Glomus tumor
A glomus tumor (also known as a "solitary glomus tumor,"[1] "solid glomus tumor,"[1]) is a rare neoplasm arising from the glomus body and mainly found under the nail, on the fingertip or in the foot.[2]:670 They account for less than 2% of all soft tissue tumors.[3] The majority of glomus tumors are benign, but they can also show malignant features.[4] Glomus tumors were first described by Hoyer in 1877 while the first complete clinical description was given by Masson in 1924.[5]
| Glomus tumor | |
|---|---|
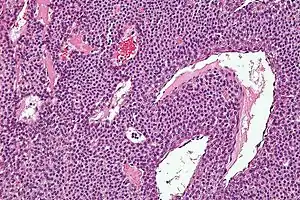 | |
| Micrograph of a glomus tumor. H&E stain. | |
| Specialty | Oncology |
- Glomus tumor was also the name formerly (and incorrectly) used for a tumor now called a paraganglioma.
Histologically, glomus tumors are made up of an afferent arteriole, anastomotic vessel, and collecting venule. Glomus tumors are modified smooth muscle cells that control the thermoregulatory function of dermal glomus bodies. As stated above, these lesions should not be confused with paragangliomas, which were formerly also called glomus tumors in now-antiquated clinical usage. Glomus tumors do not arise from glomus cells, but paragangliomas do.
Familial glomangiomas have been associated with a variety of deletions in the GLMN (glomulin) gene, and are inherited in an autosomal dominant manner, with incomplete penetrance.[5]
Signs and symptoms
Glomus tumors are usually solitary and small lesions. The vast majority are found in the hand, wrist, foot, and under the fingernails.[3]
They are often painful, and the pain is reproduced when the lesion is placed in cold water. Multiple tumors are less likely to be painful.
These tumors tend to have a bluish discoloration, although a whitish appearance may also be noted. Elevation of the nail bed can occur.
In rare cases, the tumors may present in other body areas, such as the gastric antrum or glans penis. Treatment is essentially the same.[6]
Malignant glomus tumors, or glomangiosarcomas, are extremely rare and usually represent a locally infiltrative malignancy. However, metastases do occur and are usually fatal.
Diagnosis
Cancerous glomus tumors are exceedingly rare. Criteria for the diagnosis of malignancy in glomus tumors are:[7]
- Tumor size of more than 2 centimeters and subfascial or visceral location.
- Atypical mitotic figures.
- Marked nuclear atypia and any level of mitotic activity.
- Pericytes of Zimmerman
Cancerous glomus tumors have been subdivided into three categories based on their histologic appearance: locally infiltrative glomus tumors (LIGT), glomangiosarcomas arising in benign glomus tumors (GABG), and glomangiosarcomas arising de novo (GADN).[8]
A few cases of cancerous glomus tumors have been reported; however, they are usually only locally invasive, and metastases are exceedingly rare. There is one report of widespread metastases of a malignant glomus tumor involving the skin, lungs, jejunum, liver, spleen, and lymph nodes.[9] Another report of a malignant glomus tumor (glomangiosarcoma) with metastases from the skin.[10] A malignant glomus tumor one arose from the kidneys.[8]
Differential
The probable misdiagnosis of many of these lesions as hemangiomas or venous malformations also makes an accurate assessment of incidence difficult.
Treatment

Surgical excision is the preferred treatment for benign glomus tumors.[11]
Epidemiology
The exact rate of glomus tumors is unknown. The multiple variant is rare, accounting for less than 10% of all cases.
Sex
Solitary glomus tumors, particularly subungual lesions, are more common in females than in males. Multiple lesions are slightly more common in males.
Age
Solitary glomus tumors are more frequent in adults than in others. Multiple glomus tumors develop 11–15 years earlier than single lesions; about one third of the cases of multiple tumors occur in those younger than 20 years. Congenital glomus tumors are rare; they are plaguelike in appearance and are considered a variant of multiple glomus tumors.
See also
- Coccygeal glomus
- List of cutaneous conditions
- Myopericytoma
References
- Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. (2007). Dermatology: 2-Volume Set. St. Louis: Mosby. ISBN 1-4160-2999-0.
- Freedberg, et al. (2003). Fitzpatrick's Dermatology in General Medicine. (6th ed.). McGraw-Hill. ISBN 0-07-138076-0.
- International Agency for Research on Cancer (2002). Pathology and Genetics of Tumours of Soft Tissue and Bone. St. Louis: WHO Press. pp. 136–137. ISBN 9789283224136.
- De Chiara, Annarosaria; Apice, Gaetano; Mori, Stefano; Silvestro, Giustino; Losito, Simona N.; Botti, Gerardo; Ninfo, Vito (2003). "Malignant Glomus Tumour: A Case Report and Review of the Literature". Sarcoma. 7 (2): 87–91. doi:10.1080/1357714031000081207. PMC 2395518. PMID 18521375.
- Gombos, Z; Zhang, PJ (September 2008). "Glomus tumor". Archives of Pathology & Laboratory Medicine. 132 (9): 1448–52. doi:10.1043/1543-2165(2008)132[1448:GT]2.0.CO;2. PMID 18788860.
- Macaluso JN, Jr; Sullivan, JW; Tomberlin, S (April 1985). "Glomus tumor of glans penis". Urology. 25 (4): 409–10. doi:10.1016/0090-4295(85)90503-5. PMID 2984824.
- Folpe, AL; Fanburg-Smith, JC; Miettinen, M; Weiss, SW (January 2001). "Atypical and malignant glomus tumors: analysis of 52 cases, with a proposal for the reclassification of glomus tumors". The American Journal of Surgical Pathology. 25 (1): 1–12. doi:10.1097/00000478-200101000-00001. PMID 11145243.
- Lamba, G; Rafiyath, SM; Kaur, H; Khan, S; Singh, P; Hamilton, AM; Ang, DC (August 2011). "Malignant glomus tumor of kidney: the first reported case and review of literature". Human Pathology. 42 (8): 1200–3. doi:10.1016/j.humpath.2010.11.009. PMID 21333326.
- Brathwaite, CD; Poppiti RJ, Jr (February 1996). "Malignant glomus tumor. A case report of widespread metastases in a patient with multiple glomus body hamartomas". The American Journal of Surgical Pathology. 20 (2): 233–8. doi:10.1097/00000478-199602000-00012. PMID 8554113.
- Watanabe, K; Hoshi, N; Tsu-Ura, Y; Suzuki, T (June 1995). "A case of glomangiosarcoma". Fukushima journal of medical science. 41 (1): 71–7. PMID 8606044.
- Kaylie DM, O'Malley M, Aulino JM, Jackson CG (2007). "Neurotologic surgery for glomus tumors". Otolaryngol. Clin. North Am. 40 (3): 625–649. doi:10.1016/j.otc.2007.03.009. PMID 17544699.