | Percentage change per decade increase in age at exposure |
Exponent of attained age |
Background SIRb |
|---|---|---|---|---|---|
| LSS | attained age 50 | 2.10 (1.6; 2.8) |
Not includedb | -2.0 (-2.8; -1.1) |
1.01 (0.9; 1.1) |
| TBO | attained age 50 | 0.74 (0.4; 1.2) |
Not included | -2.0 (-2.8; -1.1) |
0.96 (0.7; 1.2) |
| TBX | attained age 50 | 0.74 (0.4; 1.2) |
Not included | -2.0 (-2.8; -1.1) |
0.73 (0.6; 0.9) |
| THY | attained age 50 | 0.74 (0.4; 1.2) |
Not included | -2.0 (-2.8; -1.1) |
1.05 (0.7; 1.5) |
| BBD | age at exposure 25 | 1.9 (1.3; 2.8) |
-60% (-71%; -44%) |
Not includedc | 0.98 (0.8; 1.2) |
| APM | all ages | 0.56 (0.3; 0.9) |
Not included | Not included | 1.45 (1.1; 1.8) |
| HMG | all ages | 0.34 (0.1; 0.7) |
Not included | Not included | 1.07 (0.8; 1.3) |
| HMS | all ages | 0.34 (0.1; 0.7) |
Not included | Not included | 1.05 (0.9; 1.2) |
| a C.I.'s within parentheses; bSIR = standardized incidence ratio; c"Not included" means that the risk is assumed not to vary with age at exposure (attained age). | |||||
See also
References
- Preston, DL; Shimizu, Y; Pierce, DA; Suyama, A; Mabuchi, K (October 2003). "Studies of mortality of atomic bomb survivors. Report 13: Solid cancer and noncancer disease mortality: 1950-1997" (PDF). Radiation Research. 160 (4): 381–407. Bibcode:2003RadR..160..381P. doi:10.1667/RR3049. PMID 12968934. S2CID 41215245. Archived from the original (PDF) on 28 October 2011. Retrieved 5 July 2012.
- Committee to Assess Health Risks from Exposure to Low Levels of Ionizing Radiation; National Research Council of the National Academies (2006). Health risks from exposure to low levels of ionizing radiation BEIR VII, Phase 2 ([Online-Ausg.] ed.). Washington, D.C.: National Academies Press. ISBN 978-0-309-53040-8. Retrieved 1 October 2013.
- Preston, DL; Ron, E; Tokuoka, S; Funamoto, S; Nishi, N; Soda, M; Mabuchi, K; Kodama, K (July 2007). "Solid cancer incidence in atomic bomb survivors: 1958-1998". Radiation Research. 168 (1): 1–64. Bibcode:2007RadR..168....1P. doi:10.1667/RR0763.1. PMID 17722996. S2CID 7398164.
- Cardis, E; Vrijheid, M; Blettner, M; Gilbert, E; Hakama, M; Hill, C; Howe, G; Kaldor, J; Muirhead, CR; Schubauer-Berigan, M; Yoshimura, T; Bermann, F; Cowper, G; Fix, J; Hacker, C; Heinmiller, B; Marshall, M; Thierry-Chef, I; Utterback, D; Ahn, YO; Amoros, E; Ashmore, P; Auvinen, A; Bae, JM; Bernar, J; Biau, A; Combalot, E; Deboodt, P; Diez Sacristan, A; Eklöf, M; Engels, H; Engholm, G; Gulis, G; Habib, RR; Holan, K; Hyvonen, H; Kerekes, A; Kurtinaitis, J; Malker, H; Martuzzi, M; Mastauskas, A; Monnet, A; Moser, M; Pearce, MS; Richardson, DB; Rodriguez-Artalejo, F; Rogel, A; Tardy, H; Telle-Lamberton, M; Turai, I; Usel, M; Veress, K (April 2007). "The 15-Country Collaborative Study of Cancer Risk among Radiation Workers in the Nuclear Industry: estimates of radiation-related cancer risks". Radiation Research. 167 (4): 396–416. Bibcode:2007RadR..167..396C. doi:10.1667/RR0553.1. PMID 17388693. S2CID 36282894.
- Preston, DL; Mattsson, A; Holmberg, E; Shore, R; Hildreth, NG; Boice JD, Jr (August 2002). "Radiation effects on breast cancer risk: a pooled analysis of eight cohorts". Radiation Research. 158 (2): 220–35. Bibcode:2002RadR..158..220P. doi:10.1667/0033-7587(2002)158[0220:reobcr]2.0.co;2. JSTOR 3580776. PMID 12105993.
- NCRP (2000). NPRC Report No. 132: Recommendations of dose limits for low Earth orbit. Bethesda, MD: NCRP. Archived from the original on 4 October 2013. Retrieved 5 July 2012.
![]() This article incorporates public domain material from the National Aeronautics and Space Administration document: "Human Health and Performance Risks of Space Exploration Missions" (PDF). (NASA SP-2009-3405, pp. 132-134)
This article incorporates public domain material from the National Aeronautics and Space Administration document: "Human Health and Performance Risks of Space Exploration Missions" (PDF). (NASA SP-2009-3405, pp. 132-134)