Choking game
The choking game (also known as the fainting game, the Good Kids high[1] and a wide variety of slang terms) refers to intentionally cutting off oxygen to the brain with the goal of inducing temporary loss of consciousness and euphoria.
Reasons for practice
Limited research has been conducted regarding motivations for practicing the fainting game, although thrill-seeking has been identified as a risk factor,[2] as has the perception that it is a low-risk activity.[3] Anecdotal reasons stated include:
- Peer pressure, a challenge or dare, a rite of passage into a social group or amusement over erratic behavior.[4]
- Curiosity in experiencing an altered state of consciousness, the experience of a greyout, or an imagined approximation to a near-death experience.[4]
- A belief that it can induce a brief sense of euphoria (a rushing sensation or high).[2][4]
- The prospect of intoxication, albeit brief, at no financial cost.
Reasons for practice are distinct from erotic asphyxiation. Steve Field, chairman of the Royal College of General Practitioners in London,[5] claims that the fainting game is pursued primarily by children and teens "to get a high without taking drugs." Children "aren't playing this game for sexual gratification." It is frequently confused with erotic asphyxiation, which is oxygen deprivation for sexual arousal. Unlike erotic asphyxiation, practice of the fainting game appears to be uncommon in adulthood.[6]
Mechanisms of effect
There are two main mechanisms behind many variations of this practice, both resulting in cerebral hypoxia (oxygen deprivation to the brain). The two mechanisms tend to be confused with each other or treated as one but are quite dissimilar although both have the potential to cause permanent brain damage or death. The two mechanisms are strangulation and self-induced hypocapnia[7] and work as follows:
Strangulation
A ligature such as a belt or rope around the neck, or hands or arm pressure on the neck compresses the internal carotid artery. Apart from the direct restriction of blood to the brain there are two other significant responses produced by pressing on the neck:
- Pressing on the carotid arteries also presses on baroreceptors. These bodies then cause vasodilatation in the brain leading to insufficient blood to perfuse the brain with oxygen and maintain consciousness.
- A message is also sent via the vagus nerve to the main pacemaker of the heart to decrease the rate and volume of the heartbeat, typically by a third.[8] In some cases there is evidence that this may escalate into asystole, a form of cardiac arrest that is difficult to treat.[9] There is a dissenting view on the full extent how and when a person reaches a stage of permanent injury, but it is agreed that pressure on the vagus nerve causes changes to pulse rate and blood pressure and is dangerous in cases of carotid sinus hypersensitivity.
Increased breathing
The second mechanism requires hyperventilation (forced overbreathing) until symptoms of hypocapnia such as tingling, light-headedness or dizziness are felt, followed by a breath-hold. This alone is enough to cause a blackout, but it is widely believed that the effect is enhanced if lung air pressure is increased by holding the breath "hard" or "bearing down" (tightening the diaphragm as in a forced exhalation while allowing no air to escape or having an assistant apply a bear-hug).[10] These latter actions may augment the effects of hypoxia by approximating the Valsalva maneuver, causing vagal stimulation.
The hyperventilation leads to an excessive elimination of carbon dioxide (CO2) whereas no significant additional amounts of oxygen can be stocked in the body. As only carbon dioxide is responsible for the breathing stimulus, after hyperventilation, breath can be held longer until cerebral hypoxia occurs. The blood also becomes abnormally alkaline as a result of the excessive elimination of carbon dioxide; this subsequent rise in blood pH is termed alkalosis. Alkalosis interferes with normal oxygen utilization by the brain. The symptoms of alkalosis are neuromuscular irritability, muscular spasms, tingling and numbness of the extremities and around the mouth, and a dizziness, or giddiness, often interpreted as a sense of euphoria.
In the body alkalosis generally induces vasodilation (widening of the blood vessels) but in the brain alone it causes vasoconstriction (narrowing of the blood vessels). This vasoconstriction appears to be made even worse by a sudden increase in blood pressure caused by squeezing or holding the breath "hard". The alkalosis-induced euphoria can be followed rapidly by hypoxia-induced unconsciousness. The sequence of events leading to unconsciousness from hyperventilation is as follows:
- Decrease in partial pressure of alveolar CO2.
- Decrease in partial pressure of arterial CO2.
- Increase in blood pH, (respiratory alkalosis).
- Vasoconstriction of blood vessels supplying brain.
- Pooling of the blood present in the brain at the time.
- Brain rapidly uses up oxygen (O2) available in the pooled blood.
- O2 concentration in the brain drops.
- Unconsciousness from hypoxia of cerebral tissue.
Because the brain cannot store reserves of oxygen and, unlike other organs, has an exceedingly low tolerance of oxygen deprivation, it is highly vulnerable if vasoconstriction is not reversed. Normally, if the brain is hypoxic, autonomous systems in the body divert blood to the brain at the expense of other organs; because the brain is vasoconstricted this mechanism is not available. Vasoconstriction is only reversed by the build-up of carbon dioxide in the blood through suspension of breathing.
In some versions the bear-hug is replaced by pressure on the neck in which case blackout is a hybrid of strangulation and self-induced hypocapnia.
Other mechanisms
Unconsciousness may be induced by other methods although these are controversial: pressure over the carotid sinus may induce syncope (fainting) without any other action at all but this is difficult to reproduce and is not the basis of the game. For those susceptible to carotid sinus syncope, of which most people would be unaware until it occurred, this can be an exceedingly dangerous game.
In both strangulation and self-induced hypocapnia blackouts the victim may experience dreaming or hallucinations, though fleetingly, and regains consciousness with short-term memory loss and involuntary movement of their hands or feet. Full recovery is usually made within seconds if the strangulation stops.
Prevalence
A 2008 Centre for Addiction and Mental Health study found that at least 79,000 students in the Canadian province of Ontario participated in this act.[11] The 2006 Youth Health Risk Behavioral Survey in Williams County, Ohio found that 11% of youths aged 12–18 years and 19% of youths aged 17–18 reported ever having practiced it.[12]
Injuries and fatalities
Any activity that deprives the brain of oxygen has the potential to cause moderate to severe brain cell death leading to permanent loss of neurological function ranging from difficulty in concentration or loss of short term memory capacity through severe, lifelong mental disability to death.[13] Statistics on fatalities and neurological damage are controversial; no definitive, empirical study exists although the indications are that the practice is a significant contributor to death and disability, particularly among male juveniles in most developed countries. Many believe that deaths are significantly underreported because of false attributions to suicide.[14]
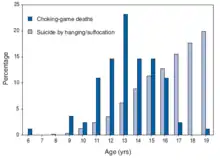
One study by the U.S. Centers for Disease Control and Prevention (CDC) found sufficient evidence to indicate that since 1995 at least 82 youths between the age of 6 and 19 have died in the United States as a result of the game (being roughly 1% of the deaths attributed to suicide by suffocation in the same age group), see chart on the right. Of these 86.6% were male, the mean age being 13.3. 95.7% of these deaths occurred while the youth was alone; parents of the decedents were unaware of the game in 92.9% of cases. Deaths were recorded in 31 states and were not clustered by location, season or day of week.[15] Neurological damage is harder to attribute accurately because of the difficulty of linking generalised, acquired neurological disability to a specific past event.
Incidental, or indirect, injuries may arise from falling or uncontrolled movements and crushing by a ligature or an assistant. Such injuries may include concussion, bone fractures, tongue biting and hemorrhaging of the eyes.[16]
The CDC encourages parents, educators and health-care providers to familiarize themselves with the signs of the game.[12] These include discussion of the game, bloodshot eyes, marks on the neck, severe headaches, disorientation after spending time alone, ropes, scarves, and belts tied to bedroom furniture or doorknobs or found knotted on the floor, and unexplained presence of things like dog leashes, choke collars and bungee cords.[17]
See also
- Asphyxia
- Blue Whale Challenge
- Death
- Shallow water blackout - for further discussion on the hyperventilation mechanism
- Momo Challenge hoax
References
- "Stopping the Choking Game". Culture of Safety. Retrieved 4 May 2020.
- Drake, Joseph A.; Price, James H.; Kolm-Valdivia, Nicole; Wielinski, Margaret (2010), "Association of Adolescent Choking Game Activity With Selected Risk Behaviors", Academic Pediatrics, 10 (6): 410–416, doi:10.1016/j.acap.2010.09.006, PMID 21075323
- Macnab, A.J.; Deevska, M.; Gagnon, F.; Cannon, W.G.; Andrew, T (2009), "Asphyxial games or "the choking game": a potentially fatal risk behaviour", Injury Prevention, 14 (1): 45–49, doi:10.1136/ip.2008.018523, PMID 19190276, S2CID 206981471, retrieved 26 October 2011
- Neal (2008), p.311
- Adams, William Lee (2010-01-18). "A Dangerous Pastime for Teens: The Choking Game". Time Magazine. Time. Retrieved 2010-01-21.
- Neal, Richard McKenzie (2008), "The choking game", The Path to Addiction: And Other Troubles We Are Born to Know, AuthorHouse, pp. 310–315 (see p.311), ISBN 978-1-4389-1674-3, retrieved 27 October 2011 Hardover ISBN 978-1-4389-1675-0
- Neal (2008), pp.312-313
- "Breath Play". Epedominion.com. Archived from the original on 2012-08-07. Retrieved 2012-08-19.
- Asystole~treatment at eMedicine
- Neal (2008), p.313 (hyperventilation)
- "Some 79,000 Ont. students play choking game: survey". CTV News. Archived from the original on 7 May 2008. Retrieved 12 May 2011.CS1 maint: bot: original URL status unknown (link)
- "Unintentional Strangulation Deaths from the "Choking Game" Among Youths Aged 6--19 Years --- United States, 1995--2007", Morbidity and Mortality Weekly Report of the Centers for Disease Control and Prevention, 57(06); 141-144, February 15, 2008 ("PDF version" (PDF).)
- "Headway UK Brain Injury Charity"
- Kids are passing out for a deadly high by Michael Okwu, Today, MSNBC.COM, February 26, 2008
- Centers for Disease Control and Prevention, (CDC) (Feb 15, 2008). "Unintentional strangulation deaths from the "choking game" among youths aged 6-19 years--United States, 1995-2007". MMWR. Morbidity and Mortality Weekly Report. 57 (6): 141–4. PMID 18272955.
- "'Choking Game' Turned Deadly for 82 Youths" by Amanda Gardner, The Washington Post, February 14, 2008
- "CDC Study Warns of Deaths Due to the 'Choking Game'" Archived 2010-03-28 at the Wayback Machine, Centers for Disease Control and Prevention press release, 14 February 2008
Further reading
- Andrew, Thomas A., & Fallon, Kim K.; Fallon (2007), "Asphyxial Games in Children and Adolescents" (PDF), The American Journal of Forensic Medicine and Pathology, 28 (4): 303–307, doi:10.1097/paf.0b013e318148bdb2, PMID 18043016, S2CID 26093452, retrieved 26 October 2011CS1 maint: multiple names: authors list (link)
- Bernacki, Jessica M; Davies, W. Hobart (2011), "Prevention of the Choking Game: Parent Perspectives", Journal of Injury and Violence Research, 4 (2. Article in press): 73–8, doi:10.5249/jivr.v4i2.119, PMC 3426904, PMID 21502782, retrieved 27 October 2011
- Cash, Ralph E (November 2007), A Dangerous High (PDF), National Association of School Psychologists, retrieved 27 October 2011
- Lieberman, Richard (2009), "Choking Game" (PDF), Youth Suicide Prevention Program Training for Crisis Teams and School Staff, Los Angeles Unified School District, pp. 3–4 See
- Martha Linkletter; Kevin Gordon; Joe Dooley (March 2010), "The Choking Game and YouTube: A Dangerous Combination" (PDF), Clinical Pediatrics, 49 (3): 274–279, CiteSeerX 10.1.1.1000.2089, doi:10.1177/0009922809339203, PMID 19596864, S2CID 33724693, archived from the original (PDF) on 2010-09-19, retrieved 26 October 2011
- McClave, Julie L.; Russell, Patricia J.; Lyren, Anne; O'Riordan, Mary Ann; Bass, Nancy E. (2010), "The Choking Game: Physician Perspectives", Pediatrics, 125 (1): 82–87, doi:10.1542/peds.2009-1287, PMID 20008424 Originally published online December 14, 2009
- Ramowski, S.K.; Nystrom, R.J.; Chaumeton, N.R.; Rosenberg, K.D. & Gilchrist, J. (2010), ""Choking Game" Awareness and Participation among 8th Graders - Oregon, 2008", Morbidity and Mortality Weekly Report, 59 (1): 1–5, retrieved 27 October 2011 Medscape News report
- Toblin, Robin L.; Paulozzi, Leonard J.; Gilchrist, Julie; Russell, Patricia J. (2008). "Unintentional strangulation deaths from the 'Choking Game' among youths aged 6-19 years – United States, 1995—2007". Journal of Safety Research. 39 (4): 445–8. doi:10.1016/j.jsr.2008.06.002. PMID 18786433.
- Urkin, Jacob; Merrick, Joav (2006), "The choking game or suffocation roulette in adolescence (editorial)", International Journal of Adolescent Medicine and Health, 18 (2): 207–208, doi:10.1515/IJAMH.2006.18.2.207, PMID 16894858, S2CID 31075593 Free abstract