Health in Eswatini
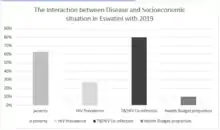
The Health in Eswatini is poor and four years into the United Nations sustainable development goals, Eswatini seems unlikely to achieve goal on health. As a result of 63% poverty prevalence, 27% HIV prevalence, and poor health systems, maternal mortality rate is a high 389/100,000 live births,[1] and under 5 mortality rate is 70.4/1000 live births[2] resulting in a life expectancy that remains amongst the lowest in the world.[3] Despite significant international aid, the government fails to adequately fund the health sector. Nurses are now and again engaged in demonstrations over poor working conditions, drug stock outs, all of which impairs quality health delivery. Despite tuberculosis and AIDS being major causes of death, diabetes and other non-communicable diseases are on the rise.[4] Primary health care is relatively free in Eswatini save for its poor quality to meet the needs of the people. Road traffic accidents[5] have increased over the years and they form a significant share of deaths in the country.[6]
Furthermore, tuberculosis remains a significant problem. The shift has been towards multi-drug resistant strains. TB has an 18 percent mortality rate and 83 percent of cases are co-infected with HIV.[7] There are roughly 14,000 new TB cases diagnosed each year.[8]
Mental illness
The global shift towards more non-communicable diseases does not spare Eswatini. However scanty research is on mental illness in the country, increasing levels of poverty, sexual violence, HIV/AIDS, alcohol and cannabis abuse[9] are highly associated with mental health issues. Lack of policy, poor facilities, and limited personnel[10] all contribute to poor awareness and is a concern that shall soon explode as a crisis in the population and burden of disease in the country.
Eswatini does not have an expansive mental health infrastructure. Most healthcare is centralized in cities where only approximately 20% of the population lives. Though recently there may have been additions, in 2011 there was one psychiatrist in National Psychiatric Referral Hospital and in the country.[11] Impractical as it may, they attended inpatients, prisoners, children, and outpatients.[12]
Given Eswatini's overall health situation, many health-oriented non-governmental organizations, university programs, and other organizations work in the country on research and service projects related to health, mental health remain on the periphery. Despite all these negatives, there is but one organization working on awareness and promotion of mental health in the country.[13]
HIV/AIDS
Eswatini has made significant strides in fighting HIV/AIDS. From being highest in prevalence and incidence in late 2000s, it has shifted to be a model for HIV control in the world. Urgency, programmatic shifts and international aid make the frontline in the combat against the epidemic. The first case of HIV in Eswatini was reported in 1986, approximately 26 years after the first known case in the world. Fast forward about two decades later, it was reported the biggest killer; at 64% of all deaths in the country. In 2003, the Eswatini government (then Swaziland) declared HIV/AIDS a national crisis, with 38.8% of tested pregnant women infected with HIV (see AIDS in Africa). Prime Minister Themba Dlamini declared a humanitarian crisis due to the combined effect of drought, land degradation, increased poverty, and HIV/AIDS. NERCHA[16] was formed in 2003 to coordinate action against the disease. HIV care guidelines were published in 2010, revised in 2015 and most recently in 2018 to improve models of care, and fit emerging developments in the fight against HIV/AIDS. A 2016 SHIMS 2[17] found a significant decrease in prevalence of HIV compared to 2012 in SHIMS 1.[18] Eswatini scores lowest incidence and related deaths today in the region.[19] Universal ART coverage and extensive outreach targeted at hard to reach populations for HTC are responsible for the country’s success towards the 90/90/90 2020 UNAIDS goal of ending HIV.
Public expenditure for HIV/AIDS was 4% of the GDP of the country, whereas private expenditure was 2.3%.[20] Infant mortality was 57.19 per 1,000 in 2014,[21] 47% of all deaths under 5 were caused by HIV/AIDS.[22]
Healthcare
There were 16 physicians per 100,000 persons in the early 2000s.[20]
In September 2018 as the government had not paid suppliers the health service ran out of food and medicine. Swazipharm could not buy drugs. in May 2017 US$18 million was said to be owed to drug companies. There were only 12 working public ambulances in the country in June 2018.[23]
Hospitals

There were in 2019 135 medical facilities in Eswanti, including four hospitals run by the Ministry of Health and two hospitals run by NGO missions. The other medical facilities are clinics and health centers.[24]
| Name | Location | Type facility | Ref |
|---|---|---|---|
| Mbabane Government Hospital | Hhohho Region | Referral Hospital | [24] |
| Pigg's Peak Government Hospital | Hhohho Region | Regional Hospital | [24] |
| Good Shepherd Hospital | Lubombo Region | Mission Hospital | [24] |
| Mankayane Hospital | Manzini Region | Regional Hospital | [24] |
| Raleigh Fitkin Memorial (RFM) Hospital | Manzini Region | Mission Hospital | [24] |
| Hlatikhulu Hospital | Shiselweni Region | Regional Hospital | [24] |
References
- "Maternal Mortality Rate". Index Mundi. Retrieved 18 October 2019.
- "Indicators in Eswanti". Index Mundi. Retrieved 18 October 2019.
- "Life Expectancy in Swaziland". World Population Review. Retrieved 15 September 2019.
- "Blobal Health Data Comparison". Vizhub. Retrieved 15 September 2019.
- "Swaziland Road Traffic Accidents". World Life Expectancy. Retrieved 15 September 2019.
- CIA Factbook, Eswatini. Central Intelligence Agency.
- "Swaziland: An MSF Doctors Explains HIV-TB Co-Infection". USA: Doctors Without Borders/Médecins Sans Frontières. 28 October 2009. Archived from the original on 25 July 2011. Retrieved 31 October 2009.
- "HIV-TB in Swaziland: A Deadly Co-Infection Epidemic". USA: Doctors Without Borders/Médecins Sans Frontières. 28 October 2009. Archived from the original on 21 June 2010. Retrieved 31 October 2009.
- Mhlongo, Gladys Thembinkosi (November 2005). Drug Abuse by Adolescents in Swaziland. MSc Thesis, University of South Africa. CiteSeerX 10.1.1.543.3720.
- "Profile of Swaziland" (PDF). WHO. Retrieved 17 September 2019.
- "Swaziland Mental Health Profile" (PDF). Retrieved 20 September 2019.
- "HealingthroughArt". healingthroughart.webflow.io. Archived from the original on 25 April 2016. Retrieved 17 April 2016.
- "About Swaziland". Imerse. Retrieved 17 September 2019.
- "Budget Speech 2019" (PDF). Government of Swaziland.
- "Atlas of African Health Statistics". AHO AFRO WHO International.
- "HIV and AIDS in Swaziland". HIV Sharespace. Retrieved 15 September 2019.
- "Final Report" (PDF). PHIA ICAP Columbia. Retrieved 13 September 2019.
- "SHIMS 2nd Report" (PDF). 2014. Retrieved 13 September 2019.
- "Atlas of African Health Statistics". 2019. Retrieved 14 September 2019.
- "Human Development Report 2009 – Swaziland". Hdrstats.undp.org. Archived from the original on 15 July 2010. Retrieved 27 June 2010.
- "The World Factbook". Cia.gov. Retrieved 16 August 2014.
- "Swaziland, Mortality Country Fact Sheet 2006" (PDF). WHO. Archived from the original (PDF) on 5 August 2009.
- "Swaziland: No Food for Hospital Patients As Broke Swaziland Government Leaves Supplier Bills Unpaid". All Africa. 27 September 2018. Retrieved 25 November 2018.
- "A spatial database of health facilities managed by the public health sector in sub-Saharan Africa". World Health Organization. February 11, 2019. Retrieved May 8, 2020.
