Lateral rectus muscle
The lateral rectus muscle is a muscle on the lateral side of the eyeball in the orbit. It is one of six extraocular muscles that control the movements of the eye. The lateral rectus muscle is responsible for lateral movement of the eyeball, specifically abduction. Abduction describes the movement of the eye away from the midline (i.a. nose), allowing the eyeball to move horizontally in the lateral direction, bringing the pupil away from the midline of the body.[1]
| Lateral rectus | |
|---|---|
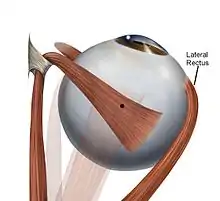 Lateral rectus muscle: is shown in this superior view of the eye. The lateral rectus is on the right side of the image. | |
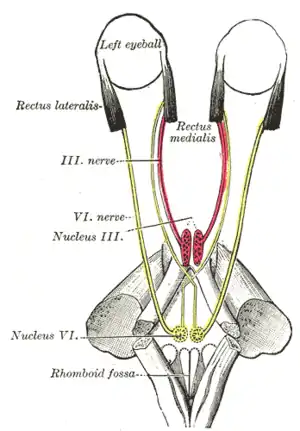 Figure showing the mode of innervation of the Recti medialis and lateralis of the eye. | |
| Details | |
| Origin | annulus of Zinn at the orbital apex |
| Insertion | 7 mm temporal to the limbus |
| Nerve | abducens nerve |
| Actions | abducts the eyeball (makes it move outwards) |
| Identifiers | |
| Latin | musculus rectus lateralis bulbi |
| TA98 | A15.2.07.013 |
| TA2 | 2045 |
| FMA | 49038 |
| Anatomical terms of muscle | |
Structure
The lateral rectus originates at the lateral part of the annulus of Zinn, also known as the annular tendon or common tendinous ring, and inserts into the temporal side of the eyeball. The annulus of Zinn is a tendinous ring that surrounds the optic nerve and serves as the origin for five of the six extraocular muscles, excluding the inferior oblique muscle.[2]
Nerve supply
It is the only muscle supplied by the abducens nerve, cranial nerve VI. The abducens nerve exits the brainstem from the pons-medullary junction, and travels through the superior orbital fissure to innervate the lateral rectus muscle.[1]
The lateral rectus muscle is innervated through the tectospinal tract. This tract begins in the tectum region of the midbrain, and crosses to the contralateral side of the midbrain. The tectospinal tract descends through the brainstem to the upper spinal cord, but goes no further than the neck. This tract is involved with both upper and lower motor neurons, as well as in the reflex of turning the head in response to visual and auditory stimulus. Part of the descending tracts carry motor signals down the brainstem and spinal cord.[3]
Function
It causes outward movement of the eyeball, also called as abduction.
Clinical significance
A sixth nerve palsy, also known as abducens nerve palsy, is a neurological defect that results from a damaged or impaired abducens nerve. This damage can stem from stroke, trauma, tumor, inflammation, and infection. Damage to the abducens nerve by trauma can be caused by any type of trauma that causes elevated intracranial pressure; including hydrocephalus, traumatic brain injury with intracranial bleeding, tumors, and lesions along the nerve at any point between the pons and lateral rectus muscle in orbit. This defect can result in horizontal double vision and reduced lateral movement. The lateral rectus muscle will be denervated and paralyzed and the patient will be unable to abduct the eye. For example, if the left abducens nerve is damaged, the left eye will not abduct fully. While attempting to look straight ahead, the left eye will be deviated medially towards the nose due to the unopposed action of the medial rectus of the eye.[4] Proper function of the lateral rectus is tested clinically by asking the patient to look laterally. Depending on the underlying cause of the lateral rectus palsy, some improvement may occur naturally over time. While the prognosis for a lateral rectus palsy onset by a viral illness is generally positive, the prognosis for an onset of trauma or tumor is quite poor. Ultimately, nerves are not very good at regenerating or healing themselves, so if the damage is severe there will be permanent damage.[5]
In addition, another disorder associated with the lateral rectus muscle is Duane Syndrome. This syndrome occurs when the sixth cranial nerve which controls the lateral rectus muscle does not develop properly. It is believed that Duane Syndrome is a result of a disturbance of normal embryonic development due to a genetic or an environmental factor.[6]
Additional images
 Lateral rectus muscle
Lateral rectus muscle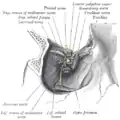 Dissection showing origins of right ocular muscles, and nerves entering by the superior orbital fissure.
Dissection showing origins of right ocular muscles, and nerves entering by the superior orbital fissure.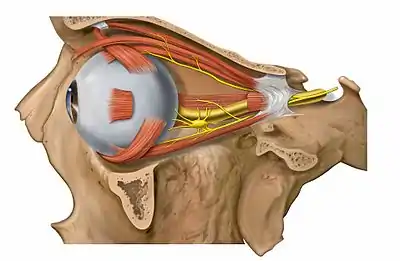 Lateral view of the eyeball with lateral rectus muscle visible (cut).
Lateral view of the eyeball with lateral rectus muscle visible (cut). Lateral rectus muscle
Lateral rectus muscle Extrinsic eye muscle. Nerves of orbita. Deep dissection.
Extrinsic eye muscle. Nerves of orbita. Deep dissection. Extrinsic eye muscle. Nerves of orbita. Deep dissection.
Extrinsic eye muscle. Nerves of orbita. Deep dissection. Extrinsic eye muscle. Nerves of orbita. Deep dissection.
Extrinsic eye muscle. Nerves of orbita. Deep dissection. Extrinsic eye muscle. Nerves of orbita. Deep dissection.
Extrinsic eye muscle. Nerves of orbita. Deep dissection.
References
- Purves, D.; Augustine, G. J.; Fitzpatrick, D., eds. (2001). "The Actions and Innervation of Extraocular Muscles". Neuroscience (2nd ed.). Sunderland: Sinauer Associates.
- "Annulus of Zinn". www.aao.org. Retrieved 2019-09-04.
- Saladin, Kenneth S. (2012). Anatomy Physiology: The Unity of Form and Function. New York: McGraw-Hill. ISBN 978-0-07-337825-1.
- Nguyen, Van; Varacallo, Matthew (2019), "Neuroanatomy, Cranial Nerve 6 (Abducens)", StatPearls, StatPearls Publishing, PMID 28613463, retrieved 2019-09-04
- Azarmina, Mohsen; Azarmina, Hossein (2013). "The Six Syndromes of the Sixth Cranial Nerve". Journal of Ophthalmic and Vision Research. 8 (2): 160–171. PMC 3740468. PMID 23943691.
- "Duane syndrome". NORD (National Organization for Rare Disorders). Retrieved 2019-09-04.
External links
- Anatomy figure: 29:01-05 at Human Anatomy Online, SUNY Downstate Medical Center
- "6-1". Cranial Nerves. Yale School of Medicine. Archived from the original on 2016-03-03.
| Authority control |
|---|