Knee arthritis
Arthritis of the knee is typically a particularly debilitating form of arthritis.[1] The knee may become affected by almost any form of arthritis.[2]
| Knee arthritis | |
|---|---|
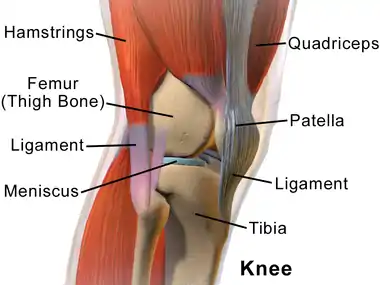 | |
| Human knee | |
| Specialty | Rheumatology |
The word arthritis refers to inflammation of the joints.[3][4] Types of arthritis include those related to wear and tear of cartilage, such as osteoarthritis, to those associated with inflammation resulting from an overactive immune system (such as rheumatoid arthritis).[5][6]
Causes
It is not always certain why arthritis of the knee develops. The knee may become affected by almost any form of arthritis, including those related to mechanical damage of the structures of the knee (osteoarthritis, and post-traumatic arthritis), various autoimmune forms of arthritis (including; rheumatoid arthritis, juvenile arthritis, and SLE-related arthritis, psoriatic arthritis, and ankylosing spondylitis), arthritis due to infectious causes (including Lyme disease-related arthritis), gouty arthritis, or reactive arthritis.[2][1]
Osteoarthritis of the knee
The knee is one of the joints most commonly affected by osteoarthritis.[2] Cartilage in the knee may begin to break down after sustained stress, leaving the bones of the knee rubbing against each other and resulting in osteoarthritis.[7] Nearly a third of US citizens are affected by osteoarthritis of the knee by age 70.[8]
Obesity is a known and very significant risk factor for the development of osteoarthritis.[9] Risk increases proportionally to body weight. Obesity contributes to OA development, not only by increasing the mechanical stress exerted upon the knees when standing, but also leads to increased production of compounds that may cause joint inflammation.[7]
Parity is associated with an increased risk of knee OA and likelihood of knee replacement. The risk increases in proportion to the number of children the woman has birthed. This may be due to weight gain after pregnancy, or increased body weight and consequent joint stress during pregnancy.[10]
Flat feet are a significant risk factor for the development of osteoarthritis.[11] Additionally, structural deformities, advanced age, female sex, past joint trauma, genetic predisposition, and certain at-risk occupations may all contribute to the development of osteoarthritis in general.[7]
Lyme disease-related arthritis of the knee
The knee is often the first joint affected in Lyme disease.[2]
Systemic lupus erythematosus
Arthritis is a common symptom of SLE. Arthritis is often symmetric and more often involves small joints. Though almost any joint may be affected, the knees and joints of the hands are most often involved in SLE. In larger joints (including the knee), avascular necrosis is a possible complication, leading to further pain and disability.[12]
Reactive arthritis
Reactive arthritis often presents with lower limb oligoarthritis, including that of the knee.[13]
Gout
Arthritis of a single joint of the lower extremities with rapid onset is highly suggestive of gouty arthritis.[14] The knee may sometimes be affected. In cases of gouty arthritis of the knee, skin symptoms occur less often, however pain and swelling may be particularly intense.[15]
Rheumatoid arthritis
RA most often first manifests as inflammation of particular finger or toe joints, however, pain and swelling of larger joints, including the knees, may also be the first sign.[16]
Diagnosis
Osteoarthritis of the knee
Diagnosis of knee osteoarthritis often entails a physical examination, assessment of symptoms and the patient's medical history, but may also involve medical imaging and blood tests.[1] Persistent knee pain, limited morning stiffness and reduced function, crepitus, restricted movement, and bony enlargement appear to be the most useful indications of knee osteoarthritis for diagnosis.[17]
Standardized medical questionnaires like the Knee injury and Osteoarthritis Outcome Score (KOOS)[18] and short form KOOS JR.[19] or the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC)[20] can also be used to diagnose and monitor progression of knee osteoarthritis.
Management
A physician will recommend a treatment regimen based upon the severity of symptoms. General recommendations for the management of knee arthritis may include avoiding activities that aggravate the condition, and applying cold or warm packs and using ointments and creams to relieve symptoms.[1]
Pharmaceutical
Pharmaceutical management is usually dependent upon the nature of the underlying condition causing arthritis. Over-the-counter medications like acetaminophen (paracetamol), and ibuprofen, naproxen, and other NSAIDs are often used as first-line medical treatments for pain relief and/or managing inflammation. Corticosteroids may be injected directly into the joint cavity to provide more significant relief from inflammation, swelling, and pain. Other medications used in management of arthritis of the knee include; disease-modifying antirheumatic drugs, biopharmaceuticals, viscosupplementation (including hyaluronic acid injections), and glucosamine and chondroitin sulphate.[1]
Hyaluronic acid is normally present in joints (including the knee), acting as lubricant and providing shock absorption, among other functions. In osteoarthritis, there is a loss of articular hyaluronic acid activity, likely contributing to pain and stiffness associated with the condition. Hyaluronic acid injections are an FDA-approved treatment for osteoarthritis of the knee, and are sometimes also used for other joints. However, the merits of HA injections are still disputed. HA injections are indicated when other medications fail to offer adequate symptom relief. Symptom relief associated with HA injections may last up to 2 years after an injection. HA injections appear to offer significant pain relief to some patients, while others may see no benefits at all.[21][22][23][24] In severe osteoarthritis without much cartilage, the benefits of hyaluronic are not observed.
Orthotics
Supportive devices like knee braces can be used for symptom relief in osteoarthritis of the knee.[25][26] Knee braces may however result in discomfort, skin irritation, swelling, and may not provide benefits to all.[26] Using a cane, shock-absorbent footwear and inserts, elastic bandages, and knee sleeves may also be helpful for managing arthritis symptoms. Braces may be especially effective when only one knee is affected.[1] Shoe insoles that are fitted to correct flat feet provide significant relief to those with severely flat feet.[27] However, it has been found that insoles used to correct medial knee osteoarthritis (the more common form) may not offer much pain relief.[28][29]
Body weight
Obesity is a known and very significant risk factor for the development of osteoarthritis.[9] Furthermore, losing weight reduces mechanical stress acting upon the knees when standing, possibly reducing pain and improving function in knee osteoarthritis.[26][1] However, it is necessary to ascertain whether the patient is actually overweight before committing to weight loss as a management technique.[9]
Exercise
Exercises can help increase range of motion and flexibility as well as help strengthen the muscles in the leg.[30] Physical therapy and exercise are often effective in reducing pain and improving function. Compared to the patient-education program, pain and function showed improvement after eight weeks of aquatic exercise, and after twelve weeks it showed improvement in the function actiites.[31] Inclusion of isokinetic quadriceps and hamstring strengthening exercises into the rehabilitation packages for the patients with knee osteoarthritis may also enhance the high-quality of life and make a contribution to the decreased hazard of fall.[32] land-based exercises that focus on hip abductor shows improvement related to performance and function in women with symptomatic knee osteoarthritis.[33] A Cochrane review could not conclude whether high-intensity exercises provide better results than low-intensity exercises.[34]
Surgical
Surgical intervention may be undertaken if no other management technique yields adequate relief. Surgical procedures may entail an arthroscopy (seldom used for sole osteoarthritis), osteotomy (performed only for unilateral early-stage osteoarthritis), or arthroplasty.[1]
Knee replacement is the most definitive treatment for osteoarthritis-related symptoms and disability.[10][7] It is a type of arthroplasty, and may involve either a partial or total replacement with a prosthesis.[1]
Alternative medicine
Alternative medicine interventions undertaken for pain relief in arthritis of the knee include acupuncture, and magnetic pulse therapy.[1]
Notes
- "Arthritis of the Knee - OrthoInfo - AAOS". www.orthoinfo.org. Retrieved 2018-12-23.
- "Osteoarthritis Knee | Arthritis In Knee | Knee Diseases". arthritis.org. Retrieved 2018-12-23.
- MHC report Archived 2014-01-27 at the Wayback Machine, The arthritis Association
- pmhdev. "Arthritis - National Library of Medicine". PubMed Health. Retrieved 2017-12-21.
- Arthritis Causes, Symptoms, Diagnosis and Treatment Information on MedicineNet.com, Retrieved on 2010-01-22.
- "Knee Arthritis". North Yorkshire Orthopaedic Specialists. Retrieved 15 January 2013.
- "Osteoarthritis - Symptoms and causes". Mayo Clinic. Retrieved 2018-12-23.
- Watson S (2013-08-21). "Insoles no help for knee osteoarthritis". Harvard Health Blog. Retrieved 2018-12-23.
- "Osteoarthritis : Role of Body Weight in Osteoarthritis - Weight Management". Arthritis Information. Retrieved 2018-12-23.
- Wise BL, Niu J, Zhang Y, Felson DT, Bradley LA, Segal N, Keysor J, Nevitt M, Lane NE (December 2013). "The association of parity with osteoarthritis and knee replacement in the multicenter osteoarthritis study". Osteoarthritis and Cartilage. 21 (12): 1849–54. doi:10.1016/j.joca.2013.08.025. PMC 3855897. PMID 24029601.
- Gross KD, Felson DT, Niu J, Hunter DJ, Guermazi A, Roemer FW, Dufour AB, Gensure RH, Hannan MT (July 2011). "Association of flat feet with knee pain and cartilage damage in older adults". Arthritis Care & Research. 63 (7): 937–44. doi:10.1002/acr.20431. PMC 3087845. PMID 21717597.
- Grossman JM (August 2009). "Lupus arthritis". Best Practice & Research. Clinical Rheumatology. 23 (4): 495–506. doi:10.1016/j.berh.2009.04.003. PMID 19591780.
- Hamdulay SS, Glynne SJ, Keat A (July 2006). "When is arthritis reactive?". Postgraduate Medical Journal. 82 (969): 446–53. doi:10.1136/pgmj.2005.044057. PMC 2563769. PMID 16822921.
- Tausche AK, Aringer M (November 2016). "[Gouty arthritis]". Zeitschrift für Rheumatologie. 75 (9): 885–898. doi:10.1007/s00393-016-0206-z. PMID 27730304.
- Ragab G, Elshahaly M, Bardin T (September 2017). "Gout: An old disease in new perspective - A review". Journal of Advanced Research. 8 (5): 495–511. doi:10.1016/j.jare.2017.04.008. PMC 5512152. PMID 28748116.
- "Rheumatoid arthritis: Overview". Informed Health Online. Cologne, Germany: Institute for Quality and Efficiency in Health Care (IQWiG). 2016-08-11.
- Zhang W, Doherty M, Peat G, Bierma-Zeinstra MA, Arden NK, Bresnihan B, et al. (2010). "EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis". Ann Rheum Dis. 69 (3): 483–9. doi:10.1136/ard.2009.113100. PMID 19762361. S2CID 12319076.
- "KOOS survey score description and calculator – orthotoolkit". Retrieved January 1, 2018.
- "KOOS Jr. survey score description and calculator – orthotoolkit". Retrieved January 1, 2018.
- McConnell S, Kolopack P, Davis AM (October 2001). "The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC): a review of its utility and measurement properties". Arthritis and Rheumatism. 45 (5): 453–61. doi:10.1002/1529-0131(200110)45:5<453::AID-ART365>3.0.CO;2-W. PMID 11642645.
- "Hyaluronic Acid Injections for Osteoarthritis". arthritis.org. Retrieved 2018-12-23.
- "Hyaluronic Acid (Injection Route) Description and Brand Names - Mayo Clinic". www.mayoclinic.org. Retrieved 2018-12-23.
- Bowman S, Awad ME, Hamrick MW, Hunter M, Fulzele S (February 2018). "Recent advances in hyaluronic acid based therapy for osteoarthritis". Clinical and Translational Medicine. 7 (1): 6. doi:10.1186/s40169-017-0180-3. PMC 5814393. PMID 29450666.
- Bowman EN, Hallock JD, Throckmorton TW, Azar FM (April 2018). "Hyaluronic acid injections for osteoarthritis of the knee: predictors of successful treatment". International Orthopaedics. 42 (4): 733–740. doi:10.1007/s00264-017-3731-8. PMID 29299652. S2CID 4379086.
- Phillips S, Li CS, Phillips M, Bischoff M, Ali P, Chahal J, Snider M, Bhandari M (June 2016). "Treatment of Osteoarthritis of the Knee with Bracing: A Scoping Review". Orthopedic Reviews. 8 (2): 6256. doi:10.4081/or.2016.6256. PMC 4933815. PMID 27433297.
- "Knee braces for osteoarthritis - Mayo Clinic". www.mayoclinic.org. Retrieved 2018-12-23.
- "Athletic shoes for knee osteoarthritis: The best walking and running options". Medical News Today. Retrieved 2018-12-23.
- Watson S (2013-08-21). "Insoles no help for knee osteoarthritis". Harvard Health Blog. Retrieved 2018-12-23.
- Parkes MJ, Maricar N, Lunt M, LaValley MP, Jones RK, Segal NA, Takahashi-Narita K, Felson DT (August 2013). "Lateral wedge insoles as a conservative treatment for pain in patients with medial knee osteoarthritis: a meta-analysis". JAMA. 310 (7): 722–30. doi:10.1001/jama.2013.243229. PMC 4458141. PMID 23989797.
- Arthritis of the Knee - American Academy of Orthopaetic Surgeons, Retrieved on 2010-01-22.
- Taglietti, Marcelo; Facci, Ligia Maria; Trelha, Celita Salmaso; de Melo, Fernanda Cristiane; da Silva, Daniela Wosiack; Sawczuk, Geovane; Ruivo, Thamires Marques; de Souza, Thaisley Barbosa; Sforza, Chiarella; Cardoso, Jefferson Rosa (June 2018). "Effectiveness of aquatic exercises compared to patient-education on health status in individuals with knee osteoarthritis: a randomized controlled trial". Clinical Rehabilitation. 32 (6): 766–776. doi:10.1177/0269215517754240. hdl:2434/548022. ISSN 1477-0873. PMID 29417831. S2CID 3431729.
- Gezginaslan, Ömer; Öztürk, Erhan Arif; Cengiz, Mustafa; Mirzaoğlu, Tacettin; Çakcı, Fatma Aytül (December 2018). "Effects of isokinetic muscle strengthening on balance, proprioception, and physical function in bilateral knee osteoarthritis patients with moderate fall risk". Turkish Journal of Physical Medicine and Rehabilitation. 64 (4): 353–361. doi:10.5606/tftrd.2018.2422. ISSN 2587-1250. PMC 6648029. PMID 31453533.
- Wang, Jianxiong; Xie, Yujie; Wang, Li; Lei, Lei; Liao, Peng; Wang, ShiQi; Gao, YaQian; Chen, Yu; Xu, Fangyuan; Zhang, Chi (2020). "Hip abductor strength-based exercise therapy in treating women with moderate-to-severe knee osteoarthritis: a randomized controlled trial". Clinical Rehabilitation. 34 (2): 160–169. doi:10.1177/0269215519875328. ISSN 1477-0873. PMID 31505954. S2CID 202557153.
- Regnaux JP, Lefevre-Colau MM, Trinquart L, Nguyen C, Boutron I, Brosseau L, Ravaud P (October 2015). "High-intensity versus low-intensity physical activity or exercise in people with hip or knee osteoarthritis". The Cochrane Database of Systematic Reviews (10): CD010203. doi:10.1002/14651858.CD010203.pub2. PMID 26513223.