Electrical injury
Electrical injury is a physiological reaction caused by electric current passing through the body.[2] The injury depends on the density of the current, tissue resistance and duration of contact.[3] Very small currents may be imperceptible or produce a light tingling sensation. A shock caused by low and otherwise harmless current could startle an individual and cause injury due to jerking away or falling. Stronger currents may cause some degree of discomfort or pain, while more intense currents may induce involuntary muscle contractions, preventing the person from breaking free of the source of electricity.[4] Still larger currents result in tissue damage and may trigger ventricular fibrillation or cardiac arrest. If death results from an electric shock the cause of death is generally referred to as electrocution.
| Electrical injury | |
|---|---|
| Other names | Electrical shock |
 | |
| Lightning injury caused by a nearby lightning strike. The slight branching redness (sometimes called a Lichtenberg figure) travelling up the leg was caused by the effects of current. | |
| Specialty | Emergency medicine |
| Complications | Burns, rhabdomyolysis, cardiac arrest, bone fractures[1] |
| Frequency | >30,000 per year (USA)[1] |
| Deaths | ~1,000 per year (USA)[1] |
Electric injury occurs upon contact of a body part with electricity that causes a sufficient current to pass through the person's tissue. Contact with energized wiring or devices is the most common cause. In cases of exposure to high voltages, such as on a power transmission tower, direct contact may not be necessary as the voltage may "jump" the air gap to the electrical device.
Following an electrical injury from household current, if a person has no symptoms, no underlying heart problems, and is not pregnant further testing is not required.[5] Otherwise an electrocardiogram, blood work to check the heart, and urine testing for signs of muscle breakdown may be performed.[5]
Management may involve resuscitation, pain medications, wound management, and heart monitoring.[5] Electrical injuries affect more than 30,000 people a year in the United States and result in about 1,000 deaths.[1]
Signs and symptoms
Burns

Heating due to resistance can cause extensive and deep burns. When applied to the hand, electricity can cause involuntary muscle contraction, producing the "no-let-go" phenomenon, and increasing the risk for serious burns.[6] Voltage levels of 500 to 1000 volts tend to cause internal burns due to the large energy (which is proportional to the duration multiplied by the square of the voltage divided by resistance) available from the source. Damage due to current is through tissue heating and/or electroporation injury. For most cases of high-energy electrical trauma, the Joule heating in the deeper tissues along the extremity will reach damaging temperatures in a few seconds.[7]
Ventricular fibrillation
A domestic power supply voltage (110 or 230 V), 50 or 60 Hz alternating current (AC) through the chest for a fraction of a second may induce ventricular fibrillation at currents as low as 30 milliamperes (mA).[8] With direct current (DC), 300 to 500 mA is required.[9] If the current has a direct pathway to the heart (e.g., via a cardiac catheter or other kind of electrode), a much lower current of less than 1 mA (AC or DC) can cause fibrillation. If not immediately treated by defibrillation, fibrillation is usually lethal because all of the heart muscle fibres move independently instead of in the coordinated pulses needed to pump blood and maintain circulation. Above 200 mA, muscle contractions are so strong that the heart muscles cannot move at all, but these conditions prevent fibrillation.
Neurological effects
Electrical current can cause interference with nervous control, especially over the heart and lungs. Electric shock which does not lead to death has been shown to cause neuropathy at the site where the current entered the body.[6] The neurologic symptoms of electrical injury may occur immediately, which traditionally have a higher likelihood for healing, though they may also be delayed by days to years.[6] The delayed neurologic consequences of electrical injury have a worse prognosis.[6]
When the patch of electrical current proceeds through the head, it appears that, with sufficient current applied, loss of consciousness almost always occurs swiftly. (This is borne out by some limited self-experimentation by early designers of the electric chair and by research from the field of animal husbandry, where electric stunning has been extensively studied).[10]
If ventricular fibrillation occurs (as above), the blood supply to the brain is diminished, which may cause cerebral hypoxia (and its associated neurologic consequences).
Mental health
There are a variety of psychiatric effects that may occur as a result of electrical injuries. Behavioral changes can occur as well, even if the path of electrical current did not proceed through the head.[6] Symptoms may include:[6]
- Depression, including feelings of low self-esteem and guilt
- Anxiety spectrum disorders, including posttraumatic stress disorder and fear of electricity
- Moodiness, including a lower threshold for frustration and "losing one's temper"
- Memory loss, decreased attention span, and difficulty learning
Arc-flash hazards
OSHA found that up to 80 percent of its electrical injuries involve thermal burns due to arcing faults.[11] The arc flash in an electrical fault produces the same type of light radiation from which electric welders protect themselves using face shields with dark glass, heavy leather gloves, and full-coverage clothing.[12] The heat produced may cause severe burns, especially on unprotected flesh. The arc blast produced by vaporizing metallic components can break bones and damage internal organs. The degree of hazard present at a particular location can be determined by a detailed analysis of the electrical system, and appropriate protection worn if the electrical work must be performed with the electricity on.
Pathophysiology
The minimum current a human can feel depends on the current type (AC or DC) as well as frequency for AC. A person can feel at least 1 mA (rms) of AC at 60 Hz, while at least 5 mA for DC. At around 10 mA, AC current passing through the arm of a 68-kilogram (150 lb) human can cause powerful muscle contractions; the victim is unable to voluntarily control muscles and cannot release an electrified object.[13] This is known as the "let go threshold" and is a criterion for shock hazard in electrical regulations.
The current may, if it is high enough and is delivered at sufficient voltage, cause tissue damage or fibrillation which can cause cardiac arrest; more than 30 mA[8] of AC (rms, 60 Hz) or 300 – 500 mA of DC at high voltage can cause fibrillation.[9][14] A sustained electric shock from AC at 120 V, 60 Hz is an especially dangerous source of ventricular fibrillation because it usually exceeds the let-go threshold, while not delivering enough initial energy to propel the person away from the source. However, the potential seriousness of the shock depends on paths through the body that the currents take.[9] If the voltage is less than 200 V, then the human skin, more precisely the stratum corneum, is the main contributor to the impedance of the body in the case of a macroshock—the passing of current between two contact points on the skin. The characteristics of the skin are non-linear however. If the voltage is above 450–600 V, then dielectric breakdown of the skin occurs.[15] The protection offered by the skin is lowered by perspiration, and this is accelerated if electricity causes muscles to contract above the let-go threshold for a sustained period of time.[9]
If an electrical circuit is established by electrodes introduced in the body, bypassing the skin, then the potential for lethality is much higher if a circuit through the heart is established. This is known as a microshock. Currents of only 10 µA can be sufficient to cause fibrillation in this case with a probability of 0.2%.[16]
Body resistance
| Voltage | 5% | 50% | 95% |
|---|---|---|---|
| 25 V | 1,750 Ω | 3,250 Ω | 6,100 Ω |
| 100 V | 1,200 Ω | 1,875 Ω | 3,200 Ω |
| 220 V | 1,000 Ω | 1,350 Ω | 2,125 Ω |
| 1000 V | 700 Ω | 1,050 Ω | 1,500 Ω |
The voltage necessary for electrocution depends on the current through the body and the duration of the current. Ohm's law states that the current drawn depends on the resistance of the body. The resistance of human skin varies from person to person and fluctuates between different times of day. The NIOSH states "Under dry conditions, the resistance offered by the human body may be as high as 100,000 ohms. Wet or broken skin may drop the body's resistance to 1,000 ohms," adding that "high-voltage electrical energy quickly breaks down human skin, reducing the human body's resistance to 500 ohms".[17]
The International Electrotechnical Commission gives the following values for the total body impedance of a hand to hand circuit for dry skin, large contact areas, 50 Hz AC currents (the columns contain the distribution of the impedance in the population percentile; for example at 100 V 50% of the population had an impedance of 1875Ω or less):[18]
Skin
The voltage-current characteristic of human skin is non-linear and depends on many factors such as intensity, duration, history, and frequency of the electrical stimulus. Sweat gland activity, temperature, and individual variation also influence the voltage-current characteristic of skin. In addition to non-linearity, skin impedance exhibits asymmetric and time varying properties. These properties can be modeled with reasonable accuracy.[19] Resistance measurements made at low voltage using a standard ohmmeter do not accurately represent the impedance of human skin over a significant range of conditions.
For sinusoidal electrical stimulation less than 10 volts, the skin voltage-current characteristic is quasilinear. Over time, electrical characteristics can become non-linear. The time required varies from seconds to minutes, depending on stimulus, electrode placement, and individual characteristics.
Between 10 volts and about 30 volts, skin exhibits non-linear but symmetric electrical characteristics. Above 20 volts, electrical characteristics are both non-linear and symmetric. Skin conductance can increase by several orders of magnitude in milliseconds. This should not be confused with dielectric breakdown, which occurs at hundreds of volts. For these reasons, current flow cannot be accurately calculated by simply applying Ohm's law using a fixed resistance model.
Point of entry
- Macroshock: Current across intact skin and through the body. Current from arm to arm, or between an arm and a foot, is likely to traverse the heart, therefore it is much more dangerous than current between a leg and the ground. This type of shock by definition must pass into the body through the skin.
- Microshock: Very small current source with a pathway directly connected to the heart tissue. The shock is required to be administered from inside the skin, directly to the heart i.e. a pacemaker lead, or a guide wire, conductive catheter etc. connected to a source of current. This is a largely theoretical hazard as modern devices used in these situations include protections against such currents.
Electrocution
The earliest usage of the term "electrocution" cited by the Oxford English Dictionary was a 1889 newspaper reference to the method of execution then being considered.[20] Shortly thereafter, in 1892, the term was used in Science to refer generically to death or injury caused by electricity.[20]
Factors in lethality of electric shock
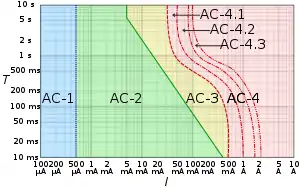
AC-1: imperceptible
AC-2: perceptible but no muscle reaction
AC-3: muscle contraction with reversible effects
AC-4: possible irreversible effects
AC-4.1: up to 5% probability of ventricular fibrillation
AC-4.2: 5-50% probability of fibrillation
AC-4.3: over 50% probability of fibrillation
The lethality of an electric shock is dependent on several variables:
- Current. The higher the current, the more likely it is lethal. Since current is proportional to voltage when resistance is fixed (ohm's law), high voltage is an indirect risk for producing higher currents.
- Duration. The longer the duration, the more likely it is lethal—safety switches may limit time of current flow
- Pathway. If current flows through the heart muscle, it is more likely to be lethal.
- High voltage (over about 600 volts). In addition to greater current flow, high voltage may cause dielectric breakdown at the skin, thus lowering skin resistance and allowing further increased current flow.
- Medical implants. Artificial cardiac pacemakers or implantable cardioverter-defibrillators (ICD) are sensitive to very small currents.[22]
- Pre-existing medical condition.[23]
- Age and sex.[24]
Other issues affecting lethality are frequency, which is an issue in causing cardiac arrest or muscular spasms. Very high frequency electric current causes tissue burning, but does not penetrate the body far enough to cause cardiac arrest (see electrosurgery). Also important is the pathway: if the current passes through the chest or head, there is an increased chance of death. From a main circuit or power distribution panel the damage is more likely to be internal, leading to cardiac arrest. Another factor is that cardiac tissue has a chronaxie (response time) of about 3 milliseconds, so electricity at frequencies of higher than about 333 Hz requires more current to cause fibrillation than is required at lower frequencies.
The comparison between the dangers of alternating current at typical power transmission frequences (i.e., 50 or 60 Hz), and direct current has been a subject of debate ever since the war of the currents in the 1880s. Animal experiments conducted during this time suggested that alternating current was about twice as dangerous as direct current per unit of current flow (or per unit of applied voltage).
It is sometimes suggested that human lethality is most common with alternating current at 100–250 volts; however, death has occurred below this range, with supplies as low as 42 volts.[25] Assuming a steady current flow (as opposed to a shock from a capacitor or from static electricity), shocks above 2,700 volts are often fatal, with those above 11,000 volts being usually fatal, though exceptional cases have been noted. According to a Guinness Book of World Records comic, seventeen-year-old Brian Latasa survived a 230,000 volt shock on the tower of an ultra-high voltage line in Griffith Park, Los Angeles on November 9, 1967.[26] A news report of the event stated that he was "jolted through the air, and landed across the line", and though rescued by firemen, he suffered burns over 40% of his body and was completely paralyzed except for his eyelids.[27] The shock with the highest voltage reported survived was that of Harry F. McGrew, who came in contact with a 340,000 volt transmission line in Huntington Canyon, Utah.[28]
Prevention
- Grounding the electrical enclosure of high-voltage machinery.
- Use of insulated gloves, insulated boots, mats and tools.
- Protecting electrical circuit with a residual-current device (RCD).
Epidemiology
There were 550 reported electrocutions in the US in 1993, 2.1 deaths per million inhabitants. At that time, the incidence of electrocutions was decreasing.[29] Electrocutions in the workplace make up the majority of these fatalities. From 1980–1992, an average of 411 workers were killed each year by electrocution.[17] A recent study conducted by the National Coroners Information System (NCIS) in Australia [30] has revealed three-hundred and twenty-one (321) closed case fatalities (and at least 39 case fatalities still under coronial investigation) that had been reported to Australian coroners where a person died from electrocution between July 2000 and October 2011.[31]
In Sweden, Denmark, Finland and Norway the number of electric deaths per million inhabitants was 0.6, 0.3, 0.3 and 0.2, respectively, in years 2007-2011.[32]
People who survive electrical trauma may suffer a host of injuries including loss of consciousness, seizures, aphasia, visual disturbances, headaches, tinnitus, paresis, and memory disturbances.[33] Even without visible burns, electric shock survivors may be faced with long-term muscular pain and discomfort, fatigue, headache, problems with peripheral nerve conduction and sensation, inadequate balance and coordination, among other symptoms. Electrical injury can lead to problems with neurocognitive function, affecting speed of mental processing, attention, concentration, and memory. The high frequency of psychological problems is well established and may be multifactorial.[33] As with any traumatic and life-threatening experience, electrical injury may result in post traumatic psychiatric disorders.[34] There exist several non-profit research institutes that coordinate rehabilitation strategies for electrical injury survivors by connecting them with clinicians that specialize in diagnosis and treatment of various traumas that arise as a result of electrical injury.[35][36]
Deliberate uses
Medical uses
Electric shock is also used as a medical therapy, under carefully controlled conditions:
- Electroconvulsive therapy or ECT, a psychiatric therapy for mental disorders
- As a surgical tool for cutting or coagulation. An electrosurgical unit (ESU) uses high currents (e.g. 10 amperes) at high frequency (e.g. 500 kHz) with various schemes of amplitude modulation to cut or coagulate
- As a treatment for fibrillation or irregular heart rhythms: see Defibrillation and Cardioversion
- As a method of pain relief: see Transcutaneous electrical nerve stimulation (TENS)
- As a treatment for excessive sweating with a process called iontophoresis
- Electrodiagnosis, for example nerve conduction studies and electromyography
- Electroporation for gene delivery
Entertainment

Mild electric shocks are also used for entertainment, especially as a practical joke for example in such devices as a shocking pen or a shocking gum. However devices such as a joy buzzer and most other machines in amusement parks today only use vibration that feels somewhat like an electric shock to someone not expecting it.
It is also used entertainingly for sex stimulation. This is usually done via the use of an erotic electrostimulator which induces erotic electrostimulation. These devices may include a violet wand, transcutaneous electrical nerve stimulation, electrical muscle stimulation, and made-for-play units.
Policing and personal defense
Electroshock weapons are incapacitant weapons used for subduing a person by administering electric shock to disrupt superficial muscle functions. One type is a conductive energy device (CED), an electroshock gun popularly known by the brand name "Taser", which fires projectiles that administer the shock through a thin, flexible wire. Although they are illegal for personal use in many jurisdictions, Tasers have been marketed to the general public.[38] Other electroshock weapons such as stun guns, stun batons ("cattle prods"), and electroshock belts administer an electric shock by direct contact.
Electric fences are barriers that uses electric shocks to deter animals or people from crossing a boundary. The voltage of the shock may have effects ranging from uncomfortable, to painful or even lethal. Most electric fencing is used today for agricultural fencing and other forms of animal control purposes, though it is frequently used to enhance security of restricted areas, and there exist places where lethal voltages are used.
Torture
Electric shocks are used as a method of torture, since the received voltage and current can be controlled with precision and used to cause pain and fear without always visibly harming the victim's body.
Electrical torture has been used in war and by repressive regimes since the 1930s.[39] The United States Army is known to have used electrical torture during World War II.[40] During the Algerian War electrical torture was a favorite method of French military forces.[41] Amnesty International published a statement that Russian military forces in Chechnya tortured local women with electric shocks by attaching wires onto their breasts.[42]
The parrilla (Spanish for 'grill') is a method of torture whereby the victim is strapped to a metal frame and subjected to electric shock.[43] It has been used in a number of contexts in South America. The parrilla was commonly used at Villa Grimaldi, a prison complex maintained by Dirección de Inteligencia Nacional, a part of the Pinochet regime.[44] In the 1970s, during the Dirty War, the parrilla was used in Argentina.[45] Francisco Tenório Júnior (known as Tenorinho), a Brazilian piano player, was subjected to the parrilla during the military dictatorship in Brazil.[46]
Advocates for the mentally ill and some psychiatrists such as Thomas Szasz have asserted that electroconvulsive therapy (ECT) is torture when used without a bona fide medical benefit against recalcitrant or non-responsive patients.[47][48][49]
The Judge Rotenberg Center has been condemned for torture by the United Nations special rapporteur on torture for its use of electric shocks as punishment as part of its behavior modification program.[50][51]
Japanese serial killer Futoshi Matsunaga used electric shocks to control his victims.[52]
Capital punishment
Electric shock delivered by an electric chair is sometimes used as an official means of capital punishment in the United States, although its use has become rare in recent times. Although some original proponents of the electric chair considered it to be a more humane execution method than hanging, shooting, poison gassing, etc., it has now generally been replaced by lethal injections in states that practice capital punishment. Modern reporting has claimed that it sometimes takes several shocks to be lethal, and that the condemned person may actually catch fire before the process is complete.
Other than in parts of the United States, only the Philippines reportedly has used this method, from 1926 to 1976. It was intermittently replaced by the firing squad, until the death penalty was abolished in that country. Electrocution remains legal in at least 5 states (Virginia, Florida, Alabama, North Carolina and Kentucky) of the United States.[53]
See also
- Electrocution
- Electrical burn
- Electromagnetism
- Graduated Electronic Decelerator
- Lichtenberg figure
- Lightning injuries
- Milgram experiment
- Residual-current device, a device used to protect against electric shocks
- Static electricity
- Transcutaneous electrical nerve stimulation
References
- Zemaitis, MR; Foris, LA; Lopez, RA; Huecker, MR (January 2020). "Electrical Injuries". PMID 28846317. Cite journal requires
|journal=(help) - Boon, Elizabeth; Parr, Rebecca; 20,000Dayananda, Samarawickrama (2012). Oxford Handbook of Dental Nursing. Oxford University Press. p. 132. ISBN 978-0191629860. Archived from the original on 2017-03-06.
- Reilly 1998, p. 1
- Leslie Alexander Geddes, Rebecca A. Roeder ,Handbook of Electrical Hazards and Accidents Lawyers & Judges Publishing Company, 2006 ISBN 0913875449, page 29
- "Electrical Injuries - Injuries; Poisoning". Merck Manuals Professional Edition. Retrieved 9 May 2020.
- Wesner, Marni; Hickie, John (2013). "Long-term sequelae of electrical injury". Can Fam Physician. 59 (9): 935–939. PMC 3771718. PMID 24029506.
- Lee, R. C.; Canaday, D. J.; Hammer, S. M. (1993). "Transient and stable ionic permeabilization of isolated skeletal muscle cells after electrical shock". The Journal of Burn Care & Rehabilitation. 14 (5): 528–40. doi:10.1097/00004630-199309000-00007. PMID 8245107.
- ucsb.edu - Electrical Safety Information - Physics Department, UCSB Archived 2013-10-23 at the Wayback Machine, 2012-01-09
- Clifford D. Ferris, Electric Shock, chapter 22.1 in Jerry C. Whitaker (ed.) The Electronics Handbook, CRC Press, 2005, ISBN 0-8493-1889-0, pp. 2317-2324
- Electric Stunning of Pigs and Sheep Archived 2016-03-06 at the Wayback Machine
- "Industry Backs IEEE-NFPA Arc Flash Testing Program with Initial Donations of $1.25 Million". IEEE. 14 July 2006. Archived from the original on 2 March 2008. Retrieved 2008-01-01.
- "Arc_flash_protection.php - Arc Flash". www.arcflash.com.au.
- John Cadick et. al (ed.) Electrical Safety Handbook Third Edition, McGraw Hill,2005 ISBN 0-07-145772-0 page 1-4
- Jack Hsu (2000). "Electric Current Needed to Kill a Human". The Physics Factbook. Archived from the original on 2013-10-23. Retrieved January 14, 2018.
- Reilly 1998, p. 30
- Norbert Leitgeb (6 May 2010). Safety of Electromedical Devices: Law - Risks - Opportunities. Springer Science & Business Media. p. 122. ISBN 978-3-211-99683-6. Archived from the original on 1 April 2017.
- "Publication No. 98-131: Worker Deaths by Electrocution" (PDF). National Institute for Occupational Safety and Health. Archived (PDF) from the original on 2008-10-11. Retrieved 2008-08-16.
- Reilly 1998, p. 43
- "The Voltage Current Characteristic of the Human Skin" (PDF). University of Pretoria. Archived (PDF) from the original on 2015-10-17.
- "electrocution". Oxford English Dictionary (Online ed.). Oxford University Press. (Subscription or participating institution membership required.)
- Weineng Wang, Zhiqiang Wang, Xiao Peng, Effects of the Earth Current Frequency and Distortion on Residual Current Devices Archived 2014-11-08 at the Wayback Machine, Scientific Journal of Control Engineering, Dec 2013, Vol 3 Issue 6 pp 417-422
- Claire M. Blandford (21 April 2016). Passing the Primary FRCA SOE: A Practical Guide. Cambridge University Press. pp. 117–. ISBN 978-1-107-54580-9. Archived from the original on 2 January 2018.
- Andrei G. Pakhomov; Damijan Miklavcic; Marko S. Markov (2 June 2010). Advanced Electroporation Techniques in Biology and Medicine. CRC Press. pp. 498–. ISBN 978-1-4398-1907-4. Archived from the original on 2 January 2018.
- John M Madden (20 January 2017). Electrical Safety and the Law. Taylor & Francis. p. 3. ISBN 978-1-317-20851-8. Archived from the original on 2 January 2018.
- "The Fatal Current". OSU Physics. Ohio State University. Archived from the original on 3 January 2018. Retrieved 4 March 2015.
- "According to Guinness (comic)". Toledo Blade. 1978-04-28.
- "Firemen risk death to save teenager". Ocala Star-Banner. 1967-11-24.
- https://archive.org/stream/in.ernet.dli.2015.115614/2015.115614.Guinness-World-Records_djvu.txt
- Folliot, Dominigue (1998). "Electricity: Physiological Effects". Encyclopaedia of Occupational Health and Safety, Fourth Edition. Archived from the original on 2007-02-28. Retrieved 2006-09-04.
- National Coroners Information System, NCIS Archived 2012-02-21 at the Wayback Machine
- Electrocution Related Deaths - National Coroners Information System (NCIS) Fact-Sheet, January 2012 Archived March 17, 2012, at the Wayback Machine
- Kinnunen, Minna (2013). "Electrical accident hazards in the Nordic countries" (PDF). Master's thesis, Tampere University of Technology. p. 19. Archived (PDF) from the original on 2014-03-27. Retrieved 2013-06-10.
- Pliskin, N. H.; Meyer, G. J.; Dolske, M. C.; Heilbronner, R. L.; Kelley, K. M.; Lee, R. C. (1994). "Neuropsychiatric Aspects of Electrical Injury". Annals of the New York Academy of Sciences. 720 (1): 219–23. Bibcode:1994NYASA.720..219P. doi:10.1111/j.1749-6632.1994.tb30450.x. PMID 8010642. S2CID 14913272.
- Grigorovich, Alisa; Gomez, Manuel; Leach, Larry; Fish, Joel (2013). "Impact of Posttraumatic Stress Disorder and Depression on Neuropsychological Functioning in Electrical Injury Survivors". Journal of Burn Care & Research. 34 (6): 659–65. doi:10.1097/BCR.0b013e31827e5062. PMID 23412330. S2CID 3698828.
- http://www.cetri.org Archived 2010-12-23 at the Wayback Machine
- "St. Johns Rehab - Electrical Injury Program - Sunnybrook Hospital". Archived from the original on 2013-10-04. Retrieved 2013-10-03.
- "Addams Family Generator - Arcade by H. Betti Industries, Inc". www.arcade-museum.com.
- International Association of Chiefs of Police, Electro Muscular Disruption Technology: A Nine-Step Strategy for Effective Deployment Archived December 10, 2013, at the Wayback Machine, 2005
- Technological Invention and Diffusion of Torture Equipment The Strange Case of Electric Torture Instruments in the Early 20th Century Archived March 5, 2010, at the Wayback Machine
- Rejali, Darius (2007-12-16). "Torture, American style: The surprising force behind torture: democracies". Boston Globe. Archived from the original on 2008-05-09. Retrieved 2008-01-01.
- Arens, Marianne; Thull, Françoise (April 9, 2001). "Torture in the Algerian war (1954-62) The Algerian war 1954-62". World Socialist Web Site. International Committee of the Fourth International (ICFI). Archived from the original on 2017-10-25. Retrieved 2 December 2017.
- "Russian Federation Preliminary briefing to the UN Committee against Torture". Archived from the original on May 16, 2009. Retrieved February 24, 2012.CS1 maint: unfit URL (link)
- Chile: Evidence of Torture. Amnesty International. 1983. pp. 3, 6. OCLC 1148222200.
- Gomez-Barris, Macarena (2009). Where Memory Dwells: Culture and State Violence in Chile. University of California Press. pp. 46–47. ISBN 978-0-520-25583-8.
- Feitlowitz, Marguerite (1999). A Lexicon of Terror: Argentina and the Legacies of Torture. New York: Oxford University Press. pp. 49, 57. OCLC 1035915088.
- McSherry, J. Patrice (2012-07-10). Predatory States: Operation Condor and Covert War in Latin America. Rowman & Littlefield. p. 188. ISBN 978-0-7425-6870-9.
- Israel, Matthew. "History and Basic Principles of JRC". Archived from the original on 2008-01-18. Retrieved 2007-12-22.
- Gonnerman, Jennifer (20 August 2007). "School of Shock". Mother Jones Magazine. Archived from the original on 22 December 2007. Retrieved 2007-12-22.
- Wen, P (2008-01-17). "Showdown over shock therapy". The Boston Globe. Archived from the original on 2010-03-13. Retrieved 2008-01-26.
- "UN Calls Shock Treatment at Mass. School 'Torture'". ABC News. Retrieved 2020-08-04.
- Fortin, Jacey (2020-03-06). "F.D.A. Bans School Electric Shock Devices". The New York Times. ISSN 0362-4331. Retrieved 2020-08-04.
- "Serial killer's death sentence upheld". Asahi Shimbun. 2007-09-27. Archived from the original on 2016-05-15. Retrieved 2008-03-21.
- Death Penalty Information Center Archived May 23, 2015, at the Wayback Machine
External links
| Classification |
|---|