Activated protein C resistance
Activated protein C resistance (APCR) is a hypercoagulability (an increased tendency of the blood to clot) characterized by a lack of a response to activated protein C (APC), which normally helps prevent blood from clotting excessively. This results in an increased risk of venous thrombosis (blood clots in veins), which resulting in medical conditions such as deep vein thrombosis (usually in the leg) and pulmonary embolism (in the lung, which can cause death).[1]
| Activated protein C resistance (APCR) | |
|---|---|
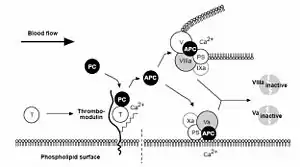 | |
| Protein C Anticoagulant Pathway: Thrombin escaping from a site of vascular injury binds to its receptor thrombomodulin (TM) on the intact cell surface. As a result, thrombin loses its procoagulant properties and instead becomes a potent activator of protein C. Activated protein C (APC) functions as a circulating anticoagulant, which specifically degrades and inactivates the phospholipid-bound factors Va and VIIIa. This effectively down-regulates the coagulation cascade and limits clot formation to sites of vascular injury. T = Thrombin, PC= Protein C, Activated Protein C= APC, PS= Protein S | |
| Specialty | Hematology |
Presentation
Associated conditions
An estimated 64 percent of patients with venous thromboembolism may have activated protein C resistance.[2]
Genetics
The disorder can be acquired or inherited, the hereditary form having an autosomal dominant inheritance pattern.[3]
Pathophysiology
Activated protein C (with protein S as a cofactor) degrades Factor Va and Factor VIIIa. Activated protein C resistance is the inability of protein C to cleave Factor Va and/or Factor VIIIa, which allows for longer duration of thrombin generation and may lead to a hypercoagulable state. This may be hereditary or acquired.[4] The best known and most common hereditary form is Factor V Leiden. Acquired forms occur in the presence of elevated Factor VIII concentrations.
Diagnosis
"APC(Activated protein C) ratio: To diagnose functional assays | PCR(Polymerase chain reaction)/ Restriction enzyme analysis: To detect the specific genetic anomaly responsible for FVL(factor V Leiden) "
References
- Dahlbäck B (2003). "The discovery of activated protein C resistance". J. Thromb. Haemost. 1 (1): 3–9. doi:10.1046/j.1538-7836.2003.00016.x. PMID 12871530. S2CID 2147784.
- Sheppard DR (2000). "Activated protein C resistance: the most common risk factor for venous thromboembolism". J Am Board Fam Pract. 13 (2): 111–5. doi:10.3122/15572625-13-2-111. PMID 10764192. S2CID 20016675.
- Koster T, Rosendaal FR, De Ronde H, Briët E, Vandenbroucke JP, Bertina RM (December 1993). "Venous thrombosis due to poor anticoagulant response to activated protein C: Leiden Thrombophilia Study". Lancet. 342 (8886–8887): 1503–6. doi:10.1016/S0140-6736(05)80081-9. ISSN 0140-6736. PMID 7902898. S2CID 54283312.
- Nicolaes GA, Dahlbäck B (2003). "Congenital and acquired activated protein C resistance". Semin Vasc Med. 3 (1): 33–46. doi:10.1055/s-2003-38331. PMID 15199491.