Neuronavigation
Neuronavigation is the set of computer-assisted technologies used by neurosurgeons to guide or "navigate” within the confines of the skull or vertebral column during surgery, and used by psychiatrists to accurately target rTMS (Transcranial Magnetic Stimulation). The set of hardware for these purposes is referred to as a neuronavigator.
| Neuronavigation | |
|---|---|
| MeSH | D038361 |
Stereotactic Surgery
Neuronavigation is recognized as the next evolutionary step of stereotactic surgery, a set of techniques that dates back to the early 1900s and that gained popularity during the 1940s, particularly in Germany, France and the U.S., with the development of surgery for the treatment of movement disorders such as Parkinson's disease and dystonias. In its infancy the purpose of this technology was to create a mathematical model describing a proposed coordinate system for the space within a closed structure, e.g., the skull. This "fiducial spatial coordinate system” uses fiducial markers as a reference to describe with high accuracy the position of specific structures within this arbitrarily defined space. The surgeon then refers to that data to target particular structures within the brain. This technology was boosted by the collection of data on human anatomy in “stereotactic atlases”, expanding the quantitatively defined “targets” that could be readily used in surgery. Finally, the advent of modern neuro-imaging technologies such as computed tomography (CT) and magnetic resonance imaging (MRI)—along with the ever-increasing capabilities of digitalization, computer-graphic modelling and accelerated manipulation of data through complex mathematical algorithms via robust computer technologies—made possible the real-time quantitative spatial fusion of images of the patient's brain with the created “fiducial coordinate system” for the purpose of guiding the surgeon's instrument or probe to a selected target. In this way the observations done via highly sophisticated neuro-imaging technologies (CT, MRI, angiography) are related to the actual patient during surgery.
Neuro Imaging
The ability to relate the position of a real surgical instrument in the surgeon's hand or the microscope's focal point to the location of the imaged pathology, updated in "real time" in an "integrated operating room", highlights the modern version of this set of technologies. In its current form, neuronavigation began in the 1990s and has adapted to new neuro-imaging technologies, real-time imaging capabilities, new technologies to transfer the information in the operating room for 3-D localization, real-time neuro-monitoring, robotics, and new and better algorithms to handle data via more sophisticated computer technology.
Surgical Virtualization
In its later conceptualization, the term neuronavigation has started to overlap fuse with surgical-virtualization in which a neurosurgeon is able to vizualize the scenario for surgery in a 3-D model of manipulable computer data. In this way the physician can "practice and check" the surgery, try alternative approaches, assess possible difficulties, etc., before the real surgery takes place.
Neuronavigation for Transcranial Magnetic Stimulation
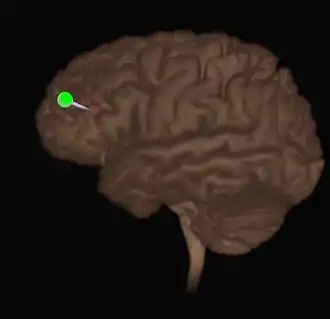
The standard TMS protocol which was FDA approved in 2008 estimates the location of the DLPFC by finding the left motor cortex and marking a spot 5 cm anterior to it. Later two more methods were introduced using measurements of the head and calculating the location of the DLPFC as 1) the F3 (EEG 10/20 system) or 2) the Beam method. Both were estimations with some limitations. With the introduction of Neuronavigation, direct visualization of structures can be achieved either with an individual's (specially ordered) MRI or an average brain (MNI) stretched to the dimensions of the individual. There is now greater significance of this increased accuracy due to recent evidence that stimulation of the gyral crown is less effective than stimulation of the sulcal bank. The introduction of robotic controlled TMS also may make Neuronavigation more important. Several manufacturers offer complete systems including Ant Neuro or Axilum Robotics.
Another solution for TMS coil positioning is 3d printed patient specific guides in the form of a helmet based on MRI data.

Neuronavigation for Spine Surgery
Assistive technologies are used during spinal fusion surgery to increase accuracy, especially for the placement of pedicle screws.[1] A review of navigation techniques for spine surgery published in 2019 listed four currently available options:[2]
External links
- Soterix Medical - Neuronavigation for Transcranial Magnetic Stimulation
- American Association of Neurological Surgeons (AANS.org) | Library. Research List.
- The NeuralNavigator : A mobile MRI guided navigation system for TMS.
- Neggers SF, Langerak TR, Schutter DJ, et al. (April 2004). "A stereotactic method for image-guided transcranial magnetic stimulation validated with fMRI and motor-evoked potentials". NeuroImage. 21 (4): 1805–17. doi:10.1016/j.neuroimage.2003.12.006. PMID 15050601.
- ANT – Advanced Neuro Technology: Your single source for clinical and research neuroscience systems.
- TRACKER : software for frameless neuronavigation developed by MEVIS.
- ANT – Visor2.
- Rogue Research Brainsight.
- Localite TMS Navigator.
- Syneika One - Neuronavigation for Transcranial Magnetic Stimulation therapy
- Stimset - A 3d printed patient-specific TMS guide.
References
- Härtl R, Lam KS, Wang J, Korge A, Kandziora F, Audigé L (2013). "Worldwide survey on the use of navigation in spine surgery". World Neurosurgery. 79 (1): 162–172. doi:10.1016/j.wneu.2012.03.011. PMID 22469525.
- Malham, Gregory M; Wells-Quinn, Thomas (2019). "What should my hospital buy next?—Guidelines for the acquisition and application of imaging, navigation, and robotics for spine surgery". J Spine Surg. 5 (1): 155–165. doi:10.21037/jss.2019.02.04. PMC 6465454. PMID 31032450.
