Aphasia
Aphasia is an inability to comprehend or formulate language because of damage to specific brain regions.[1] The major causes are a cerebral vascular accident (stroke) or head trauma. Aphasia can also be the result of brain tumors, brain infections, or neurodegenerative diseases, but the latter are far less prevalent.[2]
| Aphasia | |
|---|---|
| Pronunciation |
|
| Specialty | Neurology, Psychiatry |
| Treatment | Speech therapy |
To be diagnosed with aphasia, a person's speech or language must be significantly impaired in one (or more) of the four aspects of communication following acquired brain injury. Alternately, in the case of progressive aphasia, it must have significantly declined over a short period of time. The four aspects of communication are auditory comprehension, verbal expression, reading and writing, and functional communication.
The difficulties of people with aphasia can range from occasional trouble finding words, to losing the ability to speak, read, or write; intelligence, however, is unaffected.[2] Expressive language and receptive language can both be affected as well. Aphasia also affects visual language such as sign language.[1] In contrast, the use of formulaic expressions in everyday communication is often preserved.[3] For example, while a person with aphasia, particularly Broca's aphasia, may not be able to ask a loved one when their birthday is, they may still be able to sing "Happy Birthday". One prevalent deficit in the aphasias is anomia, which is a difficulty in finding the correct word.[4]:72
With aphasia, one or more modes of communication in the brain have been damaged and are therefore functioning incorrectly. Aphasia is not caused by damage to the brain that results in motor or sensory deficits, which produces abnormal speech; that is, aphasia is not related to the mechanics of speech but rather the individual's language cognition (although a person can have both problems, particularly if they suffered a hemorrhage that damaged a large area of the brain). An individual's "language" is the socially shared set of rules, as well as the thought processes that go behind verbalized speech. It is not a result of a more peripheral motor or sensory difficulty, such as paralysis affecting the speech muscles or a general hearing impairment.
Aphasia affects about 2 million people in the US and 250,000 people in Great Britain.[5] Nearly 180,000 people acquire the disorder every year in the US alone.[6] Any person of any age can develop aphasia, given that it is often caused by a traumatic injury. However, people who are middle aged and older are the most likely to acquire aphasia, as the other etiologies are more likely at older ages.;[7] for example, approximately 75% of all strokes occur in individuals over the age of 65.[8] Strokes account for most documented cases of aphasia:[9] 25% to 40% of people who survive a stroke develop aphasia as a result of damage to the language-processing regions of the brain.[10]
Aphasia and dysphasia
Technically, dysphasia means impaired language and aphasia means lack of language. There have been calls to use the term 'aphasia' regardless of severity. Reasons for doing so include dysphasia being easily confused with the swallowing disorder dysphagia, consumers and speech pathologists preferring the term aphasia, and many languages other than English using a word similar to aphasia.[11] It would appear that the term "aphasia" is more commonly encountered in North America, while "dysphasia" is more frequently found in British literature.[12][13]
Signs and symptoms
People with aphasia may experience any of the following behaviors due to an acquired brain injury, although some of these symptoms may be due to related or concomitant problems, such as dysarthria or apraxia, and not primarily due to aphasia. Aphasia symptoms can vary based on the location of damage in the brain. Signs and symptoms may or may not be present in individuals with aphasia and may vary in severity and level of disruption to communication.[14] Often those with aphasia will try to hide their inability to name objects by using words like thing. So when asked to name a pencil they may say it is a thing used to write.[15]
- Inability to comprehend language
- Inability to pronounce, not due to muscle paralysis or weakness
- Inability to speak spontaneously
- Inability to form words
- Inability to name objects (anomia)
- Poor enunciation
- Excessive creation and use of personal neologisms
- Inability to repeat a phrase
- Persistent repetition of one syllable, word, or phrase (stereotypies, recurrent/recurring utterances/speech automatism)
- Paraphasia (substituting letters, syllables or words)
- Agrammatism (inability to speak in a grammatically correct fashion)
- Dysprosody (alterations in inflexion, stress, and rhythm)
- Incomplete sentences
- Inability to read
- Inability to write
- Limited verbal output
- Difficulty in naming
- Speech disorder
- Speaking gibberish
- Inability to follow or understand simple requests
Related behaviors
Given the previously stated signs and symptoms the following behaviors are often seen in people with aphasia as a result of attempted compensation for incurred speech and language deficits:
- Self-repairs: Further disruptions in fluent speech as a result of mis-attempts to repair erred speech production.[16]
- Speech disfluencies: Include previously mentioned disfluencies including repetitions and prolongations at the phonemic, syllable and word level presenting in pathological/ severe levels of frequency.
- Struggle in non-fluent aphasias: A severe increase in expelled effort to speak after a life where talking and communicating was an ability that came so easily can cause visible frustration.
- Preserved and automatic language: A behavior in which some language or language sequences that were used so frequently, prior to onset, they still possess the ability to produce them with more ease than other language post onset.
- Poor eyesight (Oral Dysmorphia) usually characterized by tingling in the arms and legs, and sometimes heart disorders.[4]:75–76
Subcortical
- Subcortical aphasias characteristics and symptoms depend upon the site and size of subcortical lesion. Possible sites of lesions include the thalamus, internal capsule, and basal ganglia.
Causes
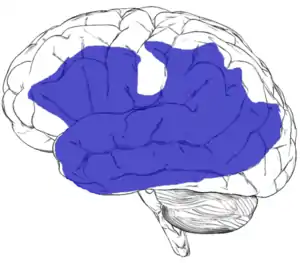
Aphasia is most often caused by stroke, but any disease or damage to the parts of the brain that control language can cause aphasia. Some of these can include brain tumors, traumatic brain injury, and progressive neurological disorders.[18] In rare cases, aphasia may also result from herpesviral encephalitis.[19] The herpes simplex virus affects the frontal and temporal lobes, subcortical structures, and the hippocampal tissue, which can trigger aphasia.[20] In acute disorders, such as head injury or stroke, aphasia usually develops quickly. When caused by brain tumor, infection, or dementia, it develops more slowly.[2][21]
Substantial damage to tissue anywhere within the region shown in blue on the figure which is shown at the right can potentially result in aphasia.[17] Aphasia can also sometimes be caused by damage to subcortical structures deep within the left hemisphere, including the thalamus, the internal and external capsules, and the caudate nucleus of the basal ganglia.[22][23] The area and extent of brain damage or atrophy will determine the type of aphasia and its symptoms.[2][21] A very small number of people can experience aphasia after damage to the right hemisphere only. It has been suggested that these individuals may have had an unusual brain organization prior to their illness or injury, with perhaps greater overall reliance on the right hemisphere for language skills than in the general population.[24][25]
Primary progressive aphasia (PPA), while its name can be misleading, is actually a form of dementia that has some symptoms closely related to several forms of aphasia. It is characterized by a gradual loss in language functioning while other cognitive domains are mostly preserved, such as memory and personality. PPA usually initiates with sudden word-finding difficulties in an individual and progresses to a reduced ability to formulate grammatically correct sentences (syntax) and impaired comprehension. The etiology of PPA is not due to a stroke, traumatic brain injury (TBI), or infectious disease; it is still uncertain what initiates the onset of PPA in those affected by it.[26]
Epilepsy can also include transient aphasia as a prodromal or episodic symptom.[27] Aphasia is also listed as a rare side-effect of the fentanyl patch, an opioid used to control chronic pain.[28]
Classification
Aphasia is best thought of as a collection of different disorders, rather than a single problem. Each individual with aphasia will present with their own particular combination of language strengths and weaknesses. Consequently, it is a major challenge just to document the various difficulties that can occur in different people, let alone decide how they might best be treated. Most classifications of the aphasias tend to divide the various symptoms into broad classes. A common approach is to distinguish between the fluent aphasias (where speech remains fluent, but content may be lacking, and the person may have difficulties understanding others), and the nonfluent aphasias (where speech is very halting and effortful, and may consist of just one or two words at a time).
However, no such broad-based grouping has proven fully adequate. There is wide variation among people even within the same broad grouping, and aphasias can be highly selective. For instance, people with naming deficits (anomic aphasia) might show an inability only for naming buildings, or people, or colors.[29]
It is important to note that there are typical difficulties with speech and language that come with normal aging as well. As we age, language can become more difficult to process resulting in a slowing of verbal comprehension, reading abilities and more likely word finding difficulties. With each of these though, unlike some aphasias, functionality within daily life remains intact.[4]:7
Boston classification
| Type of aphasia | Speech repetition | Naming | Auditory comprehension | Fluency |
|---|---|---|---|---|
| Broca's aphasia | Moderate–severe | Moderate–severe | Mild difficulty | Non-fluent, effortful, slow |
| Wernicke's aphasia | Mild–severe | Mild–severe | Defective | Fluent paraphasic |
| Conduction aphasia | Poor | Poor | Relatively good | Fluent |
| Mixed transcortical aphasia | Moderate | Poor | Poor | Non-fluent |
| Transcortical motor aphasia | Good | Mild–severe | Mild | Non-fluent |
| Transcortical sensory aphasia | Good | Moderate–severe | Poor | Fluent |
| Global aphasia | Poor | Poor | Poor | Non-fluent |
| Anomic aphasia | Mild | Moderate–severe | Mild | Fluent |
- Individuals with Wernicke's' aphasia, also referred to as receptive or fluent aphasia, may speak in long sentences that have no meaning, add unnecessary words, and even create new "words" (neologisms). For example, someone with receptive aphasia may say, "delicious taco", meaning "The dog needs to go out so I will take him for a walk". They have poor auditory and reading comprehension, and fluent, but nonsensical, oral and written expression. Individuals with receptive aphasia usually have great difficulty understanding the speech of both themselves and others and are, therefore, often unaware of their mistakes. Receptive language deficits usually arise from lesions in the posterior portion of the left hemisphere at or near Wernicke's area.[4][32]:71 It is often the result of trauma to the temporal region of the brain, specifically damage to Wernicke's area.[33] Trauma can be the result from an array of problems, however it is most commonly seen as a result of stroke[34]
- Individuals with Broca's aphasia frequently speak short, meaningful phrases that are produced with great effort. It is thus characterized as a nonfluent aphasia. Affected people often omit small words such as "is", "and", and "the". For example, a person with expressive aphasia may say, "walk dog", which could mean "I will take the dog for a walk", "you take the dog for a walk" or even "the dog walked out of the yard". Individuals with expressive aphasia are able to understand the speech of others to varying degrees. Because of this, they are often aware of their difficulties and can become easily frustrated by their speaking problems.[35] While Broca's aphasia may appear to be solely an issue with language production, evidence suggests that Broca's aphasia may be rooted in an inability to process syntactical information.[36] Individuals with Broca's aphasia may have a speech automatism (also called recurring or recurrent utterance. These speech automatisms can be repeated lexical speech automatisms; e.g., modalisations ('I can't..., I can't...'), expletives/swearwords, numbers ('one two, one two') or non-lexical utterances made up of repeated, legal but meaningless, consonant-vowel syllables (e.g.., /tan tan/, /bi bi/). In severe cases the individual may be able to utter only the same speech automatism each time they attempt speech. (examples taken from [Reference for this addition] Code C (1982). "Neurolinguistic analysis of recurrent utterances in aphasia". Cortex. 18 (1): 141–152. doi:10.1016/s0010-9452(82)80025-7. PMID 6197231. S2CID 4487128..)
- Individuals with anomic aphasia have difficulty with naming. People with this aphasia may have difficulties naming certain words, linked by their grammatical type (e.g., difficulty naming verbs and not nouns) or by their semantic category (e.g., difficulty naming words relating to photography but nothing else) or a more general naming difficulty. People tend to produce grammatic, yet empty, speech. Auditory comprehension tends to be preserved. Anomic aphasia is the aphasial presentation of tumors in the language zone; it is the aphasial presentation of Alzheimer's disease.[37] Anomic aphasia is the mildest form of aphasia, indicating a likely possibility for better recovery.[38]
- Individuals with transcortical sensory aphasia, in principle the most general and potentially among the most complex forms of aphasia, may have similar deficits as in receptive aphasia, but their repetition ability may remain intact.
- Global aphasia is considered a severe impairment in many language aspects since it impacts expressive and receptive language, reading, and writing.[39] Despite these many deficits, there is evidence that has shown individuals benefited from speech language therapy.[40] Even though individuals with global aphasia will not become competent speakers, listeners, writers, or readers, goals can be created to improve the individual's quality of life.[35] Individuals with global aphasia usually respond well to treatment that includes personally relevant information, which is also important to consider for therapy.[35]
- Individuals with conduction aphasia have deficits in the connections between the speech-comprehension and speech-production areas. This might be caused by damage to the arcuate fasciculus, the structure that transmits information between Wernicke's area and Broca's area. Similar symptoms, however, can be present after damage to the insula or to the auditory cortex. Auditory comprehension is near normal, and oral expression is fluent with occasional paraphasic errors. Paraphasic errors include phonemic/literal or semantic/verbal. Repetition ability is poor. Conduction and transcortical aphasias are caused by damage to the white matter tracts. These aphasias spare the cortex of the language centers but instead create a disconnection between them. Conduction aphasia is caused by damage to the arcuate fasciculus. The arcuate fasciculus is a white matter tract that connects Broca's and Wernicke's areas. People with conduction aphasia typically have good language comprehension, but poor speech repetition and mild difficulty with word retrieval and speech production. People with conduction aphasia are typically aware of their errors.[35] Two forms of conduction aphasia have been described: reproduction conduction aphasia (repetition of a single relatively unfamiliar multisyllabic word) and repetition conduction aphasia (repetition of unconnected short familiar words [41]
- Transcortical aphasias include transcortical motor aphasia, transcortical sensory aphasia, and mixed transcortical aphasia. People with transcortical motor aphasia typically have intact comprehension and awareness of their errors, but poor word finding and speech production. People with transcortical sensory and mixed transcortical aphasia have poor comprehension and unawareness of their errors.[35] Despite poor comprehension and more severe deficits in some transcortical aphasias, small studies have indicated that full recovery is possible for all types of transcortical aphasia.[42]
Classical-localizationist approaches
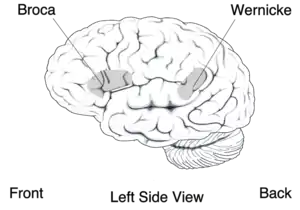
Localizationist approaches aim to classify the aphasias according to their major presenting characteristics and the regions of the brain that most probably gave rise to them.[43][44] Inspired by the early work of nineteenth-century neurologists Paul Broca and Carl Wernicke, these approaches identify two major subtypes of aphasia and several more minor subtypes:
- Expressive aphasia (also known as "motor aphasia" or "Broca's aphasia"), which is characterized by halted, fragmented, effortful speech, but well-preserved comprehension relative to expression. Damage is typically in the anterior portion of the left hemisphere,[45] most notably Broca's area. Individuals with Broca's aphasia often have right-sided weakness or paralysis of the arm and leg, because the left frontal lobe is also important for body movement, particularly on the right side.
- Receptive aphasia (also known as "sensory aphasia" or "Wernicke's aphasia"), which is characterized by fluent speech, but marked difficulties understanding words and sentences. Although fluent, the speech may lack in key substantive words (nouns, verbs, adjectives), and may contain incorrect words or even nonsense words. This subtype has been associated with damage to the posterior left temporal cortex, most notably Wernicke's area. These individuals usually have no body weakness, because their brain injury is not near the parts of the brain that control movement.
- Conduction aphasia, where speech remains fluent, and comprehension is preserved, but the person may have disproportionate difficulty where repeating words or sentences. Damage typically involves the arcuate fasciculus and the left parietal region.[45]
- Transcortical motor aphasia and transcortical sensory aphasia, which are similar to Broca's and Wernicke's aphasia respectively, but the ability to repeat words and sentences is disproportionately preserved.
Recent classification schemes adopting this approach, such as the Boston-Neoclassical Model,[43] also group these classical aphasia subtypes into two larger classes: the nonfluent aphasias (which encompasses Broca's aphasia and transcortical motor aphasia) and the fluent aphasias (which encompasses Wernicke's aphasia, conduction aphasia and transcortical sensory aphasia). These schemes also identify several further aphasia subtypes, including: anomic aphasia, which is characterized by a selective difficulty finding the names for things; and global aphasia, where both expression and comprehension of speech are severely compromised.
Many localizationist approaches also recognize the existence of additional, more "pure" forms of language disorder that may affect only a single language skill.[46] For example, in pure alexia, a person may be able to write but not read, and in pure word deafness, they may be able to produce speech and to read, but not understand speech when it is spoken to them.
Cognitive neuropsychological approaches
Although localizationist approaches provide a useful way of classifying the different patterns of language difficulty into broad groups, one problem is that a sizeable number of individuals do not fit neatly into one category or another.[47][48] Another problem is that the categories, particularly the major ones such as Broca's and Wernicke's aphasia, still remain quite broad. Consequently, even amongst individuals who meet the criteria for classification into a subtype, there can be enormous variability in the types of difficulties they experience.
Instead of categorizing every individual into a specific subtype, cognitive neuropsychological approaches aim to identify the key language skills or "modules" that are not functioning properly in each individual. A person could potentially have difficulty with just one module, or with a number of modules. This type of approach requires a framework or theory as to what skills/modules are needed to perform different kinds of language tasks. For example, the model of Max Coltheart identifies a module that recognizes phonemes as they are spoken, which is essential for any task involving recognition of words. Similarly, there is a module that stores phonemes that the person is planning to produce in speech, and this module is critical for any task involving the production of long words or long strings of speech. Once a theoretical framework has been established, the functioning of each module can then be assessed using a specific test or set of tests. In the clinical setting, use of this model usually involves conducting a battery of assessments,[49][50] each of which tests one or a number of these modules. Once a diagnosis is reached as to the skills/modules where the most significant impairment lies, therapy can proceed to treat these skills.
Progressive aphasias
Primary progressive aphasia (PPA) is a neurodegenerative focal dementia that can be associated with progressive illnesses or dementia, such as frontotemporal dementia / Pick Complex Motor neuron disease, Progressive supranuclear palsy, and Alzheimer's disease, which is the gradual process of progressively losing the ability to think. Gradual loss of language function occurs in the context of relatively well-preserved memory, visual processing, and personality until the advanced stages. Symptoms usually begin with word-finding problems (naming) and progress to impaired grammar (syntax) and comprehension (sentence processing and semantics).<American Speech-Language-Hearing Association> The loss of language before the loss of memory differentiates PPA from typical dementias. People suffering from PPA may have difficulties comprehending what others are saying. They can also have difficulty trying to find the right words to make a sentence.[51][52][53] There are three classifications of Primary Progressive Aphasia : Progressive nonfluent aphasia (PNFA), Semantic Dementia (SD), and Logopenic progressive aphasia (LPA)[53][54]
Progressive Jargon Aphasia is a fluent or receptive aphasia in which the person's speech is incomprehensible, but appears to make sense to them. Speech is fluent and effortless with intact syntax and grammar, but the person has problems with the selection of nouns. Either they will replace the desired word with another that sounds or looks like the original one or has some other connection or they will replace it with sounds. As such, people with jargon aphasia often use neologisms, and may perseverate if they try to replace the words they cannot find with sounds. Substitutions commonly involve picking another (actual) word starting with the same sound (e.g., clocktower - colander), picking another semantically related to the first (e.g., letter - scroll), or picking one phonetically similar to the intended one (e.g., lane - late).
Deaf aphasia
There have been many instances showing that there is a form of aphasia among deaf individuals. Sign languages are, after all, forms of language that have been shown to use the same areas of the brain as verbal forms of language. Mirror neurons become activated when an animal is acting in a particular way or watching another individual act in the same manner. These mirror neurons are important in giving an individual the ability to mimic movements of hands. Broca's area of speech production has been shown to contain several of these mirror neurons resulting in significant similarities of brain activity between sign language and vocal speech communication. Facial communication is a significant portion of how animals interact with each other. Humans use facial movements to create, what other humans perceive, to be faces of emotions. While combining these facial movements with speech, a more full form of language is created which enables the species to interact with a much more complex and detailed form of communication. Sign language also uses these facial movements and emotions along with the primary hand movement way of communicating. These facial movement forms of communication come from the same areas of the brain. When dealing with damages to certain areas of the brain, vocal forms of communication are in jeopardy of severe forms of aphasia. Since these same areas of the brain are being used for sign language, these same, at least very similar, forms of aphasia can show in the Deaf community. Individuals can show a form of Wernicke's aphasia with sign language and they show deficits in their abilities in being able to produce any form of expressions. Broca's aphasia shows up in some people, as well. These individuals find tremendous difficulty in being able to actually sign the linguistic concepts they are trying to express.[55]
Severity
The severity of the type of aphasia varies depending on the size of the stroke. However, there is much variance between how often one type of severity occurs in certain types of aphasia. For instance, any type of aphasia can range from mild to profound. Regardless of the severity of aphasia, people can make improvements due to spontaneous recovery and treatment in the acute stages of recovery.[56] Additionally, while most studies propose that the greatest outcomes occur in people with severe aphasia when treatment is provided in the acute stages of recovery, Robey (1998) also found that those with severe aphasia are capable of making strong language gains in the chronic stage of recovery as well.[56] This finding implies that persons with aphasia have the potential to have functional outcomes regardless of how severe their aphasia may be.[56] While there is no distinct pattern of the outcomes of aphasia based on severity alone, global aphasia typically makes functional language gains, but may be gradual since global aphasia affects many language areas.
Cognitive deficits in aphasia
While aphasia has traditionally been described in terms of language deficits, there is increasing evidence that many people with aphasia commonly experience co-occurring non-linguistic cognitive deficits.[57] By some accounts, cognitive deficits, such as attention and working memory constitute the underlying cause of language impairment in people with aphasia.[58] Others suggest that cognitive deficits often co-occur but are comparable to cognitive deficits in stroke patients without aphasia and reflect general brain dysfunction following injury.[59] The degree to which deficits in attention and other cognitive domains underlie language deficits in aphasia is still unclear.[60]
In particular, people with aphasia often demonstrate short-term and working memory deficits.[57] These deficits can occur in both the verbal domain[61][62] as well as the visuospatial domain.[63] Furthermore, these deficits are often associated with performance on language specific tasks such as naming, lexical processing, and sentence comprehension, and discourse production.[64][57][65][66] Other studies have found that most, but not all people with aphasia demonstrate performance deficits on tasks of attention, and their performance on these tasks correlate with language performance and cognitive ability in other domains.[57] Even patients with mild aphasia, who score near the ceiling on tests of language often demonstrate slower response times and interference effects in non-verbal attention abilities.[67]
In addition to deficits in short-term memory, working memory, and attention, people with aphasia can also demonstrate deficits in executive function.[68] For instance, people with aphasia may demonstrate deficits in initiation, planning, self-monitoring, and cognitive flexibility.[69] Other studies have found that people with aphasia demonstrate reduced speed and efficiency during completion executive function assessments.[70]
Regardless of their role in the underlying nature of aphasia, cognitive deficits have a clear role in the study and rehabilitation of aphasia. For instance, the severity of cognitive deficits in people with aphasia has been associated with lower quality of life, even more so than the severity of language deficits.[71] Furthermore, cognitive deficits may influence language treatment outcomes in aphasia.[72][73] Non-linguistic cognitive deficits have also been the target of interventions directed at improving language ability, though outcomes are not definitive.[74] While some studies have demonstrated language improvement secondary to cognitively-focused treatment,[75] others have found little evidence that the treatment of cognitive deficits in people with aphasia has an influence on language outcomes.[76]
One important caveat in the measurement and treatment of cognitive deficits in people with aphasia is the degree to which assessments of cognition rely on language abilities for successful performance.[77] Most studies have attempted to circumvent this challenge by utilizing non-verbal cognitive assessments to evaluate cognitive ability in people with aphasia. However, the degree to which these tasks are truly ‘non-verbal’ and not mediated by language in unclear.[60] For instance, Wall et al.[64] found that language and non-linguistic performance was related, except when non-linguistic performance was measured by ‘real life’ cognitive tasks.
Prevention of aphasia
Aphasia is largely caused by unavoidable instances. However, some precautions can be taken to decrease risk for experiencing one of the two major causes of aphasia: stroke and traumatic brain injury (TBI). To decrease the probability of having an ischemic or hemorrhagic stroke, one should take the following precautions:
- Exercising regularly
- Eating a healthy diet, avoiding cholesterol in particular
- Keeping alcohol consumption low and avoiding tobacco use
- Controlling blood pressure[78]
- Going to the emergency room immediately if you begin to experience unilateral extremity (especially leg) swelling, warmth, redness, and/or tenderness as these are symptoms of a deep vein thrombosis which can lead to a stroke.[79]
To prevent aphasia due to traumatic injury, one sure take precautionary measures when engaging in dangerous activities such as:
- Wearing a helmet when operating a bicycle, motor cycle, ATV, or any other moving vehicle that could potential be involved in an accident.
- Wearing a seatbelt when driving or riding in a car.
- Wearing proper protective gear when playing contact sports, especially American football, rugby, and hockey, or refraining from such activities.
- Minimizing anticoagulant use (including aspirin) if at all possible as they increase the risk of hemorrhage after a head injury.[80]
Additionally, one should always seek medical attention after sustaining head trauma due to a fall or accident. The sooner that one receives medical attention for a traumatic brain injury, the less likely one is to experience long-term or severe effects.[81]
Management
When addressing Wernicke's aphasia, according to Bakheit et al. (2007), the lack of awareness of the language impairments, a common characteristic of Wernicke's aphasia, may affect the rate and extent of therapy outcomes.[82] Robey (1998) determined that at least 2 hours of treatment per week is recommended for making significant language gains.[56] Spontaneous recovery may cause some language gains, but without speech-language therapy, the outcomes can be half as strong as those with therapy.[56]
When addressing Broca's aphasia, better outcomes occur when the person participates in therapy, and treatment is more effective than no treatment for people in the acute period.[56] Two or more hours of therapy per week in acute and post-acute stages produced the greatest results.[56] High-intensity therapy was most effective, and low-intensity therapy was almost equivalent to no therapy.[56]
People with global aphasia are sometimes referred to as having irreversible aphasic syndrome, often making limited gains in auditory comprehension, and recovering no functional language modality with therapy. With this said, people with global aphasia may retain gestural communication skills that may enable success when communicating with conversational partners within familiar conditions. Process-oriented treatment options are limited, and people may not become competent language users as readers, listeners, writers, or speakers no matter how extensive therapy is.[35] However, people's daily routines and quality of life can be enhanced with reasonable and modest goals.[35] After the first month, there is limited to no healing to language abilities of most people. There is a grim prognosis leaving 83% who were globally aphasic after the first month they will remain globally aphasic at the first year. Some people are so severely impaired that their existing process-oriented treatment approaches offer signs of progress, and therefore cannot justify the cost of therapy.[35]
Perhaps due to the relative rareness of conduction aphasia, few studies have specifically studied the effectiveness of therapy for people with this type of aphasia. From the studies performed, results showed that therapy can help to improve specific language outcomes. One intervention that has had positive results is auditory repetition training. Kohn et al. (1990) reported that drilled auditory repetition training related to improvements in spontaneous speech, Francis et al. (2003) reported improvements in sentence comprehension, and Kalinyak-Fliszar et al. (2011) reported improvements in auditory-visual short-term memory.[83][84][85]
Most acute cases of aphasia recover some or most skills by working with a speech-language pathologist. Recovery and improvement can continue for years after the stroke. After the onset of Aphasia, there is approximately a six-month period of spontaneous recovery; during this time, the brain is attempting to recover and repair the damaged neurons. Improvement varies widely, depending on the aphasia's cause, type, and severity. Recovery also depends on the person's age, health, motivation, handedness, and educational level.[21]
There is no one treatment proven to be effective for all types of aphasias. The reason that there is no universal treatment for aphasia is because of the nature of the disorder and the various ways it is presented, as explained in the above sections. Aphasia is rarely exhibited identically, implying that treatment needs to be catered specifically to the individual. Studies have shown that, although there is no consistency on treatment methodology in literature, there is a strong indication that treatment, in general, has positive outcomes.[86] Therapy for aphasia ranges from increasing functional communication to improving speech accuracy, depending on the person's severity, needs and support of family and friends.[87] Group therapy allows individuals to work on their pragmatic and communication skills with other individuals with aphasia, which are skills that may not often be addressed in individual one-on-one therapy sessions. It can also help increase confidence and social skills in a comfortable setting.[4]:97
Evidence does not support the use of transcranial direct current stimulation (tDCS) for improving aphasia after stroke. Moderate quality evidence does indicate naming performance improvements for nouns but not verbs using tDCS[88]
Specific treatment techniques include the following:
- Copy and recall therapy (CART) - repetition and recall of targeted words within therapy may strengthen orthographic representations and improve single word reading, writing, and naming[89]
- Visual communication therapy (VIC) - the use of index cards with symbols to represent various components of speech
- Visual action therapy (VAT) - typically treats individuals with global aphasia to train the use of hand gestures for specific items[90]
- Functional communication treatment (FCT) - focuses on improving activities specific to functional tasks, social interaction, and self-expression
- Promoting aphasic's communicative effectiveness (PACE) - a means of encouraging normal interaction between people with aphasia and clinicians. In this kind of therapy, the focus is on pragmatic communication rather than treatment itself. People are asked to communicate a given message to their therapists by means of drawing, making hand gestures or even pointing to an object[91]
- Melodic intonation therapy (MIT) - aims to use the intact melodic/prosodic processing skills of the right hemisphere to help cue retrieval of words and expressive language[4]:93
- Other - i.e. drawing as a way of communicating, trained conversation partners[86]
Semantic feature analysis (SFA) -a type of aphasia treatment that targets word-finding deficits. It is based on the theory that neural connections can be strengthened by using related words and phrases that are similar to the target word, to eventually activate the target word in the brain. SFA can be implemented in multiple forms such as verbally, written, using picture cards, etc. The SLP provides prompting questions to the individual with aphasia in order for the person to name the picture provided.[92] Studies show that SFA is an effective intervention for improving confrontational naming.[93]
Melodic intonation therapy is used to treat non-fluent aphasia and has proved to be effective in some cases.[94] However, there is still no evidence from randomized controlled trials confirming the efficacy of MIT in chronic aphasia. MIT is used to help people with aphasia vocalize themselves through speech song, which is then transferred as a spoken word. Good candidates for this therapy include people who have had left hemisphere strokes, non-fluent aphasias such as Broca's, good auditory comprehension, poor repetition and articulation, and good emotional stability and memory.[95] An alternative explanation is that the efficacy of MIT depends on neural circuits involved in the processing of rhythmicity and formulaic expressions (examples taken from the MIT manual: “I am fine,” “how are you?” or “thank you”); while rhythmic features associated with melodic intonation may engage primarily left-hemisphere subcortical areas of the brain, the use of formulaic expressions is known to be supported by right-hemisphere cortical and bilateral subcortical neural networks.[3][96]
Systematic reviews support the effectiveness and importance of partner training.[97] According to the National Institute on Deafness and Other Communication Disorders (NIDCD), involving family with the treatment of an aphasic loved one is ideal for all involved, because while it will no doubt assist in their recovery, it will also make it easier for members of the family to learn how best to communicate with them.[98]
When a person's speech is insufficient, different kinds of augmentative and alternative communication could be considered such as alphabet boards, pictorial communication books, specialized software for computers or apps for tablets or smartphones.[99]
Intensity of treatment
The intensity of aphasia therapy is determined by the length of each session, total hours of therapy per week, and total weeks of therapy provided. There is no consensus about what "intense" aphasia therapy entails, or how intense therapy should be to yield the best outcomes. A 2016 Cochrane review of speech and language therapy for people with aphasia found that treatments that are higher intensity, higher dose or over a long duration of time led to significantly better functional communication but people were more likely to drop out of high intensity treatment (up to 15 hours per week).[100]
Intensity of therapy is also dependent on the recency of stroke. People with aphasia react differently to intense treatment in the acute phase (0–3 months post stroke), sub-acute phase (3–6 months post stroke), or chronic phase (6+ months post stroke). Intensive therapy has been found to be effective for people with nonfluent and fluent chronic aphasia, but less effective for people with acute aphasia.[101]> People with sub-acute aphasia also respond well to intensive therapy of 100 hours over 62 weeks. This suggests people in the sub-acute phase can improve greatly in language and functional communication measures with intensive therapy compared to regular therapy.[101]
Individualized service delivery
Intensity of treatment should be individualized based on the recency of stroke, therapy goals, and other specific characteristics such as age, size of lesion, overall health status, and motivation.[101][102] Each individual reacts differently to treatment intensity and is able to tolerate treatment at different times post-stroke.[102] Intensity of treatment after a stroke should be dependent on the person's motivation, stamina, and tolerance for therapy.[103]
Outcomes
If the symptoms of aphasia last longer than two or three months after a stroke, a complete recovery is unlikely. However, it is important to note that some people continue to improve over a period of years and even decades. Improvement is a slow process that usually involves both helping the individual and family understand the nature of aphasia and learning compensatory strategies for communicating.[104]
After a traumatic brain injury (TBI) or cerebrovascular accident (CVA), the brain undergoes several healing and re-organization processes, which may result in improved language function. This is referred to as spontaneous recovery. Spontaneous recovery is the natural recovery the brain makes without treatment, and the brain begins to reorganize and change in order to recover.[35] There are several factors that contribute to a person's chance of recovery caused by stroke, including stroke size and location.[105] Age, sex, and education have not been found to be very predictive.[105]
Specific to aphasia, spontaneous recovery varies among affected people and may not look the same in everyone, making it difficult to predict recovery.[105]
Though some cases of Wernicke's aphasia have shown greater improvements than more mild forms of aphasia, people with Wernicke's aphasia may not reach as high a level of speech abilities as those with mild forms of aphasia.[106]
History
The first recorded case of aphasia is from an Egyptian papyrus, the Edwin Smith Papyrus, which details speech problems in a person with a traumatic brain injury to the temporal lobe.[107]
During the second half of the 19th century, aphasia was a major focus for scientists and philosophers who were working in the beginning stages of the field of psychology.[1] In medical research, speechlessness was described as an incorrect prognosis, and there was no assumption that underlying language complications existed.[108] Broca and his colleagues were some of the first to write about aphasia, but Wernicke was the first credited to have written extensively about aphasia being a disorder that contained comprehension difficulties.[109] Despite claims of who reported on aphasia first, it was F.J. Gall that gave the first full description of aphasia after studying wounds to the brain, as well as his observation of speech difficulties resulting from vascular lesions.[110] A recent book on the entire history of aphasia is available (Reference: Tesak, J. & Code, C. (2008) Milestones in the History of Aphasia: Theories and Protagonists. Hove, East Sussex: Psychology Press).
Further research
Research is currently being done using functional magnetic resonance imaging (fMRI) to witness the difference in how language is processed in normal brains vs aphasic brains. This will help researchers to understand exactly what the brain must go through in order to recover from Traumatic Brain Injury (TBI) and how different areas of the brain respond after such an injury.
Another intriguing approach being tested is that of drug therapy. Research is in progress that will hopefully uncover whether or not certain drugs might be used in addition to speech-language therapy in order to facilitate recovery of proper language function. It's possible that the best treatment for Aphasia might involve combining drug treatment with therapy, instead of relying on one over the other.
One other method being researched as a potential therapeutic combination with speech-language therapy is brain stimulation. One particular method, Transcranial Magnetic Stimulation (TMS), alters brain activity in whatever area it happens to stimulate, which has recently led scientists to wonder if this shift in brain function caused by TMS might help people re-learn languages.
The research being put into Aphasia has only just begun. Researchers appear to have multiple ideas on how Aphasia could be more effectively treated in the future.[98]
See also
References
- Damasio AR (February 1992). "Aphasia". The New England Journal of Medicine. 326 (8): 531–9. doi:10.1056/NEJM199202203260806. PMID 1732792.
- "American Speech-Language-Hearing Association (ASHA):- Aphasia". asha.org.
- Stahl B, Van Lancker Sidtis D (2015). "Tapping into neural resources of communication: formulaic language in aphasia therapy". Frontiers in Psychology. 6 (1526): 1526. doi:10.3389/fpsyg.2015.01526. PMC 4611089. PMID 26539131.
- Manasco MH (2014). Introduction to Neurogenic Communication Disorders. Burlington, MA: Jones & Bartlett Learning. ISBN 978-1-4496-5244-9.
- "Aphasia Statistics".
- "Aphasia Fact sheet - National Aphasia Association". National Aphasia Association. Retrieved 18 December 2017.
- "Aphasia: Who is at risk for aphasia?".
- "Stroke Statistics".
- "Aphasia FAQ".
- "An overview of aphasia".
- Worrall, Linda; Simmons-Mackie, Nina; Wallace, Sarah J; Rose, Tanya; Brady, Marian C; Kong, Anthony Pak Hin; Murray, Laura; Hallowell, Brooke (2016). "Let's call it "aphasia": Rationales for eliminating the term "dysphasia"". International Journal of Stroke. 11 (8): 848–851. doi:10.1177/1747493016654487. ISSN 1747-4930. PMID 27384070. S2CID 28020306.
- "What's the difference between aphasia, dysphasia and dysarthria?". Touch Type Read & Spell. Retrieved 24 March 2020.
- "What is Dysphasia?". Healthline. Retrieved 24 March 2020.
- American Speech-Language-Hearing Association (1997-2014)
- Nolen-Hoeksema, S. (2014). Neurodevelopmental and Neurocognitive Disorders. In Abnormal Psychology (6th ed.). New York: McGraw-Hill.
- Middleton EL, Schwartz MF, Brecher A, Gagliardi M, Garvey K (2016). "Does naming accuracy improve through self-monitoring of errors?". Neuropsychologia. 84: 272–281. doi:10.1016/j.neuropsychologia.2016.01.027. PMC 4826482. PMID 26863091.
- Henseler I, Regenbrecht F, Obrig H (March 2014). "Lesion correlates of patholinguistic profiles in chronic aphasia: comparisons of syndrome-, modality- and symptom-level assessment". Brain. 137 (Pt 3): 918–30. doi:10.1093/brain/awt374. PMID 24525451.
- "Aphasia". www.asha.org. Retrieved 2015-11-18.
- Soares-Ishigaki EC, Cera ML, Pieri A, Ortiz KZ (2012). "Aphasia and herpes virus encephalitis: a case study". Sao Paulo Medical Journal. 130 (5): 336–41. doi:10.1590/S1516-31802012000500011. PMID 23174874.
- Naudé H, Pretorius E (3 Jun 2010). "Can herpes simplex virus encephalitis cause aphasia?". Early Child Development and Care. 173 (6): 669–679. doi:10.1080/0300443032000088285. S2CID 143811627.
- "Aphasia". MedicineNet.com. Retrieved 2011-05-23.
- Kuljic-Obradovic DC (July 2003). "Subcortical aphasia: three different language disorder syndromes?". European Journal of Neurology. 10 (4): 445–8. doi:10.1046/j.1468-1331.2003.00604.x. PMID 12823499. S2CID 19945519.
- Kreisler A, Godefroy O, Delmaire C, Debachy B, Leclercq M, Pruvo JP, Leys D (March 2000). "The anatomy of aphasia revisited". Neurology. 54 (5): 1117–23. doi:10.1212/wnl.54.5.1117. PMID 10720284. S2CID 21847976.
- Coppens P, Hungerford S, Yamaguchi S, Yamadori A (December 2002). "Crossed aphasia: an analysis of the symptoms, their frequency, and a comparison with left-hemisphere aphasia symptomatology". Brain and Language. 83 (3): 425–63. doi:10.1016/s0093-934x(02)00510-2. PMID 12468397. S2CID 46650843.
- Mariën P, Paghera B, De Deyn PP, Vignolo LA (February 2004). "Adult crossed aphasia in dextrals revisited". Cortex; A Journal Devoted to the Study of the Nervous System and Behavior. 40 (1): 41–74. doi:10.1016/s0010-9452(08)70920-1. PMID 15070002. S2CID 4481435.
- "Primary Progressive Aphasia". www.asha.org. Retrieved 2015-11-15.
- Blumenfeld H, Meador KJ (August 2014). "Consciousness as a useful concept in epilepsy classification". Epilepsia. 55 (8): 1145–50. doi:10.1111/epi.12588. PMC 4149314. PMID 24981294.
- "Fentanyl Transdermal Official FDA information, side effects and uses". Drug Information Online.
- Kolb, Bryan; Whishaw, Ian Q. (2003). Fundamentals of human neuropsychology. [New York]: Worth. pp. 502, 505, 511. ISBN 978-0-7167-5300-1. OCLC 464808209.
- "What is Aphasia". Atlanta Aphasia Association. 2006. Retrieved 2008-12-01.
- Murdoch BE (1990). "Bostonian and Lurian aphasia syndromes". Acquired Speech and Language Disorders. Springer, Boston, MA. pp. 60–96. doi:10.1007/978-1-4899-3458-1_2. ISBN 9780412334405.
- DeWitt I, Rauschecker JP (November 2013). "Wernicke's area revisited: parallel streams and word processing". Brain and Language. 127 (2): 181–91. doi:10.1016/j.bandl.2013.09.014. PMC 4098851. PMID 24404576.
- "Aphasia". NIDCD. 2015-08-18. Retrieved 2017-05-02.
- "Common Classifications of Aphasia". www.asha.org. Retrieved 2017-05-02.
- Brookshire R. "Introduction to neurogenic communication disorders (7th edition). St. Louis, MO: Mosby". Cite journal requires
|journal=(help) - Embick D, Marantz A, Miyashita Y, O'Neil W, Sakai KL (2000). "A syntactic specialization for Broca's area". Proceedings of the National Academy of Sciences of the United States of America. 97 (11): 6150–4. doi:10.1073/pnas.100098897. PMC 18573. PMID 10811887.CS1 maint: multiple names: authors list (link)
- Alexander MP, Hillis AE (2008). Georg Goldenberg, Bruce L Miller, Michael J Aminoff, Francois Boller, D F Swaab (eds.). Aphasia. Handbook of Clinical Neurology. 88 (1 ed.). pp. 287–310. doi:10.1016/S0072-9752(07)88014-6. ISBN 9780444518972. OCLC 733092630. PMID 18631697.
- Squire LR; Dronkers NF; Baldo JV (2009). "Encyclopedia of neuroscience". Cite journal requires
|journal=(help) - Demeurisse G.; Capon A. (1987). "Language recovery in aphasic stroke patients: Clinical, CT and CBF studies". Aphasiology. 1 (4): 301–315. doi:10.1080/02687038708248851.
- Basso A, Macis M (2001). "Therapy efficacy in chronic aphasia". Behavioural Neurology. 24 (4): 317–25. doi:10.1155/2011/313480. PMC 5377972. PMID 22063820.
- Shallice, Tim; Warrington, Elizabeth K. (October 1977). "Auditory-verbal short-term memory impairment and conduction aphasia". Brain and Language. 4 (4): 479–491. doi:10.1016/0093-934x(77)90040-2. ISSN 0093-934X. PMID 922463. S2CID 40665691.
- Flamand-Roze C, Cauquil-Michon C, Roze E, Souillard-Scemama R, Maintigneux L, Ducreux D, et al. (December 2011). "Aphasia in border-zone infarcts has a specific initial pattern and good long-term prognosis". European Journal of Neurology. 18 (12): 1397–401. doi:10.1111/j.1468-1331.2011.03422.x. PMID 21554494. S2CID 26120952.
- Goodglass, H., Kaplan, E., & Barresi, B. (2001). The assessment of aphasia and related disorders. Lippincott Williams & Wilkins.
- Kertesz, A. (2006). Western Aphasia Battery-Revised (WAB-R). Austin, TX: Pro-Ed.
- "Common Classifications of Aphasia". www.asha.org. Retrieved 2015-11-19.
- Kolb, Bryan; Whishaw, Ian Q. (2003). Fundamentals of human neuropsychology. [New York]: Worth. pp. 502–504. ISBN 978-0-7167-5300-1. OCLC 464808209.
- Godefroy O, Dubois C, Debachy B, Leclerc M, Kreisler A (March 2002). "Vascular aphasias: main characteristics of patients hospitalized in acute stroke units". Stroke. 33 (3): 702–5. doi:10.1161/hs0302.103653. PMID 11872891.
- Ross K.B.; Wertz R.T. (2001). "Type and severity of aphasia during the first seven months poststroke". Journal of Medical Speech-Language Pathology. 9: 31–53.
- Coltheart, Max; Kay, Janice; Lesser, Ruth (1992). PALPA psycholinguistic assessments of language processing in aphasia. Hillsdale, N.J: Lawrence Erlbaum Associates. ISBN 978-0-86377-166-8.
- Porter, G., & Howard, D. (2004). CAT: comprehensive aphasia test. Psychology Press.
- Mesulam MM (April 2001). "Primary progressive aphasia". Annals of Neurology. 49 (4): 425–32. doi:10.1002/ana.91. PMID 11310619. S2CID 35528862.
- Wilson SM, Henry ML, Besbris M, Ogar JM, Dronkers NF, Jarrold W, et al. (July 2010). "Connected speech production in three variants of primary progressive aphasia". Brain. 133 (Pt 7): 2069–88. doi:10.1093/brain/awq129. PMC 2892940. PMID 20542982.
- Harciarek M, Kertesz A (September 2011). "Primary progressive aphasias and their contribution to the contemporary knowledge about the brain-language relationship". Neuropsychology Review. 21 (3): 271–87. doi:10.1007/s11065-011-9175-9. PMC 3158975. PMID 21809067.
- Gorno-Tempini ML, Hillis AE, Weintraub S, Kertesz A, Mendez M, Cappa SF, et al. (March 2011). "Classification of primary progressive aphasia and its variants". Neurology. 76 (11): 1006–14. doi:10.1212/WNL.0b013e31821103e6. PMC 3059138. PMID 21325651.
- Carlson N (2013). Physiology of Behavior. New York: Pearson. pp. 494–496.
- Robey RR (February 1998). "A meta-analysis of clinical outcomes in the treatment of aphasia". Journal of Speech, Language, and Hearing Research. 41 (1): 172–87. doi:10.1044/jslhr.4101.172. PMID 9493743.
- Murray LL (May 2012). "Attention and Other Cognitive Deficits in Aphasia: Presence and Relation to Language and Communication Measures" (PDF). American Journal of Speech-Language Pathology. 21 (2): S51-64. doi:10.1044/1058-0360(2012/11-0067). ISSN 1058-0360. PMID 22230179.
- Hula WD, McNeil MR (August 2008). "Models of attention and dual-task performance as explanatory constructs in aphasia". Seminars in Speech and Language. 29 (3): 169–87, quiz C 3–4. doi:10.1055/s-0028-1082882. PMID 18720315.
- Fonseca J, Raposo A, Martins IP (March 2018). "Cognitive performance and aphasia recovery". Topics in Stroke Rehabilitation. 25 (2): 131–136. doi:10.1080/10749357.2017.1390904. PMID 29072540. S2CID 3884877.
- Villard S, Kira n S (2017-10-03). "To what extent does attention underlie language in aphasia?". Aphasiology. 31 (10): 1226–1245. doi:10.1080/02687038.2016.1242711. S2CID 151445078.
- Martin N, Ayala J (June 2004). "Measurements of auditory-verbal STM span in aphasia: effects of item, task, and lexical impairment". Brain and Language. 89 (3): 464–83. doi:10.1016/j.bandl.2003.12.004. PMID 15120538. S2CID 11497057.
- Laures-Gore J, Marshall RS, Verner E (January 2011). "Performance of Individuals with Left-Hemisphere Stroke and Aphasia and Individuals with Right Brain Damage on Forward and Backward Digit Span Tasks". Aphasiology. 25 (1): 43–56. doi:10.1080/02687031003714426. PMC 3090622. PMID 21572584.
- Kasselimis DS, Simos PG, Economou A, Peppas C, Evdokimidis I, Potagas C (August 2013). "Are memory deficits dependent on the presence of aphasia in left brain damaged patients?". Neuropsychologia. 51 (9): 1773–6. doi:10.1016/j.neuropsychologia.2013.06.003. PMID 23770384. S2CID 14620782.
- Wall KJ, Cumming TB, Copland DA (2017-05-05). "Determining the Association between Language and Cognitive Tests in Poststroke Aphasia". Frontiers in Neurology. 8: 149. doi:10.3389/fneur.2017.00149. PMC 5418218. PMID 28529495.
- Cahana-Amitay D, Jenkins T (November 2018). "Working memory and discourse production in people with aphasia 6". Journal of Neurolinguistics. 48: 90–103. doi:10.1016/j.jneuroling.2018.04.007. S2CID 53183275.
- Minkina I, Martin N, Spencer KA, Kendall DL (March 2018). "Links Between Short-Term Memory and Word Retrieval in Aphasia". American Journal of Speech-Language Pathology. 27 (1S): 379–391. doi:10.1044/2017_AJSLP-16-0194. PMC 6111490. PMID 29497750.
- Hunting-Pompon R, Kendall D, Bacon Moore A (June 2011). "Examining attention and cognitive processing in participants with self-reported mild anomia". Aphasiology. 25 (6–7): 800–812. doi:10.1080/02687038.2010.542562. S2CID 145763896.
- Murray LL, Ramage AE (2000). "Assessing the executive function abilities of adults with neurogenic communication disorders". Seminars in Speech and Language. 21 (2): 153–67, quiz 168. doi:10.1055/s-2000-7562. PMID 10879547.
- Murray LL (2017-07-03). "Design fluency subsequent to onset of aphasia: a distinct pattern of executive function difficulties?". Aphasiology. 31 (7): 793–818. doi:10.1080/02687038.2016.1261248. ISSN 0268-7038. S2CID 151808957.
- Purdy M (April 2002). "Executive function ability in persons with aphasia". Aphasiology. 16 (4–6): 549–557. doi:10.1080/02687030244000176. ISSN 0268-7038. S2CID 144618814.
- Nicholas M, Hunsaker E, Guarino AJ (2017-06-03). "The relation between language, non-verbal cognition and quality of life in people with aphasia". Aphasiology. 31 (6): 688–702. doi:10.1080/02687038.2015.1076927. S2CID 146960778.
- Dignam J, Copland D, O'Brien K, Burfein P, Khan A, Rodriguez AD (February 2017). "Influence of Cognitive Ability on Therapy Outcomes for Anomia in Adults With Chronic Poststroke Aphasia" (PDF). Journal of Speech, Language, and Hearing Research. 60 (2): 406–421. doi:10.1044/2016_JSLHR-L-15-0384. PMID 28199471.
- Lambon Ralph MA, Snell C, Fillingham JK, Conroy P, Sage K (April 2010). "Predicting the outcome of anomia therapy for people with aphasia post CVA: both language and cognitive status are key predictors". Neuropsychological Rehabilitation. 20 (2): 289–305. doi:10.1080/09602010903237875. PMID 20077315. S2CID 23062509.
- Murray LL, Keeton RJ, Karcher L (January 2006). "Treating attention in mild aphasia: evaluation of attention process training-II". Journal of Communication Disorders. 39 (1): 37–61. doi:10.1016/j.jcomdis.2005.06.001. PMID 16039661.
- Peach RK, Beck KM, Gorman M, Fisher C (August 2019). "Clinical Outcomes Following Language-Specific Attention Treatment Versus Direct Attention Training for Aphasia: A Comparative Effectiveness Study". Journal of Speech, Language, and Hearing Research. 62 (8): 2785–2811. doi:10.1044/2019_JSLHR-L-18-0504. PMID 31348732.
- Nouwens F, de Lau LM, Visch-Brink EG, van de Sandt-Koenderman WM, Lingsma HF, Goosen S, et al. (June 2017). "Efficacy of early cognitive-linguistic treatment for aphasia due to stroke: A randomised controlled trial (Rotterdam Aphasia Therapy Study-3)". European Stroke Journal. 2 (2): 126–136. doi:10.1177/2396987317698327. PMC 5992741. PMID 29900407.
- Mayer JF, Murray LL (September 2012). "Measuring working memory deficits in aphasia". Journal of Communication Disorders. 45 (5): 325–39. doi:10.1016/j.jcomdis.2012.06.002. PMID 22771135.
- "What is aphasia? What causes aphasia?". Medical News Today.
- "DVT (Deep Vein Thrombosis Blood Clot in the Leg)".
- Albrecht, Jennifer S.; Liu, Xinggang; Baumgarten, Mona; Langenberg, Patricia; Rattinger, Gail B.; Smith, Gordon S.; Gambert, Steven R.; Gottlieb, Stephen S.; Zuckerman, Ilene H. (2014). "Benefits and Risks of Anticoagulation Resumption Following Traumatic Brain Injury". JAMA Internal Medicine. 174 (8): 1244–51. doi:10.1001/jamainternmed.2014.2534. PMC 4527047. PMID 24915005.
- "Causes and effects of traumatic brain injuries".
- Bakheit AM, Shaw S, Carrington S, Griffiths S (October 2007). "The rate and extent of improvement with therapy from the different types of aphasia in the first year after stroke". Clinical Rehabilitation. 21 (10): 941–9. doi:10.1177/0269215507078452. PMID 17981853. S2CID 25995618.
- Kalinyak-Fliszar M, Kohen F, Martin N (January 2011). "Remediation of language processing in aphasia: Improving activation and maintenance of linguistic representations in (verbal) short-term memory". Aphasiology. 25 (10): 1095–1131. doi:10.1080/02687038.2011.577284. PMC 3393127. PMID 22791930.
- Francis D, Clark N, Humphreys G (2003). "The treatment of an auditory working memory deficit and the implications for sentence comprehension abilities in mild 'receptive' aphasia". Aphasiology. 17 (8): 723–50. doi:10.1080/02687030344000201. S2CID 145088109.
- Kohn SE, Smith KL, Arsenault JK (April 1990). "The remediation of conduction aphasia via sentence repetition: a case study". The British Journal of Disorders of Communication. 25 (1): 45–60. doi:10.3109/13682829009011962. PMID 1695853.
- Schmitz, Thomas J.; O'Sullivan, Susan B. (2007). Physical rehabilitation. Philadelphia: F.A. Davis. ISBN 978-0-8036-1247-1. OCLC 70119705.
- "Aphasia". asha.org.
- Elsner, Bernhard; Kugler, Joachim; Pohl, Marcus; Mehrholz, Jan (21 May 2019). "Transcranial direct current stimulation (tDCS) for improving aphasia in adults with aphasia after stroke". The Cochrane Database of Systematic Reviews. 5: CD009760. doi:10.1002/14651858.CD009760.pub4. ISSN 1469-493X. PMC 6528187. PMID 31111960.
- Beeson, P. M., Egnor, H. (2007), Combining treatment for written and spoken naming, Journal of the International Neuropsychological Society, 12(6); 816-827.
- "Aphasia". American Speech Language Hearing Association. Retrieved from http://www.asha.org/PRPSpecificTopic.aspx?folderid=8589934663§ion=Treatment
- Alexander MT, Hillis AE (2008). "Aphasia". In Goldenberg G, Miller BL, Aminoff MJ, Boller F, Swaab DF (eds.). Neuropsychology and Behavioral Neurology: Handbook of Clinical Neurology. 88. Elsevier Health Sciences. pp. 287–310. ISBN 978-0-444-51897-2. OCLC 733092630.
- Davis , Stanton (2005). "Semantic Feature Analysis as a Functional Therapy Tool". Contemporary Issues in Communication Science and Disorders. 35: 85–92. doi:10.1044/cicsd_32_F_85.
- Maddy KM, Capilouto GJ, McComas KL (June 2014). "The effectiveness of semantic feature analysis: an evidence-based systematic review". Annals of Physical and Rehabilitation Medicine. 57 (4): 254–67. doi:10.1016/j.rehab.2014.03.002. PMID 24797214.
- Norton A, Zipse L, Marchina S, Schlaug G (July 2009). "Melodic intonation therapy: shared insights on how it is done and why it might help". Annals of the New York Academy of Sciences. 1169: 431–6. doi:10.1111/j.1749-6632.2009.04859.x. PMC 2780359. PMID 19673819.
- van der Meulen I, van de Sandt-Koenderman ME, Ribbers GM (January 2012). "Melodic Intonation Therapy: present controversies and future opportunities". Archives of Physical Medicine and Rehabilitation. 93 (1 Suppl): S46-52. doi:10.1016/j.apmr.2011.05.029. PMID 22202191.
- Stahl B, Kotz SA (2013). "Facing the music: three issues in current research on singing and aphasia". Frontiers in Psychology. 5 (1033): 1033. doi:10.3389/fpsyg.2014.01033. PMC 4172097. PMID 25295017.
- Simmons-Mackie, Nina; Raymer, Anastasia; Cherney, Leora R. (2016). "Communication Partner Training in Aphasia: An Updated Systematic Review". Archives of Physical Medicine and Rehabilitation. 97 (12): 2202–2221.e8. doi:10.1016/j.apmr.2016.03.023. PMID 27117383.
- "Aphasia". National Institute on Deafness and Other Communication Disorders. 2015-08-18. Retrieved December 16, 2017.
- Russo MJ (2017). "High-technology Augmentative Communication for adults with post-stroke aphasia: a systematic review". Expert Review of Medical Devices. April 26 (5): 355–370. doi:10.1080/17434440.2017.1324291. PMID 28446056. S2CID 10452302.
- Brady MC, Kelly H, Godwin J, Enderby P, Campbell P (June 2016). "Speech and language therapy for aphasia following stroke". The Cochrane Database of Systematic Reviews. 2016 (6): CD000425. doi:10.1002/14651858.CD000425.pub4. hdl:1893/26112. PMID 27245310.
- Cherney LR, Patterson JP, Raymer AM (December 2011). "Intensity of aphasia therapy: evidence and efficacy". Current Neurology and Neuroscience Reports. 11 (6): 560–9. doi:10.1007/s11910-011-0227-6. PMID 21960063. S2CID 10559070.
- Sage K, Snell C, Lambon Ralph MA (January 2011). "How intensive does anomia therapy for people with aphasia need to be?". Neuropsychological Rehabilitation. 21 (1): 26–41. doi:10.1080/09602011.2010.528966. PMID 21181603. S2CID 27001159.
- Palmer R (2015). "Innovations in aphasia treatment after stroke: Technology to the rescue". British Journal of Neuroscience Nursing. 38: 38–42. doi:10.12968/bjnn.2015.11.sup2.38.
- "Aphasia FAQs". National Aphasia Association. Retrieved December 16, 2017.
- Watila MM, Balarabe SA (May 2015). "Factors predicting post-stroke aphasia recovery". Journal of the Neurological Sciences. 352 (1–2): 12–8. doi:10.1016/j.jns.2015.03.020. PMID 25888529.
- Laska AC, Hellblom A, Murray V, Kahan T, Von Arbin M (May 2001). "Aphasia in acute stroke and relation to outcome". Journal of Internal Medicine. 249 (5): 413–22. doi:10.1046/j.1365-2796.2001.00812.x. PMID 11350565. S2CID 32102500.
- McCrory PR, Berkovic SF (December 2001). "Concussion: the history of clinical and pathophysiological concepts and misconceptions". Neurology. 57 (12): 2283–9. doi:10.1212/WNL.57.12.2283. PMID 11756611.
- Eling P, Whitaker H (2009). "Chapter 36 History of aphasia". History of Neurology. Handbook of Clinical Neurology. 95. pp. 571–82. doi:10.1016/S0072-9752(08)02136-2. ISBN 978-0-444-52009-8. PMID 19892139.
- Boller F (May 1977). "Johann Baptist Schmidt. A pioneer in the history of aphasia". Archives of Neurology. 34 (5): 306–7. doi:10.1001/archneur.1977.00500170060011. PMID 324450.
- Riese W (1947-05-01). "The early history of aphasia". Bulletin of the History of Medicine. 21 (3): 322–34. PMID 20257374.
- ἀφασία, Henry George Liddell, Robert Scott, A Greek-English Lexicon, on Perseus.
- ἄφατος, Henry George Liddell, Robert Scott, A Greek-English Lexicon, on Perseus.
External links
| Classification | |
|---|---|
| External resources |
| Library resources about Aphasia |
| Look up aphasia or aphemia in Wiktionary, the free dictionary. |
