Presbyopia
Presbyopia is physiological insufficiency of accommodation associated with the aging of the eye that results in progressively worsening ability to focus clearly on close objects.[4] Symptoms include difficulty reading small print, having to hold reading material farther away, headaches, and eyestrain.[4] Different people will have different degrees of problems.[1] Other types of refractive errors may exist at the same time as presbyopia.[1]
| Presbyopia | |
|---|---|
| Other names | The aging eye condition[1] |
 | |
| The small print of an ingredients list is hard to read for a person with presbyopia. | |
| Specialty | Optometry, ophthalmology |
| Symptoms | Hard time reading small print, having to hold reading material farther away, headaches, eyestrain[1] |
| Usual onset | Progressively worsening in those > 40 years old[1] |
| Causes | Aging-related hardening of the lens of the eye[1] |
| Diagnostic method | Eye exam[1] |
| Treatment | Eyeglasses,[1] contact lenses[2] |
| Frequency | 25% currently;[3] all eventually affected[1] |
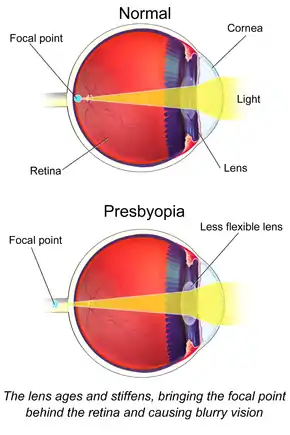
Presbyopia is a normal part of the aging process.[4] It occurs due to age related changes in lens (decreased elasticity and increased hardness) and ciliary muscle power of the eye, causing the eye to focus light behind rather than on the retina when looking at close objects.[4] It is a type of refractive error along with nearsightedness, farsightedness, and astigmatism.[4] Diagnosis is by an eye examination.[4]
Presbyopia can be corrected using glasses, contact lenses, multifocal intraocular lenses, or LASIK (presbyLASIK) surgery.[2][5][4] The most common treatment is glass correction using appropriate convex lens. Glasses used to correct presbyopia may be simple reading glasses, bifocals, trifocals, or progressive lens.[4]
People over 40 are at risk for developing presbyopia and all people become affected to some degree.[1] Around 25% of people (1.8 billion globally) are currently affected.[3]
Signs and symptoms
The first symptoms most people notice are difficulty reading fine print, particularly in low light conditions, eyestrain when reading for long periods, blurring of near objects or temporarily blurred vision when changing the viewing distance. Many extreme presbyopes complain that their arms have become "too short" to hold reading material at a comfortable distance.
Presbyopia, like other focal imperfections, becomes less noticeable in bright sunlight when the pupil becomes smaller.[6] As with any lens, increasing the focal ratio of the lens increases depth of field by reducing the level of blur of out-of-focus objects (compare the effect of aperture on depth of field in photography).
The onset of presbyopia varies among those with certain professions and those with miotic pupils.[7] In particular, farmers and homemakers seek correction later, whereas service workers and construction workers seek correction earlier. Scuba divers with interest in underwater photography may notice presbyopic changes while diving before they recognize the symptoms in their normal routines due to the near focus in low light conditions.[8]
Interaction with myopia
Many people with near-sightedness can read comfortably without eyeglasses or contact lenses even after age forty. However, their myopia does not disappear and the long-distance visual challenges remain. Myopes considering refractive surgery are advised that surgically correcting their nearsightedness may be a disadvantage after age forty, when the eyes become presbyopic and lose their ability to accommodate or change focus, because they will then need to use glasses for reading. Myopes with astigmatism find near vision better, though not perfect, without glasses or contact lenses when presbyopia sets in, but the more astigmatism, the poorer the uncorrected near vision.
A surgical technique offered is to create a "reading eye" and a "distance vision eye", a technique commonly used in contact lens practice, known as monovision. Monovision can be created with contact lenses, so candidates for this procedure can determine if they are prepared to have their corneas reshaped by surgery to cause this effect permanently.
Mechanism
The cause of presbyopia is lens hardening by decreasing levels of α-crystallin, a process which may be sped up by higher temperatures.[9] It results in a near point greater than 25 cm[10] (or equivalently, less than 4 diopters).
In optics, the closest point at which an object can be brought into focus by the eye is called the eye's near point. A standard near point distance of 25 cm is typically assumed in the design of optical instruments, and in characterizing optical devices such as magnifying glasses.
There is some confusion over how the focusing mechanism of the eye works. In the 1977 book, Eye and Brain,[11] for example, the lens is said to be suspended by a membrane, the 'zonula', which holds it under tension. The tension is released, by contraction of the ciliary muscle, to allow the lens to become more round, for close vision. This implies the ciliary muscle, which is outside the zonula, must be circumferential, contracting like a sphincter, to slacken the tension of the zonula pulling outwards on the lens. This is consistent with the fact that our eyes seem to be in the 'relaxed' state when focusing at infinity, and also explains why no amount of effort seems to enable a myopic person to see farther away.
The ability to focus on near objects declines throughout life, from an accommodation of about 20 dioptres (ability to focus at 50 mm away) in a child, to 10 dioptres at age 25 (100 mm), and levels off at 0.5 to 1 dioptre at age 60 (ability to focus down to 1–2 meters only). The expected, maximum, and minimum amplitudes of accommodation in diopters (D) for a corrected patient of a given age can be estimated using Hofstetter's formulas: expected amplitude (D) = 18.5 - 0.3 × (age in years), maximum amplitude (D) = 25 - 0.4 × (age in years), minimum amplitude (D) = 15 - 0.25 × (age in years).[12]
Treatment
In the visual system, images captured by the eye are translated into electric signals that are transmitted to the brain where they are interpreted. As such, in order to overcome presbyopia, two main components of the visual system can be addressed: image capturing by the optical system of the eye and image processing in the brain.
Image capturing in the eye
Solutions for presbyopia have advanced significantly in recent years, thanks to widened availability of optometry care as well as over-the-counter vision correction.
Corrective lenses
Corrective lenses provide a range of vision correction, some as high as +4.0 diopter. People with presbyopia choose convex lens for reading glasses; specialized preparations of convex lens usually require the services of an optometrist.[13]
Contact lenses can also be used to correct the focusing loss that comes along with presbyopia. Multifocal contact lenses can be used to correct vision for both the near and the far. Some people choose contact lenses to correct one eye for near and one eye for far with a method called monovision.
Surgery
Refractive surgery has been done to create multifocal corneas.[14] PresbyLASIK, a type of multifocal corneal ablation LASIK procedure may be used to correct presbyopia. Results are, however, more variable and some people have a decrease in visual acuity.[15] Concerns with refractive surgeries for presbyopia include people's eyes changing with time also.[14] Other side effects of multifocal corneal ablation include postoperative glare, halos, ghost images, and monocular diplopia.[16]
Image processing in the brain
A number of studies have claimed improvements in near visual acuity by the use of training protocols based on perceptual learning and requiring the detection of briefly presented low-contrast Gabor stimuli; study participants suffering from presbyopia were enabled to read smaller font sizes and to increase their reading speed.[17][18][19][20]
Etymology
The term is from Greek πρέσβυς presbys meaning "old" and ὤψ ōps meaning "sight" (GEN ὠπός ōpos)[21][22]).
Research
Eye drops to constrict the pupil are being studied for presbyopia.[23]
History
The condition was mentioned as early as the writings of Aristotle in the 4th century BC.[24] Glass lenses first came into use for the problem in the late 13th century.[24]
References
- "Facts About Presbyopia". NEI. October 2010. Archived from the original on 4 October 2016. Retrieved 11 September 2016.
- Pérez-Prados, Roque; Piñero, David P; Pérez-Cambrodí, Rafael J; Madrid-Costa, David (March 2017). "Soft multifocal simultaneous image contact lenses: a review". Clinical and Experimental Optometry. 100 (2): 107–127. doi:10.1111/cxo.12488. PMID 27800638. S2CID 205049139.
- Fricke, Timothy R.; Tahhan, Nina; Resnikoff, Serge; Papas, Eric; Burnett, Anthea; Ho, Suit May; Naduvilath, Thomas; Naidoo, Kovin S. (October 2018). "Global Prevalence of Presbyopia and Vision Impairment from Uncorrected Presbyopia". Ophthalmology. 125 (10): 1492–1499. doi:10.1016/j.ophtha.2018.04.013. PMID 29753495.
- Khurana, AK (September 2008). "Asthenopia, anomalies of accommodation and convergence". Theory and practice of optics and refraction (2nd ed.). Elsevier. pp. 100–107. ISBN 978-81-312-1132-8.
- "PresbyLASIK - EyeWiki". eyewiki.aao.org. Retrieved 27 August 2020.
- "Presbyopia: Patient Information". Marquette, MI: Eye Associates of Marquette. 2008. Archived from the original on 2 December 2008. Retrieved 31 October 2010.
- García Serrano, JL; López Raya, R; Mylonopoulos Caripidis, T (November 2002). "Variables related to the first presbyopia correction" (Free full text). Archivos de la Sociedad Española de Oftalmología. 77 (11): 597–604. ISSN 0365-6691. PMID 12410405. Archived from the original on 7 October 2011.
- Bennett QM (June 2008). "New thoughts on the correction of presbyopia for divers". Diving Hyperb Med. 38 (2): 163–164. PMID 22692711. Archived from the original on 19 April 2013. Retrieved 19 April 2013.
- Pathai, S; Shiels, PG; Lawn, SD; Cook, C; Gilbert, C (March 2013). "The eye as a model of ageing in translational research--molecular, epigenetic and clinical aspects". Ageing Research Reviews. 12 (2): 490–508. doi:10.1016/j.arr.2012.11.002. PMID 23274270. S2CID 26015190.
- Katz, Debora M. (2015). Physics for Scientists and Engineers: Foundations and Connections, Advance Edition. Cengage Learning. ISBN 978-1-305-53720-0.
- Gregory, Richard Langton (1977). Eye and brain : the psychology of seeing (3rd ed. rev. and update. ed.). New York; Toronto: McGraw-Hill. ISBN 978-0070246652.
- Robert P. Rutstein, Kent M. Daum, Anomalies of Binocular Vision: Diagnosis & Management, Mosby, 1998.
- Li, G; Mathine, DL; Valley, P; Ayräs, P; Haddock, JN; Giridhar, MS; Williby, G; Schwiegerling, J; et al. (April 2006). "Switchable electro-optic diffractive lens with high efficiency for ophthalmic applications". Proceedings of the National Academy of Sciences of the United States of America. 103 (16): 6100–4. Bibcode:2006PNAS..103.6100L. doi:10.1073/pnas.0600850103. ISSN 0027-8424. PMC 1458838. PMID 16597675.
- Kim, Tae-im; del Barrio, Jorge L Alió; Wilkins, Mark; Cochener, Beatrice; Ang, Marcus (May 2019). "Refractive surgery". The Lancet. 393 (10185): 2085–2098. doi:10.1016/S0140-6736(18)33209-4. PMID 31106754. S2CID 4474834.
- Pallikaris IG, Panagopoulou SI (July 2015). "PresbyLASIK approach for the correction of presbyopia". Current Opinion in Ophthalmology. 26 (4): 265–72. doi:10.1097/icu.0000000000000162. PMID 26058023. S2CID 35434343.
- Dimitri T., Azar (2007). "Terminology, classification, and history of refractive surgery". Refractive surgery (2nd ed.). Philadelphia: Mosby / Elsevier. ISBN 978-0-323-03599-6. OCLC 853286620.
- Polat U., Schor C., Tong J., Zomet A., Lev M., Yehezkel O., Sterkin A., Levi D.M. (2012). "Training improves visual processing speed and generalizes to untrained functions". Scientific Reports. 2: 278. Bibcode:2012NatSR...2E.278P. doi:10.1038/srep00278. PMC 3284862. PMID 22363834.CS1 maint: multiple names: authors list (link)
- Lev, M., Ludwig, K., Gilaie-Dotan, S. et al.. Training the brain to overcome the effect of aging on the human eye. Scientific Reports. 2012 [Retrieved 12-01-2021];4(1):7251. doi:10.1038/srep00278.
- DeLoss, Denton J., Watanabe, Takeo, Andersen, George J.. Optimization of perceptual learning: Effects of task difficulty and external noise in older adults. Vision research. 2014 [Retrieved 12-01-2021];99:37-45. doi:10.1016/j.visres.2013.11.003.
- Sterkin A, Levy Y, Pokroy R, Lev M, Levian L, Doron R, Yehezkel O, Fried M, Frenkel-Nir Y, Gordon B, Polat U.. Vision improvement in pilots with presbyopia following perceptual learning. Vision research. 2018 [Retrieved 12-01-2021];(152):61-73. doi:10.1016/j.visres.2017.09.003. PMID 29154795.
- "Presbyopia". Dictionary.reference.com. Archived from the original on 12 April 2013. Retrieved 19 April 2013.
- "Presbyopia". Etymonline.com. Archived from the original on 18 August 2017. Retrieved 4 May 2017.
- Dick, HB (July 2019). "Small-aperture strategies for the correction of presbyopia". Current Opinion in Ophthalmology. 30 (4): 236–242. doi:10.1097/ICU.0000000000000576. PMID 31033734.
- Wade, Nicholas J.; Wade, Nicholas (2000). A Natural History of Vision. MIT Press. p. 50. ISBN 9780262731294. Archived from the original on 8 September 2017.
External links
| Look up presbyopia in Wiktionary, the free dictionary. |
- "Presbyopia" at MedLinePlus Medical Encyclopedia
| Classification | |
|---|---|
| External resources |