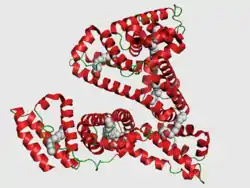
Human serum albumin
Human serum albumin is the serum albumin found in human blood. It is the most abundant protein in human blood plasma; it constitutes about half of serum protein. It is produced in the liver. It is soluble in water, and it is monomeric.


Albumin transports hormones, fatty acids, and other compounds, buffers pH, and maintains oncotic pressure, among other functions.
Albumin is synthesized in the liver as preproalbumin, which has an N-terminal peptide that is removed before the nascent protein is released from the rough endoplasmic reticulum. The product, proalbumin, is in turn cleaved in the Golgi apparatus to produce the secreted albumin.
The reference range for albumin concentrations in serum is approximately 35–50 g/L (3.5–5.0 g/dL).[5] It has a serum half-life of approximately 21 days.[6] It has a molecular mass of 66.5 kDa.
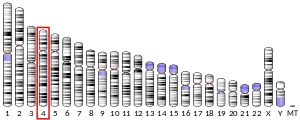
The gene for albumin is located on chromosome 4 in locus 4q13.3 and mutations in this gene can result in anomalous proteins. The human albumin gene is 16,961 nucleotides long from the putative 'cap' site to the first poly(A) addition site. It is split into 15 exons that are symmetrically placed within the 3 domains thought to have arisen by triplication of a single primordial domain.
Prolonged release of drugs
Cancer is the uncontrolled growth of cells with loss of differentiation and commonly with metastasis. Anticancer drugs are used to control the growth of cancerous cells. Oxaliplatin is a third-generation platinum-derived antineoplastic agent that has been proved effective mainly against advanced colorectal cancer (CRC). Oxaliplatin administration has an acute excitatory and sensitizing effect, including unpleasant cold allodynia in the distal extremities, mouth, and throat and usually associated with muscle cramps. However, the major side effect, a dose-limiting toxicity of the peripheral nerves, affects the sustainability of the planned treatment. Although these acute symptoms resolve within 1 week, severe chronic sensory neuropathy develops with the increasing cumulative dose and is characterized by distal paresthesia and numbness.[7][8] Drug delivery systems aim to deliver the drugs over an extended duration or at a specific time during treatment. Therefore, the improvement of the efficiency and convenience of a drug release system is of paramount importance. In the past two decades, numerous nanoparticles (NPs) have been extensively explored in order to achieve precisely controlled drug delivery.[9] However, the application and development of high-efficiency drug release system are still limited due to a lacking of simple, stable and efficient drug delivery vehicle. Human serum albumin (HSA) is a highly water-soluble globular monomeric plasma protein with a relative molecular weight of 67 KDa, consisting of 585 amino acid residues, one sulfhydryl group and 17 disulfide bridges. Among nanoparticulate carriers, HSA nanoparticles have long been the center of attention in the pharmaceutical industry due to their ability to bind to various drug molecules, great stability during storage and in vivo usage, no toxicity and antigenicity, biodegradability, reproducibility, scale up of the production process and a better control over release properties. In addition, significant amounts of drug can be incorporated into the particle matrix because of the large number of drug binding sites on the albumin molecule.[10]
Function
- Maintains oncotic pressure
- Transports thyroid hormones
- Transports other hormones, in particular, ones that are fat-soluble
- Transports fatty acids ("free" fatty acids) to the liver and to myocytes for utilization of energy
- Transports unconjugated bilirubin
- Transports many drugs; serum albumin levels can affect the half-life of drugs. Competition between drugs for albumin binding sites may cause drug interaction by increasing the free fraction of one of the drugs, thereby affecting potency.
- Competitively binds calcium ions (Ca2+)
- Serum albumin, as a negative acute-phase protein, is down-regulated in inflammatory states. As such, it is not a valid marker of nutritional status; rather, it is a marker of an inflammatory state
- Prevents photodegradation of folic acid
- Prevent pathogenic effects of Clostridium difficile toxins[11]
Measurement
Serum albumin is commonly measured by recording the change in absorbance upon binding to a dye such as bromocresol green or bromocresol purple.[12]
Reference ranges
The normal range of human serum albumin in adults (> 3 y.o.) is 3.5–5.0 g/dL (35–50 g/L). For children less than three years of age, the normal range is broader, 2.9–5.5 g/dL.[13]
Low albumin (hypoalbuminemia) may be caused by liver disease, nephrotic syndrome, burns, protein-losing enteropathy, malabsorption, malnutrition, late pregnancy, artefact, genetic variations and malignancy.
High albumin (hyperalbuminemia) is almost always caused by dehydration. In some cases of retinol (Vitamin A) deficiency, the albumin level can be elevated to high-normal values (e.g., 4.9 g/dL). This is because retinol causes cells to swell with water (this is also the reason too much Vitamin A is toxic).[14] This swelling also likely occurs during treatment with 13-cis retinoic acid (isotretnoin), a pharmaceutical for treating severe acne, amongst other conditions. In lab experiments it has been shown that all-trans retinoic acid down regulates human albumin production.[15]
Pathology
Hypoalbuminemia
Hypoalbuminemia means low blood albumin levels.[16] This can be caused by:
- Liver disease; cirrhosis of the liver is most common
- Excess excretion by the kidneys (as in nephrotic syndrome)
- Excess loss in bowel (protein-losing enteropathy, e.g., Ménétrier's disease)
- Burns (plasma loss in the absence of skin barrier)
- Redistribution (hemodilution [as in pregnancy], increased vascular permeability or decreased lymphatic clearance)
- Acute disease states (referred to as a negative acute-phase protein)
- Malnutrition and wasting[17]
- Mutation causing analbuminemia (very rare)
- Anorexia nervosa (most common cause in adolescents)
Hyperalbuminemia
Hyperalbuminemia is an increased concentration of albumin in the blood.[18] Typically, this condition is due to dehydration.[18] Hyperalbuminemia has also been associated with high protein diets.[19]
Medical use
Human albumin solution (HSA) is available for medical use, usually at concentrations of 5–25%.
Human albumin is often used to replace lost fluid and help restore blood volume in trauma, burns and surgery patients. There is no strong medical evidence that albumin administration (compared to saline) saves lives for people who have hypovolaemia or for those who are critically ill due to burns or hypoalbuminaemia.[20] It is also not known if there are people who are critically ill that may benefit from albumin.[20] Therefore, the Cochrane Collaboration recommends that it should not be used, except in clinical trials.[21]
In acoustic droplet vaporization (ADV), albumin is sometimes used as a surfactant. ADV has been proposed as a cancer treatment by means of occlusion therapy.[22]
Human serum albumin may be used to potentially reverse drug/chemical toxicity by binding to free drug/agent.[23]
Human albumin may also be used in treatment of decompensated cirrhosis.[24]
Human serum albumin has been used as a component of a frailty index.[17]
It has not been shown to give better results than other fluids when used simply to replace volume, but is frequently used in conditions where loss of albumin is a major problem, such as liver disease with ascites.
Glycation
It has been known for a long time that human blood proteins like hemoglobin[25] and serum albumin[26][27] may undergo a slow non-enzymatic glycation, mainly by formation of a Schiff base between ε-amino groups of lysine (and sometimes arginine) residues and glucose molecules in blood (Maillard reaction). This reaction can be inhibited in the presence of antioxidant agents.[28] Although this reaction may happen normally,[26] elevated glycoalbumin is observed in diabetes mellitus.[27]
Glycation has the potential to alter the biological structure and function of the serum albumin protein.[29][30][31][32]
Moreover, the glycation can result in the formation of Advanced Glycation End-Products (AGE), which result in abnormal biological effects. Accumulation of AGEs leads to tissue damage via alteration of the structures and functions of tissue proteins, stimulation of cellular responses, through receptors specific for AGE-proteins, and generation of reactive oxygen intermediates. AGEs also react with DNA, thus causing mutations and DNA transposition. Thermal processing of proteins and carbohydrates brings major changes in allergenicity. AGEs are antigenic and represent many of the important neoantigens found in cooked or stored foods.[33] They also interfere with the normal product of nitric oxide in cells.[34]
Although there are several lysine and arginine residues in the serum albumin structure, very few of them can take part in the glycation reaction.[27][35]
Oxidation
The albumin is the predominant protein in most body fluids, its Cys34 represents the largest fraction of free thiols within body. The albumin Cys34 thiol exists in both reduced and oxidized forms.[36] In plasma of healthy young adults, 70–80% of total HSA contains the free sulfhydryl group of Cys34 in a reduced form or mercaptoalbumin (HSA-SH).[37] However, in pathological states characterized by oxidative stress and during the aging process, the oxidized form, or non-mercaptoalbumin (HNA), could predominate.[38] The albumin thiol reacts with radical hydroxyl (.OH), hydrogen peroxide (H2O2) and the reactive nitrogen species as peroxynitrite (ONOO.), and have been shown to oxidize Cys34 to sulfenic acid derivate (HSA-SOH), it can be recycled to mercapto-albumin; however at high concentrations of reactive species leads to the irreversible oxidation to sulfinic (HSA-SO2H) or sulfonic acid (HSA-SO3H) affecting its structure.[39] Presence of reactive oxygen species (ROS), can induce irreversible structural damage and alter protein activities.
Loss via kidneys
In the healthy kidney, albumin's size and negative electric charge exclude it from excretion in the glomerulus. This is not always the case, as in some diseases including diabetic nephropathy, which can sometimes be a complication of uncontrolled or of longer term diabetes in which proteins can cross the glomerulus. The lost albumin can be detected by a simple urine test.[40] Depending on the amount of albumin lost, a patient may have normal renal function, microalbuminuria, or albuminuria.
Interactions
Human serum albumin has been shown to interact with FCGRT.[41]
It might also interact with a yet-unidentified albondin (gp60), a certain pair of gp18/gp30, and some other proteins like osteonectin, hnRNPs, calreticulin, cubilin, and megalin.[42]
See also
References
- GRCh38: Ensembl release 89: ENSG00000163631 - Ensembl, May 2017
- GRCm38: Ensembl release 89: ENSMUSG00000029368 - Ensembl, May 2017
- "Human PubMed Reference:". National Center for Biotechnology Information, U.S. National Library of Medicine.
- "Mouse PubMed Reference:". National Center for Biotechnology Information, U.S. National Library of Medicine.
- "Harmonisation of Reference Intervals" (PDF). pathologyharmony.co.uk. Pathology Harmony. Archived from the original (PDF) on 2 August 2013. Retrieved 23 June 2013.
- "Hypoalbuminemia: Background, Pathophysiology, Etiology". Medscape Reference. 2019-11-10. Retrieved 2019-12-22.
- Kokotis P, Schmelz M, Kostouros E, Karandreas N, Dimopoulos MA (September 2016). "Oxaliplatin-Induced Neuropathy: A Long-Term Clinical and Neurophysiologic Follow-Up Study". Clinical Colorectal Cancer. 15 (3): e133-40. doi:10.1016/j.clcc.2016.02.009. PMID 27038553.
- Krishnan AV, Goldstein D, Friedlander M, Kiernan MC (July 2005). "Oxaliplatin-induced neurotoxicity and the development of neuropathy". Muscle & Nerve. 32 (1): 51–60. doi:10.1002/mus.20340. PMID 15880395. S2CID 23098627.
- Kaur IP, Singh H (June 2014). "Nanostructured drug delivery for better management of tuberculosis". Journal of Controlled Release. 184: 36–50. doi:10.1016/j.jconrel.2014.04.009. PMID 24732260.
- Kouchakzadeh H, Shojaosadati SA, Shokri F (September 2014). "Efficient loading and entrapment of tamoxifen in human serum albumin based nanoparticulate delivery system by a modified desolvation technique". Chemical Engineering Research and Design. 92 (9): 1681–1692. doi:10.1016/j.cherd.2013.11.024.
- di Masi A, Leboffe L, Polticelli F, Tonon F, Zennaro C, Caterino M, Stano P, Fischer S, Hägele M, Müller M, Kleger A, Papatheodorou P, Nocca G, Arcovito A, Gori A, Ruoppolo M, Barth H, Petrosillo N, Ascenzi P, Di Bella S (September 2018). "Human Serum Albumin Is an Essential Component of the Host Defense Mechanism Against Clostridium difficile Intoxication". The Journal of Infectious Diseases. 218 (9): 1424–1435. doi:10.1093/infdis/jiy338. PMID 29868851.
- "Albumin: analyte monograph" (PDF). Association for Clinical Biochemistry and Laboratory Medicine. Archived from the original (PDF) on 13 November 2012. Retrieved 23 June 2013.
- "Normal Ranges for Common Laboratory Tests". Archived from the original on 2013-01-14. Retrieved 2007-12-06.CS1 maint: bot: original URL status unknown (link) Rush University
- Pasantes-Morales H, Wright CE, Gaull GE (December 1984). "Protective effect of taurine, zinc and tocopherol on retinol-induced damage in human lymphoblastoid cells". The Journal of Nutrition. 114 (12): 2256–61. doi:10.1093/jn/114.12.2256. PMID 6502269.
- Masaki T, Matsuura T, Ohkawa K, Miyamura T, Okazaki I, Watanabe T, Suzuki T (July 2006). "All-trans retinoic acid down-regulates human albumin gene expression through the induction of C/EBPbeta-LIP". The Biochemical Journal. 397 (2): 345–53. doi:10.1042/BJ20051863. PMC 1513275. PMID 16608438.
- Anderson DM (2000). Dorland's illustrated medical dictionary (29th ed.). Philadelphia [u.a.]: Saunders. p. 860. ISBN 978-0721682617.
- Green P, Woglom AE, Genereux P, Daneault B, Paradis JM, Schnell S, Hawkey M, Maurer MS, Kirtane AJ, Kodali S, Moses JW, Leon MB, Smith CR, Williams M (September 2012). "The impact of frailty status on survival after transcatheter aortic valve replacement in older adults with severe aortic stenosis: a single-center experience". JACC. Cardiovascular Interventions. 5 (9): 974–81. doi:10.1016/j.jcin.2012.06.011. PMC 3717525. PMID 22995885.
- Busher JT (1990). "Chapter 101: Serum Albumin and Globulin". In Walker HK, Hall WD, Hurst JW (eds.). Clinical methods : the history, physical, and laboratory examinations (3rd ed.). Boston: Butterworths. ISBN 978-0409900774.
- Mutlu EA, Keshavarzian A, Mutlu GM (June 2006). "Hyperalbuminemia and elevated transaminases associated with high-protein diet". Scandinavian Journal of Gastroenterology. 41 (6): 759–60. doi:10.1080/00365520500442625. PMID 16716979. S2CID 21264934.
- Roberts I, Blackhall K, Alderson P, Bunn F, Schierhout G (November 2011). "Human albumin solution for resuscitation and volume expansion in critically ill patients". The Cochrane Database of Systematic Reviews (11): CD001208. doi:10.1002/14651858.CD001208.pub4. hdl:2299/5243. PMC 7055200. PMID 22071799.
- Roberts I, Blackhall K, Alderson P, Bunn F, Schierhout G (November 2011). "Human albumin solution for resuscitation and volume expansion in critically ill patients". The Cochrane Database of Systematic Reviews (11): CD001208. doi:10.1002/14651858.CD001208.pub4. PMC 7055200. PMID 22071799.
- Lo AH, Kripfgans OD, Carson PL, Rothman ED, Fowlkes JB (May 2007). "Acoustic droplet vaporization threshold: effects of pulse duration and contrast agent". IEEE Transactions on Ultrasonics, Ferroelectrics, and Frequency Control. 54 (5): 933–46. doi:10.1109/tuffc.2007.339. PMID 17523558. S2CID 11983041.
- Ascenzi P, Leboffe L, Toti D, Polticelli F, Trezza V (August 2018). "Fipronil recognition by the FA1 site of human serum albumin". Journal of Molecular Recognition. 31 (8): e2713. doi:10.1002/jmr.2713. PMID 29656610. S2CID 4894574.
- Caraceni P, Riggio O, Angeli P, Alessandria C, Neri S, Foschi FG, et al. (June 2018). "Long-term albumin administration in decompensated cirrhosis (ANSWER): an open-label randomised trial". Lancet. 391 (10138): 2417–2429. doi:10.1016/S0140-6736(18)30840-7. hdl:2108/208667. PMID 29861076. S2CID 44120418.
- Rahbar S (October 1968). "An abnormal hemoglobin in red cells of diabetics". Clinica Chimica Acta; International Journal of Clinical Chemistry. 22 (2): 296–8. doi:10.1016/0009-8981(68)90372-0. PMID 5687098.
- Day JF, Thorpe SR, Baynes JW (February 1979). "Nonenzymatically glucosylated albumin. In vitro preparation and isolation from normal human serum". The Journal of Biological Chemistry. 254 (3): 595–7. PMID 762083.
- Iberg N, Flückiger R (October 1986). "Nonenzymatic glycosylation of albumin in vivo. Identification of multiple glycosylated sites". The Journal of Biological Chemistry. 261 (29): 13542–5. PMID 3759977.
- Jakus V, Hrnciarová M, Cársky J, Krahulec B, Rietbrock N (1999). "Inhibition of nonenzymatic protein glycation and lipid peroxidation by drugs with antioxidant activity". Life Sciences. 65 (18–19): 1991–3. doi:10.1016/S0024-3205(99)00462-2. PMID 10576452.
- Mohamadi-Nejad A, Moosavi-Movahedi AA, Hakimelahi GH, Sheibani N (September 2002). "Thermodynamic analysis of human serum albumin interactions with glucose: insights into the diabetic range of glucose concentration". The International Journal of Biochemistry & Cell Biology. 34 (9): 1115–24. doi:10.1016/S1357-2725(02)00031-6. PMID 12009306.
- Shaklai N, Garlick RL, Bunn HF (March 1984). "Nonenzymatic glycosylation of human serum albumin alters its conformation and function". The Journal of Biological Chemistry. 259 (6): 3812–7. PMID 6706980.
- Mendez DL, Jensen RA, McElroy LA, Pena JM, Esquerra RM (December 2005). "The effect of non-enzymatic glycation on the unfolding of human serum albumin". Archives of Biochemistry and Biophysics. 444 (2): 92–9. doi:10.1016/j.abb.2005.10.019. PMID 16309624.
- Mohamadi-Nejada A, Moosavi-Movahedi AA, Safariana S, Naderi-Maneshc MH, Ranjbarc B, Farzamid B, Mostafavie H, Larijanif MB, Hakimelahi GH (July 2002). "The thermal analysis of nonezymatic glycosylation of human serum albumin: differential scanning calorimetry and circular dichroism studies". Thermochimica Acta. 389 (1–2): 141–151. doi:10.1016/S0040-6031(02)00006-0.
- Kańska U, Boratyński J (2002). "Thermal glycation of proteins by D-glucose and D-fructose". Archivum Immunologiae et Therapiae Experimentalis. 50 (1): 61–6. PMID 11916310.
- Rojas A, Romay S, González D, Herrera B, Delgado R, Otero K (February 2000). "Regulation of endothelial nitric oxide synthase expression by albumin-derived advanced glycosylation end products". Circulation Research. 86 (3): E50-4. doi:10.1161/01.RES.86.3.e50. PMID 10679490.
- Garlick RL, Mazer JS (May 1983). "The principal site of nonenzymatic glycosylation of human serum albumin in vivo". The Journal of Biological Chemistry. 258 (10): 6142–6. PMID 6853480.
- Kawakami A, Kubota K, Yamada N, Tagami U, Takehana K, Sonaka I, Suzuki E, Hirayama K (July 2006). "Identification and characterization of oxidized human serum albumin. A slight structural change impairs its ligand-binding and antioxidant functions". The FEBS Journal. 273 (14): 3346–57. doi:10.1111/j.1742-4658.2006.05341.x. PMID 16857017. S2CID 12844381.
- Turell L, Carballal S, Botti H, Radi R, Alvarez B (April 2009). "Oxidation of the albumin thiol to sulfenic acid and its implications in the intravascular compartment". Brazilian Journal of Medical and Biological Research = Revista Brasileira de Pesquisas Medicas e Biologicas. 42 (4): 305–11. doi:10.1590/s0100-879x2009000400001. PMID 19330257.
- Rosas-Díaz M, Camarillo-Cadena M, Hernández-Arana A, Ramón-Gallegos E, Medina-Navarro R (June 2015). "Antioxidant capacity and structural changes of human serum albumin from patients in advanced stages of diabetic nephropathy and the effect of the dialysis". Molecular and Cellular Biochemistry. 404 (1–2): 193–201. doi:10.1007/s11010-015-2378-2. PMID 25758354. S2CID 6718332.
- Matsuyama Y, Terawaki H, Terada T, Era S (August 2009). "Albumin thiol oxidation and serum protein carbonyl formation are progressively enhanced with advancing stages of chronic kidney disease". Clinical and Experimental Nephrology. 13 (4): 308–315. doi:10.1007/s10157-009-0161-y. PMID 19363646. S2CID 20886185.
- "Microalbumin Urine Test". WebMD.
- Chaudhury C, Mehnaz S, Robinson JM, Hayton WL, Pearl DK, Roopenian DC, Anderson CL (February 2003). "The major histocompatibility complex-related Fc receptor for IgG (FcRn) binds albumin and prolongs its lifespan". The Journal of Experimental Medicine. 197 (3): 315–22. doi:10.1084/jem.20021829. PMC 2193842. PMID 12566415.
- Merlot AM, Kalinowski DS, Richardson DR (2014). "Unraveling the mysteries of serum albumin-more than just a serum protein". Frontiers in Physiology. 5: 299. doi:10.3389/fphys.2014.00299. PMC 4129365. PMID 25161624.
Further reading
- Komatsu T, Nakagawa A, Curry S, Tsuchida E, Murata K, Nakamura N, Ohno H (September 2009). "The role of an amino acid triad at the entrance of the heme pocket in human serum albumin for O(2) and CO binding to iron protoporphyrin IX". Organic & Biomolecular Chemistry. 7 (18): 3836–41. doi:10.1039/b909794e. PMID 19707690.
- Milojevic J, Raditsis A, Melacini G (November 2009). "Human serum albumin inhibits Abeta fibrillization through a "monomer-competitor" mechanism". Biophysical Journal. 97 (9): 2585–94. Bibcode:2009BpJ....97.2585M. doi:10.1016/j.bpj.2009.08.028. PMC 2770600. PMID 19883602.
- Silva AM, Hider RC (October 2009). "Influence of non-enzymatic post-translation modifications on the ability of human serum albumin to bind iron. Implications for non-transferrin-bound iron speciation". Biochimica et Biophysica Acta. 1794 (10): 1449–58. doi:10.1016/j.bbapap.2009.06.003. PMID 19505594.
- Otosu T, Nishimoto E, Yamashita S (February 2010). "Multiple conformational state of human serum albumin around single tryptophan residue at various pH revealed by time-resolved fluorescence spectroscopy". Journal of Biochemistry. 147 (2): 191–200. doi:10.1093/jb/mvp175. PMID 19884191.
- Blindauer CA, Harvey I, Bunyan KE, Stewart AJ, Sleep D, Harrison DJ, Berezenko S, Sadler PJ (August 2009). "Structure, properties, and engineering of the major zinc binding site on human albumin". The Journal of Biological Chemistry. 284 (34): 23116–24. doi:10.1074/jbc.M109.003459. PMC 2755717. PMID 19520864.
- Juárez J, López SG, Cambón A, Taboada P, Mosquera V (July 2009). "Influence of electrostatic interactions on the fibrillation process of human serum albumin". The Journal of Physical Chemistry B. 113 (30): 10521–9. doi:10.1021/jp902224d. PMID 19572666.
- Fu BL, Guo ZJ, Tian JW, Liu ZQ, Cao W (August 2009). "[Advanced glycation end products induce expression of PAI-1 in cultured human proximal tubular epithelial cells through NADPH oxidase dependent pathway]". Xi Bao Yu Fen Zi Mian Yi Xue Za Zhi = Chinese Journal of Cellular and Molecular Immunology. 25 (8): 674–7. PMID 19664386.
- Ascenzi P, di Masi A, Coletta M, Ciaccio C, Fanali G, Nicoletti FP, Smulevich G, Fasano M (November 2009). "Ibuprofen impairs allosterically peroxynitrite isomerization by ferric human serum heme-albumin". The Journal of Biological Chemistry. 284 (45): 31006–17. doi:10.1074/jbc.M109.010736. PMC 2781501. PMID 19734142.
- Sowa ME, Bennett EJ, Gygi SP, Harper JW (July 2009). "Defining the human deubiquitinating enzyme interaction landscape". Cell. 138 (2): 389–403. doi:10.1016/j.cell.2009.04.042. PMC 2716422. PMID 19615732.
- Curry S (August 2002). "Beyond expansion: structural studies on the transport roles of human serum albumin". Vox Sanguinis. 83 Suppl 1: 315–9. doi:10.1111/j.1423-0410.2002.tb05326.x. PMID 12617161. S2CID 44482133.
- Guo S, Shi X, Yang F, Chen L, Meehan EJ, Bian C, Huang M (September 2009). "Structural basis of transport of lysophospholipids by human serum albumin". The Biochemical Journal. 423 (1): 23–30. doi:10.1042/BJ20090913. PMID 19601929.
- de Jong PE, Gansevoort RT (2009). "Focus on microalbuminuria to improve cardiac and renal protection". Nephron Clinical Practice. 111 (3): c204–10, discussion c211. doi:10.1159/000201568. PMID 19212124.
- Page TA, Kraut ND, Page PM, Baker GA, Bright FV (September 2009). "Dynamics of loop 1 of domain I in human serum albumin when dissolved in ionic liquids". The Journal of Physical Chemistry B. 113 (38): 12825–30. doi:10.1021/jp904475v. PMID 19711930.
- Roche M, Rondeau P, Singh NR, Tarnus E, Bourdon E (June 2008). "The antioxidant properties of serum albumin". FEBS Letters. 582 (13): 1783–7. doi:10.1016/j.febslet.2008.04.057. PMID 18474236. S2CID 5364683.
- Wyatt AR, Wilson MR (February 2010). "Identification of human plasma proteins as major clients for the extracellular chaperone clusterin". The Journal of Biological Chemistry. 285 (6): 3532–9. doi:10.1074/jbc.M109.079566. PMC 2823492. PMID 19996109.
- Cui FL, Yan YH, Zhang QZ, Qu GR, Du J, Yao XJ (February 2010). "A study on the interaction between 5-Methyluridine and human serum albumin using fluorescence quenching method and molecular modeling". Journal of Molecular Modeling. 16 (2): 255–62. doi:10.1007/s00894-009-0548-4. PMID 19588173. S2CID 9042021.
- Caridi G, Dagnino M, Simundic AM, Miler M, Stancic V, Campagnoli M, Galliano M, Minchiotti L (March 2010). "Albumin Benkovac (c.1175 A > G; p.Glu392Gly): a novel genetic variant of human serum albumin". Translational Research. 155 (3): 118–9. doi:10.1016/j.trsl.2009.10.001. PMID 20171595.
- Deeb O, Rosales-Hernández MC, Gómez-Castro C, Garduño-Juárez R, Correa-Basurto J (February 2010). "Exploration of human serum albumin binding sites by docking and molecular dynamics flexible ligand-protein interactions". Biopolymers. 93 (2): 161–70. doi:10.1002/bip.21314. PMID 19785033.
- Karahan SC, Koramaz I, Altun G, Uçar U, Topbaş M, Menteşe A, Kopuz M (2010). "Ischemia-modified albumin reduction after coronary bypass surgery is associated with the cardioprotective efficacy of cold-blood cardioplegia enriched with N-acetylcysteine: a preliminary study". European Surgical Research. 44 (1): 30–6. doi:10.1159/000262324. PMID 19955769. S2CID 26699371.
- Jin C, Lu L, Zhang RY, Zhang Q, Ding FH, Chen QJ, Shen WF (October 2009). "Association of serum glycated albumin, C-reactive protein and ICAM-1 levels with diffuse coronary artery disease in patients with type 2 diabetes mellitus". Clinica Chimica Acta; International Journal of Clinical Chemistry. 408 (1–2): 45–9. doi:10.1016/j.cca.2009.07.003. PMID 19615354.
External links
- Human Albumin structure in the Protein data bank
- Human Albumin information in the Swis-Prot/TrEMBL database
- Human Serum Albumin on the Human Protein Reference Database
- Albumin binding prediction
- Albumin at Lab Tests Online
- Albumin: analyte monograph from the Association for Clinical Biochemistry and Laboratory Medicine
- Overview of all the structural information available in the PDB for UniProt: P02768 (Serum albumin) at the PDBe-KB.
PDB gallery | |
|---|---|
|








































{kind=link}