Human T-lymphotropic virus 2
A virus closely related to HTLV-I, human T-lymphotropic virus 2 (HTLV-II) shares approximately 70% genomic homology (structural similarity) with HTLV-I. It was discovered by Robert Gallo and colleagues.[1][2]
| Human T-lymphotropic virus 2 | |
|---|---|
| Specialty | Infectious diseases |
| Symptoms | Mild cognitive Impairment, Mycosis fungoides |
| Duration | Chronic, incurable |
| Causes | HTLV-2 |
| Risk factors | Unsafe sex, haemophiliacs |
| Diagnostic method | Blood test |
| Differential diagnosis | HIV/AIDS, Lymphoma, HTLV-1 |
| Prevention | Practicing safe-sex, use of clean needles, screening blood transfusions, Avoiding breastfeeding. |
| Medication | Antiretrovirals, chemotherapy |
| Prognosis | 95% present with no symptoms, generally good |
| Frequency | 15-20 million people worldwide |
| Human T-lymphotropic virus_2 | |
|---|---|
| Virus classification | |
| Group: | Group VI (ssRNA-RT) |
| Order: | |
| Family: | |
| Subfamily: | Orthoretrovirinae |
| Genus: | |
| Species: | Primate T-lymphotropic virus 2 |
HTLV-2 is prevalent among the indigenous populations in Africa and the Indian-American tribes in Central and South America as well as among drug users in Europe and North America[3] It can be passed down from mother to child through breastmilk and genetically as well from either parent.
HTLV-II entry in target cells is mediated by the glucose transporter GLUT1.[4]
Virology
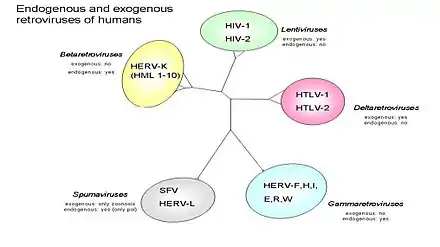
HTLV-1 and HTLV-2 share broad similarities in their overall genetic organization and expression pattern, but they differ substantially in their pathogenic properties.[3] The virus utilizes the GLUT-1 and NRP1 cellular receptors for their entry, although HTLV-1, but not HTLV-2, is dependent on heparan sulfate proteoglycans. Cell-to-cell transmission is essential for virus replication and occurs through the formation of a virological synapse.[3] The family of Human T-lymphotropic virus (Figure 2) can be further categorized into four sub types. The figure also divides the retroviruses into exogenous and endogenous. Retroviruses can exist as two different forms: endogenous which consist of normal genetic components and exogenous which are horizontally transferred genetic components that are usually infectious agents that cause disease i.e. HIV. In (Figure 3) open reading frames (ORF) are shown which can if translated can predict which genes will be present and this can help to better understand human retroviruses. Of the four subtypes, HTLV-2 may be linked to Cutaneous T-cell lymphoma (CTCL).[5] In one study involving cultured lymphocytes from patients with mycosis fungoides (Figure 1), PCR amplification showed gene sequences of HTLV-II. This finding may suggest a possible correlation with HTLV-2 and CTCL. Further research and studies must be conducted to show a positive relationship.[1]
Transmission
Perinatal transmission and breastfeeding and through blood transfusion, sexual contact, and use of intravenous drugs.[3]
Epidemology
HTLV-1 and HTLV-2 are both involved in actively spreading epidemics, affecting 15-20 million people worldwide. [4] In the United States, the overall prevalence is 22 per 100,000 population, with HTLV-2 more common than HTLV-1. Data collection performed from 2000 to 2009 among US blood donors has shown a general decline since the 1990s.[6]
Symptoms
Human T- leukemia, type 2 (HTLV-2) generally causes no signs or symptoms. Although HTLV-2 has not been definitively linked with any specific health problems, scientists suspect that some affected people may later develop neurological problems such as:[7][6]
- Sensory neuropathies (conditions that affect the nerves that provide feeling)
- Gait abnormalities
- Bladder dysfunction
- Mild cognitive impairment
- Motor abnormalities (loss of or limited muscle control or movement, or limited mobility)
- Erectile dysfunction
- Mycosis fungoides

Although evidence is limited, there may also be a link between HTLV-2 and chronic lung infections (i.e. pneumonia and bronchitis), asthma and dermatitis.[8]
Clinical significance
HTLV-II has not been clearly linked to any disease, but has been associated with several cases of myelopathy/tropical spastic paraparesis (HAM/TSP)- like neurological disease and may cause chronic lung problems.
An impact on platelet count has been observed.[9]
In the 1980s, HTLV-2 was identified in a patient with an unidentified T cell lymphoproliferative disease that was described as having characteristics similar to the B cell disorder, hairy cell leukemia.[10] HTLV-2 was identified in a second patient with a T cell lymphoproliferative disease; this patient later developed hairy cell leukemia, but HTLV-2 was not found in the hairy cell clones.[11] The cause of hairy cell leukemia is not known, but it is no longer believed to be related to viral infections.
Treatment
There are few treatments [12] including chemotherapy and antiretrovirals that can slow the viral load but no cure or definitive treatment exists for HTLV-2.[8]
Diagnosis
Human T- leukemia, type 2 (HTLV-2) is usually diagnosed based on blood tests that detect to the virus. However, HTLV-2 is often never suspected or diagnosed since most people never develop any signs or symptoms of the infection. Diagnosis may occur during for blood donation, testing performed due to an infection, or a work-up for an HTLV-2-associated medical problems.[8]
Prevention
Due to there being no cure for HTLV II the prevention is focused on early detection and preventing the spread of HTLV-2 to others. blood donors, promoting safe sex and discouraging needle sharing can decrease the number of new infections. Mother-to-child transmission can be reduced by screening pregnant women so infected mothers can avoid breastfeeding.[8]
Prognosis
The long-term outlook for most people infected with HTLV-2 is good. Infection with HTLV-2 is lifelong, but 95% of affected people have no signs or symptoms of the condition. Although, HTLV-2-related health problems tend to be significantly milder than those associated with HTLV1.[8]
References
- Geskin, Larisa J.; Pomerantz, Rebecca G.; Mirvish, Ezra D. (2011-02-01). "Infectious agents in cutaneous T-cell lymphoma". Journal of the American Academy of Dermatology. 64 (2): 423–431. doi:10.1016/j.jaad.2009.11.692. ISSN 0190-9622. PMC 3954537. PMID 20692726.
- "Robert gallo discovers htlv2 and 1". Retrieved 23 February 2019.
- Ciminale, Vincenzo; Rende, Francesca; Bertazzoni, Umberto; Romanelli, Maria G. (2014-07-29). "HTLV-1 and HTLV-2: highly similar viruses with distinct oncogenic properties". Frontiers in Microbiology. 5: 398. doi:10.3389/fmicb.2014.00398. ISSN 1664-302X. PMC 4114287. PMID 25120538.
- Manel N, Kim FJ, Kinet S, Taylor N, Sitbon M, Battini JL (November 2003). "The ubiquitous glucose transporter GLUT-1 is a receptor for HTLV". Cell. 115 (4): 449–59. doi:10.1016/S0092-8674(03)00881-X. PMID 14622599.
- "Journal of the American Academy of Dermatology". www.jaad.org. Retrieved 2019-02-22.
- "Human T-Cell Lymphotropic Viruses (HTLV)". Medscape. Retrieved 22 February 2019.
- "HTLV Type I and Type II". NORD (National Organization for Rare Disorders). Retrieved 2019-02-22.
- "Human T-cell leukemia virus type 2". US Department of Health and Human Services | Genetic and Rare Diseases Information Center (GARD) – an NCATS Program. Retrieved 2019-02-22.
 This article incorporates text from this source, which is in the public domain.
This article incorporates text from this source, which is in the public domain. - Bartman MT, Kaidarova Z, Hirschkorn D, et al. (November 2008). "Long-term increases in lymphocytes and platelets in human T-lymphotropic virus type II infection". Blood. 112 (10): 3995–4002. doi:10.1182/blood-2008-05-155960. PMC 2581993. PMID 18755983.
- Kalyanaraman VS, Sarngadharan MG, Robert-Guroff M, Miyoshi I, Golde D, Gallo RC (November 1982). "A new subtype of human T-cell leukemia virus (HTLV-II) associated with a T-cell variant of hairy cell leukemia". Science. 218 (4572): 571–3. Bibcode:1982Sci...218..571K. doi:10.1126/science.6981847. PMID 6981847.
- Rosenblatt JD, Giorgi JV, Golde DW, et al. (February 1988). "Integrated human T-cell leukemia virus II genome in CD8 + T cells from a patient with "atypical" hairy cell leukemia: evidence for distinct T and B cell lymphoproliferative disorders". Blood. 71 (2): 363–9. doi:10.1182/blood.V71.2.363.363. PMID 2827811. Retrieved 10 July 2020.
- Gotuzzo, Eduardo; Vanham, Guido; Vandamme, Anne-Mieke; Dooren, Sonia Van; González, Elsa; Verdonck, Kristien (2007-04-01). "Human T-lymphotropic virus 1: recent knowledge about an ancient infection". The Lancet Infectious Diseases. 7 (4): 266–281. doi:10.1016/S1473-3099(07)70081-6. ISSN 1473-3099. PMID 17376384.
External links
- "Human T-lymphotropic virus 2". NCBI Taxonomy Browser. 11909.
- International Retrovirology Association
- Human+T-lymphotropic+virus+2 at the US National Library of Medicine Medical Subject Headings (MeSH)