Lobotomy
A lobotomy, or leucotomy, is a form of psychosurgery, a neurosurgical treatment of a mental disorder that involves severing connections in the brain's prefrontal cortex.[2] Most of the connections to and from the prefrontal cortex, the anterior part of the frontal lobes of the brain, are severed. It was used for mental disorders and occasionally other conditions as a mainstream procedure in some Western countries for more than two decades, despite general recognition of frequent and serious side-effects. Some patients improved in some ways after the operation, but complications and impairments – sometimes severe – were frequent. The procedure was controversial from its initial use, in part due to the balance between benefits and risks. Today, the lobotomy has become a disparaged procedure, a byword for medical barbarism and an exemplary instance of the medical trampling of patients' rights.[3]
| Lobotomy | |
|---|---|
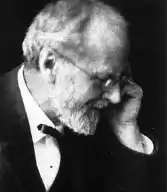
 "Dr. Walter Freeman, left, and Dr. James W. Watts study an X ray before a psychosurgical operation. Psychosurgery is cutting into the brain to form new patterns and rid a patient of delusions, obsessions, nervous tensions and the like." Waldemar Kaempffert, "Turning the Mind Inside Out", Saturday Evening Post, 24 May 1941.[1] | |
| Other names | Leukotomy, leucotomy |
| ICD-9-CM | 01.32 |
| MeSH | D011612 |
The originator of the procedure, Portuguese neurologist António Egas Moniz, shared the Nobel Prize for Physiology or Medicine of 1949 for the "discovery of the therapeutic value of leucotomy in certain psychoses",[n 1] although the awarding of the prize has been subject to controversy.[5]
The use of the procedure increased dramatically from the early 1940s and into the 1950s; by 1951, almost 20,000 lobotomies had been performed in the United States and proportionally more in the United Kingdom.[6] The majority of lobotomies were performed on women; a 1951 study of American hospitals found nearly 60% of lobotomy patients were women; limited data show 74% of lobotomies in Ontario from 1948–1952 were performed on women.[7][8][9] From the 1950s onward, lobotomy began to be abandoned,[10] first in the Soviet Union[11] and Europe.[12] The term is derived from Greek: λοβός lobos "lobe" and τομή tomē "cut, slice".
Effects
— `Comments added to the consent form for a lobotomy operation on "Helaine Strauss", the pseudonym used for "a patient at an elite private hospital".[13]
Historically, patients of lobotomy were, immediately following surgery, often stuporous, confused, and incontinent. Some developed an enormous appetite and gained considerable weight. Seizures were another common complication of surgery. Emphasis was put on the training of patients in the weeks and months following surgery.[14]
The purpose of the operation was to reduce the symptoms of mental disorders, and it was recognized that this was accomplished at the expense of a person's personality and intellect. British psychiatrist Maurice Partridge, who conducted a follow-up study of 300 patients, said that the treatment achieved its effects by "reducing the complexity of psychic life". Following the operation, spontaneity, responsiveness, self-awareness and self-control were reduced. The activity was replaced by inertia, and people were left emotionally blunted and restricted in their intellectual range.[15]
The consequences of the operation have been described as "mixed".[16] Some patients died as a result of the operation and others later committed suicide. Some were left severely brain-damaged. Others were able to leave the hospital, or became more manageable within the hospital.[16] A few people managed to return to responsible work, while at the other extreme, people were left with severe and disabling impairments.[17] Most people fell into an intermediate group, left with some improvement of their symptoms but also with emotional and intellectual deficits to which they made a better or worse adjustment.[17] On average, there was a mortality-rate of approximately 5% during the 1940s.[17]
The lobotomy-procedure could have severe negative effects on a patient's personality and ability to function independently.[18] Lobotomy-patients often show a marked reduction in initiative and inhibition.[19] They may also exhibit difficulty putting themselves in the position of others because of decreased cognition and detachment from society.[20]
Walter Freeman coined the term "surgically induced childhood" and used it constantly to refer to the results of lobotomy. The operation left people with an "infantile personality"; a period of maturation would then, according to Freeman, lead to recovery. In an unpublished memoir, he described how the "personality of the patient was changed in some way in the hope of rendering him more amenable to the social pressures under which he is supposed to exist." He described one 29-year-old woman as being, following lobotomy, a "smiling, lazy and satisfactory patient with the personality of an oyster" who could not remember Freeman's name and endlessly poured coffee from an empty pot. When her parents had difficulty dealing with her behavior, Freeman advised a system of rewards (ice-cream) and punishment (smacks).[21]
History

In the early 20th century, the number of patients residing in mental hospitals increased significantly[n 2] while little in the way of effective medical treatment was available.[n 3][27] Lobotomy was one of a series of radical and invasive physical therapies developed in Europe at this time that signaled a break with a psychiatric culture of therapeutic nihilism that had prevailed since the late nineteenth-century.[28] The new "heroic" physical therapies devised during this experimental era,[29] including malarial therapy for general paresis of the insane (1917),[30] deep sleep therapy (1920), insulin shock therapy (1933), cardiazol shock therapy (1934), and electroconvulsive therapy (1938),[31] helped to imbue the then therapeutically moribund and demoralised psychiatric profession with a renewed sense of optimism in the curability of insanity and the potency of their craft.[32] The success of the shock therapies, despite the considerable risk they posed to patients, also helped to accommodate psychiatrists to ever more drastic forms of medical intervention, including lobotomy.[29]
The clinician–historian Joel Braslow argues that from malarial therapy onward to lobotomy, physical psychiatric therapies "spiral closer and closer to the interior of the brain" with this organ increasingly taking "center stage as a source of disease and site of cure".[33] For Roy Porter, once the doyen of medical history,[34] the often violent and invasive psychiatric interventions developed during the 1930s and 1940s are indicative of both the well-intentioned desire of psychiatrists to find some medical means of alleviating the suffering of the vast number of patients then in psychiatric hospitals and also the relative lack of social power of those same patients to resist the increasingly radical and even reckless interventions of asylum doctors.[35] Many doctors, patients and family-members of the period believed that despite potentially catastrophic consequences, the results of lobotomy were seemingly positive in many instances or, at least, they were deemed as such when measured next to the apparent alternative of long-term institutionalisation. Lobotomy has always been controversial, but for a period of the medical mainstream, it was even feted and regarded as a legitimate last-resort remedy for categories of patients who were otherwise regarded as hopeless.[36] Today, lobotomy has become a disparaged procedure, a byword for medical barbarism and an exemplary instance of the medical trampling of patients' rights.[3]
Early psychosurgery
Before the 1930s, individual doctors had infrequently experimented with novel surgical operations on the brains of those deemed insane. Most notably in 1888, the Swiss psychiatrist Gottlieb Burckhardt initiated what is commonly considered the first systematic attempt at modern human psychosurgery.[37] He operated on six patients under his care at the Swiss Préfargier Asylum, removing sections of their cerebral cortex. Burckhardt's decision to operate was informed by three pervasive views on the nature of mental illness and its relationship to the brain. First, the belief that mental illness was organic in nature, and reflected an underlying brain-pathology; next, that the nervous-system was organized according to an associationist model comprising an input or afferent system (a sensory center), a connecting system where information-processing took place (an association center), and an output or efferent system (a motor center); and, finally, a modular conception of the brain whereby discrete mental faculties were connected to specific regions of the brain.[38] Burckhardt's hypothesis was that by deliberately creating lesions in regions of the brain identified as association centers a transformation in behavior might ensue.[38] According to his model, those mentally ill might experience "excitations abnormal in quality, quantity and intensity" in the sensory regions of the brain and this abnormal stimulation would then be transmitted to the motor regions giving rise to mental pathology.[39] He reasoned, however, that removing material from either of the sensory or motor zones could give rise to "grave functional disturbance".[39] Instead, by targeting the association-centers and creating a "ditch" around the motor region of the temporal lobe, he hoped to break their lines of communication and thus alleviate both mental symptoms and the experience of mental distress.[40]

Intending to ameliorate symptoms in those with violent and intractable conditions rather than effect a cure,[41] Burckhardt began operating on patients in December 1888,[42] but both his surgical methods and instruments were crude and the results of the procedure were mixed at best.[39] He operated on six patients in total and, according to his own assessment, two experienced no change, two patients became quieter, one patient experienced epileptic convulsions and died a few days after the operation, and one patient improved.[n 4] Complications included motor weakness, epilepsy, sensory aphasia and "word deafness".[44] Claiming a success rate of 50 percent,[45] he presented the results at the Berlin Medical Congress and published a report, but the response from his medical peers was hostile and he did no further operations.[46]
In 1912, two physicians based in Saint Petersburg, the leading Russian neurologist Vladimir Bekhterev and his younger Estonian colleague, the neurosurgeon Ludvig Puusepp, published a paper reviewing a range of surgical interventions that had been performed on the mentally ill.[47] While generally treating these endeavours favorably, in their consideration of psychosurgery they reserved unremitting scorn for Burckhardt's surgical experiments of 1888 and opined that it was extraordinary that a trained medical doctor could undertake such an unsound procedure.[48]
We have quoted this data to show not only how groundless but also how dangerous these operations were. We are unable to explain how their author, holder of a degree in medicine, could bring himself to carry them out ...[49]
The authors neglected to mention, however, that in 1910 Puusepp himself had performed surgery on the brains of three mentally ill patients,[n 5][51] sectioning the cortex between the frontal and parietal lobes.[52] He had abandoned these attempts because of unsatisfactory results and this experience probably inspired the invective that was directed at Burckhardt in the 1912 article.[48] By 1937, Puusepp, despite his earlier criticism of Burckhardt, was increasingly persuaded that psychosurgery could be a valid medical intervention for the mentally disturbed.[n 6][54] In the late 1930s, he worked closely with the neurosurgical team of the Racconigi Hospital near Turin to establish it as an early and influential centre for the adoption of leucotomy in Italy.[55]
Development

Leucotomy was first undertaken in 1935 under the direction of the Portuguese neurologist (and inventor of the term psychosurgery) António Egas Moniz.[n 7][59] First developing an interest in psychiatric conditions and their somatic treatment in the early 1930s,[60] Moniz apparently conceived a new opportunity for recognition in the development of a surgical intervention on the brain as a treatment for mental illness.[41]
Frontal lobes
The source of inspiration for Moniz's decision to hazard psychosurgery has been clouded by contradictory statements made on the subject by Moniz and others, both contemporaneously and retrospectively.[61] The traditional narrative addresses the question of why Moniz targeted the frontal lobes by way of reference to the work of the Yale neuroscientist John Fulton and, most dramatically, to a presentation Fulton made with his junior colleague Carlyle Jacobsen at the Second International Congress of Neurology held in London in 1935.[62] Fulton's primary area of research was on the cortical function of primates and he had established America's first primate neurophysiology laboratory at Yale in the early 1930s.[63] At the 1935 Congress, with Moniz in attendance,[n 8] Fulton and Jacobsen presented two chimpanzees, named Becky and Lucy, who had had frontal lobectomies and subsequent changes in behaviour and intellectual function.[64] According to Fulton's account of the congress, they explained that before surgery, both animals, and especially Becky, the more emotional of the two, exhibited "frustrational behaviour" – that is, have tantrums that could include rolling on the floor and defecating – if, because of their poor performance in a set of experimental tasks, they were not rewarded.[65] Following the surgical removal of their frontal lobes, the behaviour of both primates changed markedly and Becky was pacified to such a degree that Jacobsen apparently stated it was as if she had joined a "happiness cult".[64] During the question and answer section of the paper, Moniz, it is alleged, "startled" Fulton by inquiring if this procedure might be extended to human subjects suffering from mental illness. Fulton stated that he replied that while possible in theory it was surely "too formidable" an intervention for use on humans.[66]
Moniz began his experiments with leucotomy just three months after the congress had reinforced the apparent cause-and-effect relationship between the Fulton and Jacobsen presentation and the Portuguese neurologist's resolve to operate on the frontal lobes.[67] As the author of this account Fulton, who has sometimes been claimed as the father of lobotomy, was later able to record that the technique had its true origination in his laboratory.[68] Endorsing this version of events, in 1949, the Harvard neurologist Stanley Cobb remarked during his presidential address to the American Neurological Association that "seldom in the history of medicine has a laboratory observation been so quickly and dramatically translated into a therapeutic procedure". Fulton's report, penned ten years after the events described, is, however, without corroboration in the historical record and bears little resemblance to an earlier unpublished account he wrote of the congress. In this previous narrative he mentioned an incidental, private exchange with Moniz, but it is likely that the official version of their public conversation he promulgated is without foundation.[69] In fact, Moniz stated that he had conceived of the operation some time before his journey to London in 1935, having told in confidence his junior colleague, the young neurosurgeon Pedro Almeida Lima, as early as 1933 of his psychosurgical idea.[70] The traditional account exaggerates the importance of Fulton and Jacobsen to Moniz's decision to initiate frontal lobe surgery, and omits the fact that a detailed body of neurological research that emerged at this time suggested to Moniz and other neurologists and neurosurgeons that surgery on this part of the brain might yield significant personality changes in the mentally ill.[71]
As the frontal lobes had been the object of scientific inquiry and speculation since the late 19th century, Fulton's contribution, while it may have functioned as source of intellectual support, is of itself unnecessary and inadequate as an explanation of Moniz's resolution to operate on this section of the brain.[72] Under an evolutionary and hierarchical model of brain development it had been hypothesized that those regions associated with more recent development, such as the mammalian brain and, most especially, the frontal lobes, were responsible for more complex cognitive functions.[73] However, this theoretical formulation found little laboratory support, as 19th-century experimentation found no significant change in animal behaviour following surgical removal or electrical stimulation of the frontal lobes.[73] This picture of the so-called "silent lobe" changed in the period after World War I with the production of clinical reports of ex-servicemen who had suffered brain trauma. The refinement of neurosurgical techniques also facilitated increasing attempts to remove brain tumours, treat focal epilepsy in humans and led to more precise experimental neurosurgery in animal studies.[73] Cases were reported where mental symptoms were alleviated following the surgical removal of diseased or damaged brain tissue.[52] The accumulation of medical case studies on behavioural changes following damage to the frontal lobes led to the formulation of the concept of Witzelsucht, which designated a neurological condition characterised by a certain hilarity and childishness in the afflicted.[73] The picture of frontal lobe function that emerged from these studies was complicated by the observation that neurological deficits attendant on damage to a single lobe might be compensated for if the opposite lobe remained intact.[73] In 1922, the Italian neurologist Leonardo Bianchi published a detailed report on the results of bilateral lobectomies in animals that supported the contention that the frontal lobes were both integral to intellectual function and that their removal led to the disintegration of the subject's personality.[74] This work, while influential, was not without its critics due to deficiencies in experimental design.[73]
The first bilateral lobectomy of a human subject was performed by the American neurosurgeon Walter Dandy in 1930.[n 9][75] The neurologist Richard Brickner reported on this case in 1932,[76] relating that the recipient, known as "Patient A", while experiencing a blunting of affect, had suffered no apparent decrease in intellectual function and seemed, at least to the casual observer, perfectly normal.[77] Brickner concluded from this evidence that "the frontal lobes are not 'centers' for the intellect".[78] These clinical results were replicated in a similar operation undertaken in 1934 by the neurosurgeon Roy Glenwood Spurling and reported on by the neuropsychiatrist Spafford Ackerly.[79] By the mid-1930s, interest in the function of the frontal lobes reached a high-water mark. This was reflected in the 1935 neurological congress in London, which hosted[79] as part of its deliberations,[79] "a remarkable symposium ... on the functions of the frontal lobes".[80] The panel was chaired by Henri Claude, a French neuropsychiatrist, who commenced the session by reviewing the state of research on the frontal lobes, and concluded that "altering the frontal lobes profoundly modifies the personality of subjects".[78] This parallel symposium contained numerous papers by neurologists, neurosurgeons and psychologists; amongst these was one by Brickner, which impressed Moniz greatly,[77] that again detailed the case of "Patient A".[79] Fulton and Jacobsen's paper, presented in another session of the conference on experimental physiology, was notable in linking animal and human studies on the function of the frontal lobes.[79] Thus, at the time of the 1935 Congress, Moniz had available to him an increasing body of research on the role of the frontal lobes that extended well beyond the observations of Fulton and Jacobsen.[81]
Nor was Moniz the only medical practitioner in the 1930s to have contemplated procedures directly targeting the frontal lobes.[82] Although ultimately discounting brain surgery as carrying too much risk, physicians and neurologists such as William Mayo, Thierry de Martel, Richard Brickner, and Leo Davidoff had, before 1935, entertained the proposition.[n 10][84] Inspired by Julius Wagner-Jauregg's development of malarial therapy for the treatment of general paresis of the insane, the French physician Maurice Ducosté reported in 1932 that he had injected 5 ml of malarial blood directly into the frontal lobes of over 100 paretic patients through holes drilled into the skull.[82] He claimed that the injected paretics showed signs of "uncontestable mental and physical amelioration" and that the results for psychotic patients undergoing the procedure was also "encouraging".[85] The experimental injection of fever-inducing malarial blood into the frontal lobes was also replicated during the 1930s in the work of Ettore Mariotti and M. Sciutti in Italy and Ferdière Coulloudon in France.[86] In Switzerland, almost simultaneously with the commencement of Moniz's leucotomy programme, the neurosurgeon François Ody had removed the entire right frontal lobe of a catatonic schizophrenic patient.[87] In Romania, Ody's procedure was adopted by Dimitri Bagdasar and Constantinesco working out of the Central Hospital in Bucharest.[83] Ody, who delayed publishing his own results for several years, later rebuked Moniz for claiming to have cured patients through leucotomy without waiting to determine if there had been a "lasting remission".[88]
Neurological model
The theoretical underpinnings of Moniz's psychosurgery were largely commensurate with the nineteenth-century ones that had informed Burckhardt's decision to excise matter from the brains of his patients. Although in his later writings Moniz referenced both the neuron theory of Ramón y Cajal and the conditioned reflex of Ivan Pavlov,[89] in essence he simply interpreted this new neurological research in terms of the old psychological theory of associationism.[61] He differed significantly from Burckhardt, however in that he did not think there was any organic pathology in the brains of the mentally ill, but rather that their neural pathways were caught in fixed and destructive circuits leading to "predominant, obsessive ideas".[n 11][91] As Moniz wrote in 1936:
[The] mental troubles must have ... a relation with the formation of cellulo-connective groupings, which become more or less fixed. The cellular bodies may remain altogether normal, their cylinders will not have any anatomical alterations; but their multiple liaisons, very variable in normal people, may have arrangements more or less fixed, which will have a relation with persistent ideas and deliria in certain morbid psychic states.[92]
For Moniz, "to cure these patients," it was necessary to "destroy the more or less fixed arrangements of cellular connections that exist in the brain, and particularly those which are related to the frontal lobes",[93] thus removing their fixed pathological brain circuits. Moniz believed the brain would functionally adapt to such injury.[94] Unlike the position adopted by Burckhardt, it was unfalsifiable according to the knowledge and technology of the time as the absence of a known correlation between physical brain pathology and mental illness could not disprove his thesis.[95]
First leucotomies
Egas Moniz (1937)[96]
On 12 November 1935 at the Hospital Santa Marta in Lisbon, Moniz initiated the first of a series of operations on the brains of the mentally ill.[97] The initial patients selected for the operation were provided by the medical director of Lisbon's Miguel Bombarda Mental Hospital, José de Matos Sobral Cid.[98] As Moniz lacked training in neurosurgery and his hands were crippled from gout, the procedure was performed under general anaesthetic by Pedro Almeida Lima, who had previously assisted Moniz with his research on cerebral angiography.[n 12][100] The intention was to remove some of the long fibres that connected the frontal lobes to other major brain centres.[101] To this end, it was decided that Lima would trephine into the side of the skull and then inject ethanol into the "subcortical white matter of the prefrontal area"[96] so as to destroy the connecting fibres, or association tracts,[102] and create what Moniz termed a "frontal barrier".[n 13][103] After the first operation was complete, Moniz considered it a success and, observing that the patient's depression had been relieved, he declared her "cured" although she was never, in fact, discharged from the mental hospital.[104] Moniz and Lima persisted with this method of injecting alcohol into the frontal lobes for the next seven patients but, after having to inject some patients on numerous occasions to elicit what they considered a favourable result, they modified the means by which they would section the frontal lobes.[104] For the ninth patient they introduced a surgical instrument called a leucotome; this was a cannula that was 11 centimetres (4.3 in) in length and 2 centimetres (0.79 in) in diameter. It had a retractable wire loop at one end that, when rotated, produced a 1 centimetre (0.39 in) diameter circular lesion in the white matter of the frontal lobe.[105] Typically, six lesions were cut into each lobe, but, if they were dissatisfied by the results, Lima might perform several procedures, each producing multiple lesions in the left and right frontal lobes.[104]
By the conclusion of this first run of leucotomies in February 1936, Moniz and Lima had operated on twenty patients with an average period of one week between each procedure; Moniz published his findings with great haste in March of the same year.[106] The patients were aged between 27 and 62 years of age; twelve were female and eight were male. Nine of the patients were diagnosed as suffering from depression, six from schizophrenia, two from panic disorder, and one each from mania, catatonia and manic-depression with the most prominent symptoms being anxiety and agitation. The duration of the illness before the procedure varied from as little as four weeks to as much as 22 years, although all but four had been ill for at least one year.[107] Patients were normally operated on the day they arrived at Moniz's clinic and returned within ten days to the Miguel Bombarda Mental Hospital.[108] A perfunctory post-operative follow-up assessment took place anywhere from one to ten weeks following surgery.[109] Complications were observed in each of the leucotomy patients and included: "increased temperature, vomiting, bladder and bowel incontinence, diarrhea, and ocular affections such as ptosis and nystagmus, as well as psychological effects such as apathy, akinesia, lethargy, timing and local disorientation, kleptomania, and abnormal sensations of hunger".[110] Moniz asserted that these effects were transitory and,[110] according to his published assessment, the outcome for these first twenty patients was that 35%, or seven cases, improved significantly, another 35% were somewhat improved and the remaining 30% (six cases) were unchanged. There were no deaths and he did not consider that any patients had deteriorated following leucotomy.[111]
Reception
Moniz rapidly disseminated his results through articles in the medical press and a monograph in 1936.[103] Initially, however, the medical community appeared hostile to the new procedure.[112] On 26 July 1936, one of his assistants, Diogo Furtado, gave a presentation at the Parisian meeting of the Société Médico-Psychologique on the results of the second cohort of patients leucotomised by Lima.[103] Sobral Cid, who had supplied Moniz with the first set of patients for leucotomy from his own hospital in Lisbon, attended the meeting and denounced the technique,[112] declaring that the patients who had been returned to his care post-operatively were "diminished" and had suffered a "degradation of personality".[113] He also claimed that the changes Moniz observed in patients were more properly attributed to shock and brain trauma, and he derided the theoretical architecture that Moniz had constructed to support the new procedure as "cerebral mythology."[113] At the same meeting the Parisian psychiatrist, Paul Courbon, stated he could not endorse a surgical technique that was solely supported by theoretical considerations rather than clinical observations.[114] He also opined that the mutilation of an organ could not improve its function and that such cerebral wounds as were occasioned by leucotomy risked the later development of meningitis, epilepsy and brain abscesses.[115] Nonetheless, Moniz's reported successful surgical treatment of 14 out of 20 patients led to the rapid adoption of the procedure on an experimental basis by individual clinicians in countries such as Brazil, Cuba, Italy, Romania and the United States during the 1930s.[116]
Italian leucotomy
Amarro Fiamberti[117]
Throughout the remainder of the 1930s the number of leucotomies performed in most countries where the technique was adopted remained quite low. In Britain, which was later a major centre for leucotomy,[n 14] only six operations had been undertaken before 1942.[119] Generally, medical practitioners who attempted the procedure adopted a cautious approach and few patients were leucotomised before the 1940s. Italian neuropsychiatrists, who were typically early and enthusiastic adopters of leucotomy, were exceptional in eschewing such a gradualist course.[55]
Leucotomy was first reported in the Italian medical press in 1936 and Moniz published an article in Italian on the technique in the following year.[55] In 1937, he was invited to Italy to demonstrate the procedure and for a two-week period in June of that year he visited medical centres in Trieste, Ferrara, and one close to Turin – the Racconigi Hospital – where he instructed his Italian neuropsychiatric colleagues on leucotomy and also oversaw several operations.[55] Leucotomy was featured at two Italian psychiatric conferences in 1937 and over the next two years a score of medical articles on Moniz's psychosurgery was published by Italian clinicians based in medical institutions located in Racconigi, Trieste, Naples, Genoa, Milan, Pisa, Catania and Rovigo.[55] The major centre for leucotomy in Italy was the Racconigi Hospital, where the experienced neurosurgeon Ludvig Puusepp provided a guiding hand.[n 15][55] Under the medical directorship of Emilio Rizzatti, the medical personnel at this hospital had completed at least 200 leucotomies by 1939.[121] Reports from clinicians based at other Italian institutions detailed significantly smaller numbers of leucotomy operations.[55]
Experimental modifications of Moniz's operation were introduced with little delay by Italian medical practitioners.[122] Most notably, in 1937 Amarro Fiamberti, the medical director of a psychiatric institution in Varese,[123] first devised the transorbital procedure whereby the frontal lobes were accessed through the eye sockets.[122] Fiamberti's method was to puncture the thin layer of orbital bone at the top of the socket and then inject alcohol or formalin into the white matter of the frontal lobes through this aperture.[124] Using this method, while sometimes substituting a leucotome for a hypodermic needle, it is estimated that he leucotomised about 100 patients in the period up to the outbreak of World War II.[123] Fiamberti's innovation of Moniz's method would later prove inspirational for Walter Freeman's development of transorbital lobotomy.[124]
American leucotomy
The first prefrontal leucotomy in the United States was performed at the George Washington University Hospital on 14 September 1936 by the neurologist Walter Freeman and his friend and colleague, the neurosurgeon, James W. Watts.[125] Freeman had first encountered Moniz at the London-hosted Second International Congress of Neurology in 1935 where he had presented a poster exhibit of the Portuguese neurologist's work on cerebral angiography.[126] Fortuitously occupying a booth next to Moniz, Freeman, delighted by their chance meeting, formed a highly favourable impression of Moniz, later remarking upon his "sheer genius".[126] According to Freeman, if they had not met in person it is highly unlikely that he would have ventured into the domain of frontal lobe psychosurgery.[127] Freeman's interest in psychiatry was the natural outgrowth of his appointment in 1924 as the medical director of the Research Laboratories of the Government Hospital for the Insane in Washington, known colloquially as St Elizabeth's.[128] Ambitious and a prodigious researcher, Freeman, who favoured an organic model of mental illness causation, spent the next several years exhaustively, yet ultimately fruitlessly, investigating a neuropathological basis for insanity.[129] Chancing upon a preliminary communication by Moniz on leucotomy in the spring of 1936, Freeman initiated a correspondence in May of that year. Writing that he had been considering psychiatric brain surgery previously, he informed Moniz that, "having your authority I expect to go ahead".[130] Moniz, in return, promised to send him a copy of his forthcoming monograph on leucotomy and urged him to purchase a leucotome from a French supplier.[131]
Upon receipt of Moniz's monograph, Freeman reviewed it anonymously for the Archives of Neurology and Psychiatry.[131] Praising the text as one whose "importance can scarcely be overestimated",[131] he summarised Moniz's rationale for the procedure as based on the fact that while no physical abnormality of cerebral cell bodies was observable in the mentally ill, their cellular interconnections may harbour a "fixation of certain patterns of relationship among various groups of cells" and that this resulted in obsessions, delusions and mental morbidity.[132] While recognising that Moniz's thesis was inadequate, for Freeman it had the advantage of circumventing the search for diseased brain tissue in the mentally ill by instead suggesting that the problem was a functional one of the brain's internal wiring where relief might be obtained by severing problematic mental circuits.[132]
In 1937 Freeman and Watts adapted Lima and Moniz's surgical procedure, and created the Freeman-Watts technique, also known as the Freeman-Watts standard prefrontal lobotomy, which they styled the "precision method".[133]
Transorbital lobotomy
The Freeman-Watts prefrontal lobotomy still required drilling holes in the scalp, so surgery had to be performed in an operating room by trained neurosurgeons. Walter Freeman believed this surgery would be unavailable to those he saw as needing it most: patients in state mental hospitals that had no operating rooms, surgeons, or anesthesia and limited budgets. Freeman wanted to simplify the procedure so that it could be carried out by psychiatrists in psychiatric hospitals.[134]
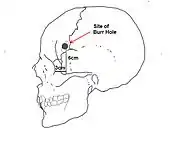
Inspired by the work of Italian psychiatrist Amarro Fiamberti, Freeman at some point conceived of approaching the frontal lobes through the eye sockets instead of through drilled holes in the skull. In 1945 he took an icepick[n 16] from his own kitchen and began testing the idea on grapefruit[n 17] and cadavers. This new "transorbital" lobotomy involved lifting the upper eyelid and placing the point of a thin surgical instrument (often called an orbitoclast or leucotome, although quite different from the wire loop leucotome described above) under the eyelid and against the top of the eyesocket. A mallet was used to drive the orbitoclast through the thin layer of bone and into the brain along the plane of the bridge of the nose, around 15 degrees toward the interhemispherical fissure. The orbitoclast was malleted 5 centimeters (2 in) into the frontal lobe, and then pivoted 40 degrees at the orbit perforation so the tip cut toward the opposite side of the head (toward the nose). The instrument was returned to the neutral position and sent a further 2 centimeters (4⁄5 in) into the brain, before being pivoted around 28 degrees each side, to cut outwards and again inwards. (In a more radical variation at the end of the last cut described, the butt of the orbitoclast was forced upwards so the tool cut vertically down the side of the cortex of the interhemispheric fissure; the "Deep Frontal Cut".) All cuts were designed to transect the white fibrous matter connecting the cortical tissue of the prefrontal cortex to the thalamus. The leucotome was then withdrawn and the procedure repeated on the other side.
Freeman performed the first transorbital lobotomy on a live patient in 1946. Its simplicity suggested the possibility of carrying it out in mental hospitals lacking the surgical facilities required for the earlier, more complex procedure. (Freeman suggested that, where conventional anesthesia was unavailable, electroconvulsive therapy be used to render the patient unconscious.)[136] In 1947, the Freeman and Watts partnership ended, as the latter was disgusted by Freeman's modification of the lobotomy from a surgical operation into a simple "office" procedure.[137] Between 1940 and 1944, 684 lobotomies were performed in the United States. However, because of the fervent promotion of the technique by Freeman and Watts, those numbers increased sharply towards the end of the decade. In 1949, the peak year for lobotomies in the US, 5,074 procedures were undertaken, and by 1951 over 18,608 individuals had been lobotomized in the US.[138]
Prevalence
In the United States, approximately 40,000 people were lobotomized. In England, 17,000 lobotomies were performed, and the three Nordic countries of Denmark, Norway, and Sweden had a combined figure of approximately 9,300 lobotomies.[139] Scandinavian hospitals lobotomized 2.5 times as many people per capita as hospitals in the US.[140] Sweden lobotomized at least 4,500 people between 1944 and 1966, mainly women. This figure includes young children.[141] In Norway, there were 2,005 known lobotomies.[142] In Denmark, there were 4,500 known lobotomies.[143] In Japan, the majority of lobotomies were performed on children with behavior problems. The Soviet Union banned the practice in 1950 on moral grounds. In Germany, it was performed only a few times.[144] By the late 1970s, the practice of lobotomy had generally ceased, although it continued as late as the 1980s in France.[145]
Criticism
As early as 1944 an author in the Journal of Nervous and Mental Disease remarked: "The history of prefrontal lobotomy has been brief and stormy. Its course has been dotted with both violent opposition and with slavish, unquestioning acceptance." Beginning in 1947 Swedish psychiatrist Snorre Wohlfahrt evaluated early trials, reporting that it is "distinctly hazardous to leucotomize schizophrenics" and that lobotomy was "still too imperfect to enable us, with its aid, to venture on a general offensive against chronic cases of mental disorder", stating further that "Psychosurgery has as yet failed to discover its precise indications and contraindications and the methods must unfortunately still be regarded as rather crude and hazardous in many respects."[146] In 1948 Norbert Wiener, the author of Cybernetics: Or the Control and Communication in the Animal and the Machine, said: "[P]refrontal lobotomy ... has recently been having a certain vogue, probably not unconnected with the fact that it makes the custodial care of many patients easier. Let me remark in passing that killing them makes their custodial care still easier."[147]
Concerns about lobotomy steadily grew. Soviet psychiatrist Vasily Gilyarovsky criticized lobotomy and the mechanistic brain localization assumption used to carry out lobotomy:
It is assumed that the transection of white substance of the frontal lobes impairs their connection with the thalamus and eliminates the possibility to receive from it stimuli which lead to irritation and on the whole derange mental functions. This explanation is mechanistic and goes back to the narrow localizationism characteristic of psychiatrists of America, from where leucotomy was imported to us.[148]
The USSR officially banned the procedure in 1950[149] on the initiative of Gilyarovsky.[150] Doctors in the Soviet Union concluded that the procedure was "contrary to the principles of humanity" and "'through lobotomy' an insane person is changed into an idiot".[151] By the 1970s, numerous countries had banned the procedure, as had several US states.[152]
In 1977 the US Congress, during the presidency of Jimmy Carter, created the National Committee for the Protection of Human Subjects of Biomedical and Behavioral Research to investigate allegations that psychosurgery—including lobotomy techniques—was used to control minorities and restrain individual rights. The committee concluded that some extremely limited and properly performed psychosurgery could have positive effects.[153]
There have been calls in the early 21st century for the Nobel Foundation to rescind the prize it awarded to Moniz for developing lobotomy, a decision that has been called an astounding error of judgment at the time and one that psychiatry might still need to learn from, but the Foundation declined to take action and has continued to host an article defending the results of the procedure.[154][5]
Notable cases
- Rosemary Kennedy, sister of President John F. Kennedy, underwent a lobotomy in 1941 that left her incapacitated and institutionalized for the rest of her life.[155]
- Howard Dully wrote a memoir of his late-life discovery that he had been lobotomized in 1960 at age 12.[156]
- New Zealand author and poet Janet Frame received a literary award in 1951 the day before a scheduled lobotomy was to take place, and it was never performed.[157]
- Josef Hassid, a Polish violinist and composer, was diagnosed with schizophrenia and died at the age of 26 following a lobotomy.[158]
- Swedish modernist painter Sigrid Hjertén died following a lobotomy in 1948.[159]
- American playwright Tennessee Williams' older sister Rose received a lobotomy that left her incapacitated for life; the episode is said to have inspired characters and motifs in certain works of his.[160]
- It is often said that when an iron rod was accidentally driven through the head of Phineas Gage in 1848, this constituted an "accidental lobotomy", or that this event somehow inspired the development of surgical lobotomy a century later. According to the only book-length study of Gage, careful inquiry turns up no such link.[161]
- In 2011, Daniel Nijensohn, an Argentine-born neurosurgeon at Yale, examined X-rays of Eva Perón and concluded that she underwent a lobotomy for the treatment of pain and anxiety in the last months of her life.[162]
Literary and cinematic portrayals
Lobotomies have been featured in several literary and cinematic presentations that both reflected society's attitude towards the procedure and, at times, changed it. Writers and film-makers have played a pivotal role in turning public sentiment against the procedure.[5]
- Robert Penn Warren's 1946 novel All the King's Men describes a lobotomy as making "a Comanche brave look like a tyro with a scalping knife", and portrays the surgeon as a repressed man who cannot change others with love, so he instead resorts to "high-grade carpentry work".[163]
- Tennessee Williams criticized lobotomy in his play Suddenly, Last Summer (1958) because it was sometimes inflicted on homosexuals—to render them "morally sane".[5] In the play a wealthy matriarch offers the local mental hospital a substantial donation if the hospital will give her niece a lobotomy, which she hopes will stop the niece's shocking revelations about the matriarch's son.[164] Warned that a lobotomy might not stop her niece's "babbling", she responds, "That may be, maybe not, but after the operation who would believe her, Doctor?"[165]
- In Ken Kesey's 1962 novel One Flew Over the Cuckoo's Nest and its 1975 film adaptation, lobotomy is described as "frontal-lobe castration", a form of punishment and control after which "There's nothin' in the face. Just like one of those store dummies." In one patient, "You can see by his eyes how they burned him out over there; his eyes are all smoked up and gray and deserted inside."[163]
- In Sylvia Plath's 1963 novel The Bell Jar, the protagonist reacts with horror to the "perpetual marble calm" of a lobotomized young woman.[163]
- Elliott Baker's 1964 novel and 1966 film version, A Fine Madness, portrays the dehumanizing lobotomy of a womanizing, quarrelsome poet who, afterwards, is just as aggressive as ever. The surgeon is depicted as an inhumane crackpot.[166]
- The 1982 biopic film Frances depicts actress Frances Farmer (the subject of the film) undergoing transorbital lobotomy (though the idea[167] that a lobotomy was performed on Farmer, and that Freeman performed it, has been criticized as having little or no factual foundation).[168]
- The 2018 film The Mountain centers around lobotomization, its cultural significance in the context of 1950s America, and mid-century attitudes surrounding mental health in general. The film interrogates the ethical and social implications of the practice through the experiences of its protagonist, a young man whose late mother had been lobotomized. The protagonist takes a job as a medical photographer for the fictional Dr. Wallace Fiennes, portrayed by Jeff Goldblum. Fiennes is loosely based on Freeman. [169][170]
See also
- Bilateral cingulotomy destruction of a part of the brain
- Bioethics and Medical ethics
- Frontal lobe disorder
- Frontal lobe injury
- Psychosurgery
- History of psychosurgery in the United Kingdom
Notes
- Walter Rudolf Hess, who was the joint winner with Moniz of the Nobel Prize in 1949 for his work on the function of the midbrain, had no involvement with leucotomy.[4]
- A 1937 report detailed that in the United States there were then 477 psychiatric institutions with a total population of approximately 451,672 patients, almost half of whom had been resident for a period of five years or more.[22] The report also observed that psychiatric patients occupied 55 per cent of all hospital-beds in America.[22] Conditions within U.S. mental hospitals became the subject of public debate as a series of exposés were published in the 1940s.[23] A 1946 Life magazine-article remarked that the nation's system of mental hospitals resembled "little more than concentration camps on the Belsen pattern";[24] a point the piece emphasized with documentary photography that depicted patient-neglect and dilapidated material conditions within psychiatric institutions.[25]
- Ugo Cerletti, the Italian psychiatrist and joint inventor with Lucio Bini of electroconvulsive therapy, described psychiatry during the interwar period as a "funereal science".[26] Likewise Egas Moniz, the inventor of leucotomy, referred to the "impotência terapeutica" (therapeutic impotence) of existing therapeutic remedies during the 1930s.[27]
- The patient he thought improved subsequently committed suicide.[43]
- According to Puusepp, the three patients were suffering from bipolar disorder or considered "epileptic equivalents".[50]
- Puusepp admitted to his 1910 experimentation with psychosurgery in a 1937 publication.[53] At that point he had completed a series of 14 leucotomies to relieve aggressive symptoms in patients. Convinced that the results had been positive in these cases, he felt that further research into psychosurgery was warranted.[52]
- Professor of neurology at the University of Lisbon from 1911 to 1944, Moniz was also for several decades a prominent parliamentarian and diplomat. He was Portugal's ambassador to Spain during World War I and represented Portugal at the postwar Versailles Treaty negotiations,[56] but after the Portuguese coup d'état of 1926, which ushered in the Ditadura Nacional (National Dictatorship), the Republican Moniz, then 51 years old, devoted his considerable talents and energies to neurological research entirely. Throughout his career he published on topics as diverse as neurology, sexology, historical biography, and the history of card games.[57] For his 1927 development of cerebral angiography, which allowed routine visualisation of the brain's peripheral blood-vessels for the first time, he was twice nominated, unsuccessfully, for a Nobel Prize. Some have attributed his development of leucotomy to a determination on his part to win the Nobel after these disappointments.[58]
- The American neuropsychiatrist Walter Freman also attended Congress, where he presented his research-findings on cerebral ventriculography. Freeman, who would later play a central role in the popularisation and practice of leucotomy in America, also had an interest in personality-changes following frontal-lobe surgery.[52]
- The patient suffered from meningioma, a rare form of brain tumour arising in the meninges.[75]
- Brickner and Davidoff had planned, before Moniz's first leucotomies, to operate on the frontal lobes to relieve depression.[83]
- Moniz wrote in 1948: 'sufferers from melancholia, for instance, are distressed by fixed and obsessive ideas ... and live in a permanent state of anxiety caused by a fixed idea which predominates over all their lives ... in contrast to automatic actions, these morbid ideas are deeply rooted in the synaptic complex which regulates the functioning of consciousness, stimulating it and keeping it in constant activity ... all these considerations led me to the following conclusion: it is necessary to alter these synaptic adjustments and change the paths chosen by the impulses in their constant passage so as to modify the corresponding ideas and force thoughts along different paths ...'[90]
- Lima described his role as that of an "instrument handled by the Master".[99]
- Before operating on live subjects, they practised the procedure on a cadaver head.[84]
- It was estimated by William Sargant and Eliot Slater that 15,000 leucotomies had been performed in the UK by 1962.[118]
- The 14 leucotomies reported by Puusepp in his 1937 paper were performed at the Racconigi Hospital.[120]
- Frank Freeman, Walter Freeman's son, stated in an interview with Howard Dully that: "He had several ice-picks that just cluttered the back of the kitchen drawer. The first ice-pick came right out of our drawer. A humble ice-pick to go right into the frontal lobes. It was, from a cosmetic standpoint, diabolical. Just observing this thing was horrible, gruesome." When Dully asked Frank Freeman, then a 79-year-old security guard, whether he was proud of his father, he replied: "Oh yes, yes, yeah. He was terrific. He was really quite a remarkable pioneer lobotomist. I wish he could have gotten further."[135]
- Rodney Dully, whose son Howard Dully had had a transorbital lobotomy performed on him by Walter Freeman when he was twelve years old, stated in an interview with his son that: "I only met him [Freeman] I think the one time. He described how accurate it [transorbital lobotomy] was and that he had practised the cutting on, literally, a carload of grapefruit, getting the right move and the right turn. That's what he told me."[135]
Citations
- Kaempffert 1941, p. 18.
- "Lobotomy: Definition, Procedure & History". Live Science. Retrieved 28 June 2018.
- Raz 2009, p. 116
- Nobelprize.org 2013.
- Sutherland 2004
- Levinson, Hugh (8 November 2011). "The strange and curious history of lobotomy". BBC News. BBC.
- Johnson, Jenell (17 October 2014). American Lobotomy: A Rhetorical History. University of Michigan Press. pp. 50–60. ISBN 978-0472119448. Retrieved 12 August 2017.
- El-Hai, Jack (21 December 2016). "Race and Gender in the Selection of Patients for Lobotomy". Wonders & Marvels. Retrieved 12 August 2017.
- "Lobotomies". Western University. Retrieved 12 August 2017.
- Kalat, James W. (2007). Biological psychology (9th ed.). Belmont, California: Wadsworth/Thomson Learning. p. 101. ISBN 9780495090793. Retrieved 21 December 2015.
- Zajicek, Benjamin (2017). "Banning the Soviet Lobotomy: Psychiatry, Ethics, and Professional Politics during Late Stalinism". Bulletin of the History of Medicine. 91 (1): 33–61. doi:10.1353/bhm.2017.0002. ISSN 1086-3176. PMID 28366896. S2CID 46563971.
- Gallea, Michael (Summer 2017). "A brief reflection on the not-so-brief history of the lobotomy". BCMedical Journal. 59: 302–04. Archived from the original on 7 February 2019. Retrieved 4 February 2019.
- Quoted in Pressman 2002, p. 48
- Noyes & Kolb 1962, pp. 550–55
- Partridge 1950, pp. 470–71
- Cooper 2014, pp. 143–54.
- Valenstein 1997, pp. 499–516
- Szasz 2007, pp. 151–72
- Freberg 2010, pp. 416–17
- Shutts 1982
- Raz 2013, pp. 101–13
- Feldman & Goodrich 2001, p. 650; Mashour, Walker & Martuza 2005, p. 411
- Maisel 1946; Wright 1947; Deutsch 1948;Feldman & Goodrich 2001, p. 650; Pressman 2002, pp. 148–50
- Albert Q. Maisel, "Bedlam 1946, Most U.S. Mental Hospitals are a Shame and a Disgrace", Life 20 (1946), pp. 102–03, quoted in Pressman 2002, p. 149
- Pressman 2002, pp. 148–49.
- Shorter 1997, p. 218.
- Gross & Schäfer 2011, p. 5
- Swayze 1995, pp. 505–15;Hoenig 1995, p. 337; Meduna 1985, p. 53
- Pressman 2002, p. 200
- Brown 2000, pp. 371–82.
- Shorter 1997, pp. 190–225; Jansson 1998
- Healy 2000, p. 404; Braslow 1995, pp. 600–05; Braslow 1997, pp. 89, 93
- Braslow 1997, p. 3.
- Cooter 2012, p. 216
- Porter 1999, p. 520.
- Pressman 2002, p. 428; Raz 2009, pp. 116, 129
- Gross & Schäfer 2011, p. 1; Heller et al. 2006, p. 727; Joanette et al. 1993, pp. 572, 575; Kotowicz 2008, p. 486; Manjila et al. 2008, p. 1; Noll 2007, p. 326; Reevy, Ozer & Ito 2010, p. 485; Steck 2010, pp. 85–89; Stone 2001, pp. 79–92; Suchy 2011, p. 37; Mareke & Fangerau 2010, p. 138; Ford & Henderson 2006, p. 219; Green et al. 2010, p. 208; Sakas et al. 2007, p. 366; Whitaker, Stemmer & Joanette 1996, p. 276
- Berrios 1997, p. 68
- Berrios 1997, p. 69
- Berrios 1997, pp. 69, 77
- Tierney 2000, p. 26
- Whitaker, Stemmer & Joanette 1996, p. 276; Berrios 1997, p. 69
- Stone 2001, p. 80.
- Berrios 1997, p. 70
- Manjila et al. 2008, p. 1.
- Kotowicz 2005, pp. 77–101
- Bechterev & Puusepp 1912; Kotowicz 2008, p. 486
- Kotowicz 2005, p. 80; Kotowicz 2008, p. 486
- Quoted in Berrios 1997, p. 71
- Feldman & Goodrich 2001, p. 149
- Kotowicz 2005, p. 80; Kotowicz 2008, p. 486; Berrios 1997, p. 71
- Feldman & Goodrich 2001, p. 649
- Puusepp 1937
- Kotowicz 2008, p. 486
- Kotowicz 2008, p. 477
- Tierney 2000, p. 23
- Tierney 2000, p. 25; Tierney 2000, pp. 22–23; Kotowicz 2005, pp. 78
- Shorter 1997, p. 226; Tierney 2000, pp. 25
- Doby 1992, p. 2; Tierney 2000, pp. 25
- El-Hai 2005, p. 100
- Berrios 1997, p. 72
- Pressman 2002, pp. 13–14, 48–51, 54–55; Berrios 1997, pp. 72–73; Shorter 1997, p. 226; Heller et al. 2006, p. 721
- Heller et al. 2006, p. 721
- Pressman 2002, p. 48.
- Pressman 2002, p. 48; Heller et al. 2006, p. 721
- Pressman 2002, p. 48; Berrios 1997, p. 73
- Berrios 1997, p. 73
- Pressman 2002, pp. 48–50
- Pressman 2002, p. 50
- Berrios 1997, pp. 72–73
- Pressman 2002, pp. 48–55; Valenstein 1997, p. 541
- Pressman 2002, pp. 51, 55
- Pressman 2002, p. 51
- Bianchi 1922; Pressman 2002, p. 51; Levin & Eisenberg 1991, p. 14
- Pressman 2002, p. 52; Kotowicz 2005, p. 84
- Brickner 1932
- Kotowicz 2005, p. 84
- Quoted in Pressman 2002, p. 52
- Pressman 2002, p. 52
- Quoted in Freeman & Watts 1944, p. 532
- Pressman 2002, p. 53
- Valenstein 1990, p. 541
- Valenstein 1997, p. 503
- Feldman & Goodrich 2001, p. 650
- Quoted in Valenstein 1990, p. 541
- Valenstein 1990, p. 541; Feldman & Goodrich 2001, p. 650; Kotowicz 2008, p. 478
- Berrios 1997, p. 77; Valenstein 1990, p. 541; Valenstein 1997, p. 503
- Quoted in Valenstein 1997, p. 503
- Gross & Schäfer 2011, p. 1
- Quoted in Berrios 1997, p. 74
- Kotowicz 2005, p. 99; Gross & Schäfer 2011, p. 1
- Quoted in Kotowicz 2005, p. 88
- Quoted in Feldman & Goodrich 2001, p. 651
- Berrios 1997, p. 74
- Kotowicz 2005, p. 89
- Moniz 1994, p. 237.
- Kotowicz 2005, pp. 80–81; Feldman & Goodrich 2001, p. 650
- Gross & Schäfer 2011, p. 2; Kotowicz 2008, p. 482
- , Gross & Schäfer 2011, p. 2
- Tierney 2000, p. 29; Kotowicz 2005, pp. 80–81; Gross & Schäfer 2011, p. 2
- Pressman 2002, p. 54
- Finger 2001, p. 292.
- Kotowicz 2005, p. 81
- Feldman & Goodrich 2001, p. 651
- Jansson 1998; Gross & Schäfer 2011, p. 2; Feldman & Goodrich 2001, p. 651. For Moniz's account of the procedure see, Moniz 1994, pp. 237–39
- Kotowicz 2005, p. 81; Feldman & Goodrich 2001, p. 651; Valenstein 1997, p. 504
- Berrios 1997, p. 75
- Kotowicz 2005, p. 92
- Berrios 1997, p. 75; Kotowicz 2005, p. 92
- Gross & Schäfer 2011, p. 3
- Berrios 1997, p. 74; Gross & Schäfer 2011, p. 3
- Kotowicz 2008, p. 482
- Quoted in Kotowicz 2008, p. 482
- Kotowicz 2008, pp. 482–83
- Kotowicz 2008, p. 483
- Feldman & Goodrich 2001, p. 652; Kotowicz 2005, p. 81
- Quoted in El-Hai 2005, p. 182
- Kotowicz 2008, pp. 486 n.1; Sargant & Slater 1963, p. 98
- Kotowicz 2008, pp. 476–77
- Puusepp 1937; Kotowicz 2008, pp. 477, 486
- Kotowicz 2008, pp. 477, 487
- Kotowicz 2008, p. 478
- El-Hai 2005, p. 182
- El-Hai 2005, p. 182; Finger 2001, p. 293; Weiss, Rauch & Price 2007, p. 506
- Shorter 1997, p. 227; Pressman 2002, p. 78
- Pressman 2002, p. 76; Feldman & Goodrich 2001, p. 649
- Pressman 2002, p. 76; Kotowicz 2005, p. 94
- Pressman 2002, p. 73
- Pressman 2002, pp. 73–75
- Quoted in Pressman 2002, p. 76
- Pressman 2002, p. 76
- Pressman 2002, p. 77
- Finger 2001, p. 293
- El-Hai 2005, p. 184.
- Dully 2005.
- El-Hai 2005
- Caruso, James P.; Sheehan, Jason P. (2017). "Psychosurgery, ethics, and media: a history of Walter Freeman and the lobotomy". Neurosurgical Focus. 43 (3): E6. doi:10.3171/2017.6.FOCUS17257. PMID 28859561.
- Shorter 1997, pp. 227–28
- Tranøy & Blomberg 2005, p. 107
- Tranøy 1996, pp. 1–20
- Ogren & Sandlund 2005, pp. 353–67
- Goldbeck-Wood 1996, pp. 708–09
- "Jesper Vaczy Kragh: "Sidste udvej? Træk af psykokirurgiens historie i Danmark" (Dansk Medicinhistorisk Årbog 2007)" (PDF). Archived from the original (PDF) on 5 March 2016. Retrieved 20 January 2018.
- Bangen, Hans: Geschichte der medikamentösen Therapie der Schizophrenie. Berlin 1992, ISBN 3-927408-82-4
- "La neurochirurgie fonctionnelle d'affections psychiatriques sévères" (PDF) (in French). Comité Consultatif National d'Ethique. 25 April 2002. Archived from the original (PDF) on 20 July 2011. (French national consultative committee on ethics, opinion #71: Functional neurosurgery of severe psychiatric conditions)
- Ogren & Sandlund 2005.
- Wiener 1948, p. 148.
- Gilyarovsky 1950
- Lichterman 1993, pp. 1–4; USSR Ministry of Health 1951, pp. 17–18
- Gilyarovsky 1973, p. 4
- Diefenbach et al. 1999, pp. 60–69
- Wood & Wood 2008, p. 153.
- DHEW 1977.
- Jansson, Bengt. "Controversial Psychosurgery Resulted in a Nobel Prize, first published 29 October 1998". Official website of the Nobel Prize. www.Nobelprize.org. Retrieved 21 March 2013.
- Feldman 2001, p. 271
- Day 2008
- Martin 2004
- Prior 2008
- Snyder & Steffen-Fluhr 2012, p. 52
- Kolin 1998, pp. 50–51
- Macmillan (2000, p. 250, 1999–2012)
- Nijensohn 2012, p. 582
- Grenander 1978, pp. 42–44
- Bigsby 1985, p. 100
- Williams 1998, p. 15
- Gabbard & Gabbard 1999, pp. 119–20
- Arnold 1982.
- Bragg 2005, pp. 72–75; El-Hai 2005, pp. 241–42
- Lapin, Andrew (25 July 2019). "A Lobotomist Struggles To Hang On In The Brilliant, Blistering 'The Mountain'". NPR. Retrieved 8 November 2020.
- Kohn, Eric (30 August 2018). "'The Mountain' Review: Jeff Goldblum and Tye Sheridan Are Lost Souls in Rick Alverson's Beautiful, Fractured America". IndieWire. Retrieved 8 November 2020.
Sources
Print Sources
- Acharya, Hernish J.. The Rise and Fall of Frontal Leucotomy. In: Whitelaw, W.A. (ed). The Proceedings of the 13th Annual History of Medicine Days. Calgary: 2004. p. 32–41.
- Arnold, William. Shadowland. Berkley Books; 1982. ISBN 0-425-05481-0.
- Bechterev, V.; Puusepp, L.. La chirugie des aliénes [Surgery of the Insane]. Archives Internationales de Neurologie. 1912;34:1–17, 69–89.
- Berrios, German E.. The Origins of Psychosurgery: Shaw, Burckhardt and Moniz. History of Psychiatry. 1997;8(1):61–81. doi:10.1177/0957154X9700802905. PMID 11619209.
- Bianchi, Leonardo. The Mechanism of the Brain and the Function of the Frontal Lobes. New York & Edinburgh: William Wood & Co; E.S Livingstone; 1922.
- Bigsby, C.W.E.. A Critical Introduction to Twentieth-Century American Drama: Volume 2. Cambridge University Press; 1985. ISBN 978-0-521-27717-4.
- Bragg, Lynn. Myths and Mysteries of Washington. 1st ed. TwoDot; 2005. ISBN 978-0-7627-3427-6.
- Braslow, Joel T.. Effect of therapeutic innovation on perception of disease and the doctor-patient relationship: a history of general paralysis of the insane and malaria fever therapy, 1910–1950. American Journal of Psychiatry. May 1995;152(2):660–65. PMID 7726304.
- Braslow, Joel T.. Mental Ills and Bodily Cures: Psychiatric Treatment in the First Half of the Twentieth Century. University of California; 1997. ISBN 0-520-20547-2.
- Brickner, Richard M.. An interpretation of frontal lobe function based upon the study of a case of partial bilateral frontal lobotomy. Research Publications – Association for Research for Nervous end Mental Disease. 1932;13:259–351.
- Brown, Edward M.. Why Wagner-Jauregg won the Nobel Prize for discovering malaria therapy for General Paresis of the Insane. History of Psychiatry. 2000 [archived 4 January 2013];11(4):371–82. doi:10.1177/0957154X0001104403.
- Cooper, Rachel. On deciding to have a lobotomy: either lobotomies were justified or decisions under risk should not always seek to maximise expected utility. Medicine, Health Care and Philosophy. 2014;17(1):143–54. doi:10.1007/s11019-013-9519-8.
- Cooter, Roger. Neuropatients in Historyland. In: Jacyna, Stephen J.; Casper, Stephen T. (eds). The Neurological Patient in History. Rochester, NY: University of Rochester Press; 2012. ISBN 978-1-58046-412-3. p. 215–222.
- Day, Elizabeth. He was bad, so they put an ice pick in his brain... The Guardian. 12 January 2008 [Retrieved 31 March 2010].
- Department of Health, Education, and Welfare. Protection on Human Subjects: Use of Psychosurgery in Practice and Research: Report and Recommendations for Public Comment. Part 3. Federal Register. 23 May 1977 [archived 18 June 2013];42(99):26317–32.
- Deutsch, Albert. Shame of the States. New York: Harcourt, Brace; 1948.
- Diefenbach, Gretchen; Diefenbach, Donald; Baumeister, Alan; West, Mark. Portrayal of lobotomy in the popular press: 1935–1960. Journal of the History of the Neurosciences. 1999 [archived 23 March 2010];8(1):60–69. doi:10.1076/jhin.8.1.60.1766. PMID 11624138.
- Doby, T. Cerebral Angiography and Egas Moniz. American Journal of Roentgenology. 1992;359(2):364.
- El-Hai, Jack. The Lobotomist: A Maverick Medical Genius and His Tragic Quest to Rid the World of Mental Illness. Wiley; 2005. ISBN 0-471-23292-0.
- Feldman, Burton. The Nobel prize: a history of genius, controversy, and prestige. Arcade Publishing; 2001. ISBN 1-55970-592-2.
- Feldman, Robert P.; Goodrich, James T.. Psychosurgery: A Historical Overview. Neurosurgery. March 2001;48(3):647–57; discussion 657–59. doi:10.1097/00006123-200103000-00041. PMID 11270556.
- Finger, Stanley. Origins of Neuroscience: A History of Explorations into Brain Function. Oxford: Oxford University Press; 2001. ISBN 978-0-19-514694-3.
- Ford, Paul J.; Henderson, Jaimie M.. Functional neurosurgical intervention: neuroethics in the operating rooms. In: Illes, Judy (ed.). Neuroethics: defining the issues in theory, practice, and policy. Oxford University Press; 2006. ISBN 978-0-19-856721-9.
- Freberg, Laura A.. Discovering Biological Psychology. 2nd ed. Belmont, California: Wadsworth; 2010. ISBN 0-547-17779-8.
- Freeman, Walter; Watts, James W.. Psychosurgery: An Evaluation of Two Hundred Cases over Seven Years. Journal of Mental Science. 1944;90(379):532–37. doi:10.1192/bjp.90.379.532.
- Gabbard, Glen O.; Gabbard, Krin. Psychiatry and the Cinema. 2nd ed. American Psychiatric Publishing, Inc.; 1999. ISBN 978-0-88048-964-5.
- Gilyarovsky, Vasily [Гиляровский, Василий]. Учение Павлова – основа психиатрии [Pavlov's teaching is the basis of psychiatry]. Медицинский работник [Health Worker]. 14 September 1950;(37). Russian.
- Gilyarovsky, Vasily [Гиляровский, Василий]. Избранные труды [Selected Works]. Moscow: Медицина [Medicine]; 1973. Russian. p. 4.
- Goldbeck-Wood, Sandra. Norway compensates lobotomy victims. British Medical Journal. 21 September 1996;313(7059):708–09. doi:10.1136/bmj.313.7059.708a. PMID 11644825.
- Green, Alexander; Astradsson, A.; Stacey, R.J.; Aziz, T.Z.. Functional and epilepsy neurosurgery. In: Johnson, Reuben; Green, Alexander (eds). Landmark Papers in Neurosurgery. Oxford University Press; 2010. ISBN 978-0-19-959125-1.
- Grenander, M.E.. Of Graver Import Than History: Psychiatry In Fiction. Journal of Libertarian Studies. 1978 [Retrieved 22 January 2008];2(1):29–44. PMID 11614766.
- Gross, Dominik; Schäfer, Gereon. Egas Moniz (1874–1955) and the "invention" of modern psychosurgery: a historical and ethical reanalysis under special consideration of Portuguese original sources. Neurosurgical Focus. 2011;30(2):8. doi:10.3171/2010.10.FOCUS10214. PMID 21284454.
- Healy, David. Some continuities and discontinuities in the pharmacotherapy of nervous conditions before and after chlorpromazine and imipramine. History of Psychiatry. January 2000;11(44):393–412. doi:10.1177/0957154X0001104405.
- Heller, A. C.; Amar, A.P.; Liu, C.Y.; Apuzzo, M.L.J.. Surgery of the mind and mood: A mosaic of issues in time and evolution. Neurosurgery. 2006;59(4):727.
- Hoenig, J.. Schizophrenia. In: Berrios, German E.; Porter, Roy (eds). A History of Clinical Psychiatry: The Origin and History of Psychiatric Disorders. Athlone; 1995. ISBN 0-485-24011-4.
- Joanette, Yves; Stemmer, Brigitte; Assal, Gil; Whitaker, Harry. From theory to practice: the unconventional contribution of Gottlieb Burckhardt to psychosurgery. Brain and Language. 1993;45(4):572–87. doi:10.1006/brln.1993.1061. PMID 8118674.
- Kaempffert, Waldemar. Turning the Mind Inside Out. Saturday Evening Post. 24 May 1941;213(47):18–19, 69–74.
- Kolin, Philip. Something Cloudy, Something Clear: Tennessee Williams's Postmodern Memory Play. Journal of Dramatic Theory and Criticism. Spring 1998;12(2):35–55.
- Kondratev, Fedor [Фёдор Кондратьев]. Судьбы больных шизофренией: клинико-социальный и судебно-психиатрический аспекты [The fates of the ill with schizophrenia: clinico-social and forensico-psychiatric aspects]. Moscow: ЗАО Юстицинформ [Closed joint-stock company Justitsinform]; 2010. Russian.
- Kotowicz, Zbigniew. Gottlieb Burckhardt and Egas Moniz – Two Beginnings of Psychosugery. Gesnerus. 2005 [archived 15 December 2011; Retrieved 26 November 2009];62(1/2):77–101.
- Kotowicz, Zbigniew. Psychosurgery in Italy, 1936–39. History of Psychiatry. December 2008;19(4):476–489. doi:10.1177/0957154X07087345. PMID 19397090.
- Kragh, J.V.. Shock Therapy in Danish Psychiatry. Medical History. 2010;54(3):341–64. doi:10.1017/S0025727300004646. PMID 20592884.
- Levin, Harvey S.; Eisenberg, Howard M.. Frontal Lobe Function and Dysfunction. Oxford: Oxford University Press; 1991. ISBN 978-0-19-506284-7.
- Lichterman, B.L.. On the history of psychosurgery in Russia. Acta Neurochirugie. 1993;125(1–4):1–4. doi:10.1007/BF01401819. PMID 8122532.
- Maisel, Albert Q.. Bedlam 1946, Most U.S. Mental Hospitals are a Shame and a Disgrace. 6 May 1946.
- Manjila, S.; Rengachary, S.; Xavier, A.R.; Parker, B.; Guthikonda, M.. Modern psychosurgery before Egas Moniz: a tribute to Gottlieb Burckhardt. Neurosurgery Focus. 2008;25(1):1–4.
- Macmillan, M.. An Odd Kind of Fame: Stories of Phineas Gage. MIT Press; 2000. ISBN 0-262-13363-6.
- Mareke, Arends; Fangerau, Heiner. Deep brain stimulation in psychiatric disorders. In: Fangerau, Heiner; Jörg, Fegert; Mareke, Arends (eds). Implanted Minds: The Neuroethics of Intracerebral Stem Cell Transplantation and Deep Brain Stimulation. Verlag; 2010. ISBN 978-3-8376-1433-6.
- Martin, Douglas. Janet Frame, 79, Writer Who Explored Madness. The New York Times. 30 January 2004 [Retrieved 17 November 2007].
- Mashour, George A.; Walker, Erin E.; Martuza, Robert L.. Psychosurgery: Past, Present, and Future. Brain Research Reviews. 2005 [archived 17 January 2013];48(3):409–19. doi:10.1016/j.brainresrev.2004.09.002. PMID 15914249.
- Meduna, L.J.. Autobiography of L.J. Meduna. Convulsive Therapy. 1985;1(1):43–57. PMID 11940805.
- Moniz, Egas. Prefrontal Leucotomy in the Treatment of Mental Disorders (1937) American Journal of Psychiatry 1844–1944. American Psychiatric Publishing; 1994. ISBN 978-0-89042-275-5. p. 237–39.
- Nijensohn, DE. New evidence of prefrontal lobotomy in the last months of the illness of Eva Perón. World Neurosurgery. 2012;77(3-4):582–90. doi:10.1016/j.wneu.2011.02.036. PMID 22079825.
- Noll, Richard. The encyclopedia of schizophrenia and other psychotic disorders. Infobase Publishing; January 2007. ISBN 978-0-8160-6405-2.
- Noyes, A.P.; Kolb, L.C.. Modern clinical psychiatry. Philadelphia and London: W.B. Saunders; 1962.
- Ogren, K.; Sandlund, M.. Psychosurgery in Sweden 1944–1964. Journal of the History of the Neurosciences. 2005;14(4):353–67. doi:10.1080/096470490897692. PMID 16338693.
- Partridge, Maurice. Pre-frontal leucotomy:. Oxford: Blackwell Scientific Publications; 1950.
- Pressman, Jack D.. Last Resort: Psychosurgery and the Limits of Medicine. Cambridge: Cambridge University Press; 2002. ISBN 0-521-52459-8.
- Prior, Alex. Music's boy wonder: Composer, conductor, singer ... and he's only fifteen. The Independent. 6 February 2008 [Retrieved 11 July 2010].
- Porter, Roy. The Greatest Benefit to Mankind: A Medical History of Humanity from Antiquity to the Present. Fontana Press; 1999. ISBN 0-00-637454-9.
- Puusepp, L.. Alcune considerazioni sugli interventi chirurgici nelle malattie mentali [Some Considerations about Surgery in Mental Illness]. G Accad Med Torino. 1937;100:3–16.
- Raz, Mical. Psychosurgery, Industry and Personal Responsibility, 1940–1965. Social History of Medicine. 2009;23(1):116–33. doi:10.1093/shm/hkp061.
- Raz, Mical. The lobotomy letters: the making of American psychosurgery. University of Rochester Press; 2013. ISBN 9781580464499.
- Reevy, Gretchen; Ozer, Yvette Malamud; Ito, Yuri. Encyclopedia of Emotion. ABC-CLIO; 2010. ISBN 978-0-313-34576-0.
- Sakas, Damianos E.; Panourias, L.G.; Singounas, E.; Simpson, B.A.. Neurosurgery for psychiatric disorders: from the excision of brain tissue to the chronic electrical stimulation of neural networks. In: Sakas, D.E.; Simpson, B.A. (eds). Operative Neuromodulation. Functional Neuroprosthetic Surgery. Volume II: Neural Networks Surgery. Vol. 2. Springer; 2007. ISBN 978-3-211-33081-4. p. 365–74.
- Shorter, Edward. A History of Psychiatry: From the Era of the Asylum to the Age of Prozac. Wiley; 1997. ISBN 0-471-24531-3.
- Snyder, John; Steffen-Fluhr, Nancy. Overcoming Depression Without Drugs: Mahler's Polka With Introductory Funeral March. AuthorHouse; 2012. ISBN 1-4685-4962-6.
- Shutts, David. Lobotomy: resort to the knife. Van Nostrand Reinhold; 1982. ISBN 978-0-442-20252-1.
- Sargant, William; Slater, Elliot. An Introduction to Physical Methods of Treatment in Psychiatry. Williams & Wilkins; 1963.
- Steck, A.J.. Milestones in the development of neurology and psychiatry in Europe. Schweizer Archiv für Neurologie und Psychiatrie. 2010;161(3):85–89. doi:10.4414/sanp.2010.02153.
- Stone, James L.. Gottlieb Burckhardt – The Pioneer of Psychosurgery. Journal of the History of the Neurosciences. 2001;10(1):79–92. doi:10.1076/jhin.10.1.79.5634. PMID 11446267.
- Suchy, Yana. Clinical Neuropsychology of Emotion. Guilford Press; 2011. ISBN 978-1-60918-072-0.
- Swayze, V.W.. Frontal leukotomy and related psychosurgical procedures in the era before antipsychotics (1935–1954): a historical overview. American Journal of Psychiatry. 1995;152(4):505–15. doi:10.1176/ajp.152.4.505. PMID 7900928.
- Szasz, Thomas. Coercion as Cure: A Critical History of Psychiatry. New Brunswick, New Jersey: Transaction; 2007. ISBN 0-7658-0379-8.
- Tierney, Ann Jane. Egas Moniz and the Origins of Psychosurgery: A Review Commemorating the 50th Anniversary of Moniz's Nobel Prize. Journal of the History of the Neurosciences. April 2000;9(1):22–36. doi:10.1076/0964-704X(200004)9:1;1-2;FT022. PMID 11232345.
- Tranøy, Joar. Lobotomy in Scandinavian psychiatry. The Journal of Mind and Behavior. 1996 [archived 26 May 2008];17(1):1–20.
- Tranøy, Joar; Blomberg, Wenche. Lobotomy in Norwegian Psychiatry. History of Psychiatry. 2005 [archived 3 December 2007];16(1):107–10. doi:10.1177/0957154X05052224.
- USSR Ministry of Health. Приказ МЗ СССР 1003 (9 декабря 1950) [Order 1003 (9 December 1950)]. Невропатология и психиатрия [Neuropathology and Psychiatry]. 1951;20(1):17–18. Russian.
- Valenstein, Elliot S.. The Prefrontal Area and Psychosurgery. In: Uylings, H.B.M.; Van Eden, C.G.; De Bruin, J.P.C.; Corner, M.A.; Feenstra, M.G.P. (eds). The Prefrontal Cortex: Its Structure, Function and Pathology. Amsterdam & New York: Elsevier; 1990. (Progress in Brain Research, Volume 85). ISBN 978-0-444-81124-0. p. 539–54.
- Valenstein, Elliot A.. History of Psychosurgery. In: Greenblatt, Samuel H. (ed.). A History of Neurosurgery: In Its Scientific and Professional Contexts. Contributing editors Dagi, T. Forcht; Epstein, Mel H.. Park Ridge, IL: The American Association of Neurological Surgeons; 1997. ISBN 978-1-879284-17-3. p. 499–516.
- Weiss, Anthony P.; Rauch, Scott L.; Price, Bruce H.. Neurosurgical intervention for psychiatric illness: past, present and future. In: Miller, Bruce L.; Cummings, Jeffrey L. (eds). The Human Frontal Lobes: Functions and Disorders. Guilford Press; 2007. ISBN 978-1-59385-329-7. p. 505–17.
- Whitaker, H.A.; Stemmer, B.; Joanette, Y.. A psychosurgical chapter in the history of cerebral localization: the six cases of Gottlieb Burkhardt. In: Code, Christopher; Wallesch, C.-W.; Joanette Y.; Roch A. (eds). Classic Cases in Neuropsychology. Hove: Psychology Press; 1996. ISBN 978-0-86377-395-2. p. 275–304.
- Wiener, Norbert. Cybernetics. MIT Press; 1948. ISBN 0-262-73009-X.
- Williams, Tennessee. Suddenly Last Summer. Dramatists Play Service; 1998. ISBN 978-0-8222-1094-8.
- Wood, Jeffrey C.; Wood, Minnie. Therapy 101: A Brief Look at Modern Psychotherapy Techniques & How They Can Help. New Harbinger Publications; 2008. ISBN 978-1-57224-568-6.
- Wright, Frank Leon. Out of Sight, Out of Mind: A Graphic Picture of Present-day Institutional Care of the Mentally Ill in America, Based on More Than Two Thousand Eye-witness Reports. Philadelphia: Mental Health Foundation; 1947.
Online sources
- Dully, Howard. NPR. "My Lobotomy": Howard Dully's Journey [podcast]; 16 November 2005 [Retrieved 28 November 2009].
- Jansson, Bengt. Nobel Media [Retrieved 24 January 2012]. Controversial Psychosurgery Resulted in a Nobel Prize; 29 October 1998.
- Macmillan, Malcolm. The Center for the History of Psychology, University of Akron, Ohio, USA. The Phineas Gage Information Page: Lobotomy; 1999–2012 [Retrieved 21 March 2009].
- Nobel Media. The Nobel Prize in Physiology or Medicine 1949 Walter Hess, Egas Moniz; 2013 [Retrieved 24 January 2013].
- Sutherland, John. Should they de-Nobel Moniz?. The Guardian. 5 August 2004 [Retrieved 22 December 2011].
External links
| Look up lobotomy in Wiktionary, the free dictionary. |
- My Lobotomy Radio story: Interview with Sallie Ellen Ionesco Lobotomised in 1946
- Mental Cruelty: Sunday Times article on lobotomy and contemporary psychosurgery
- Lobotomy's back: Discover article on cingulotomy
- 'My Lobotomy': Howard Dully's Journey. NPR Radio Documentary
- A Qualified Defence of 'Then': QJM
- Ten Notable Lobotomies
- Nobel Panel Urged to Rescind Prize for Lobotomies
- The Lobotomists: BBC Radio 4 documentary on the history of lobotomy