CA19-9
Carbohydrate antigen 19-9 (CA19-9), also known as sialyl-LewisA, is a tetrasaccharide which is usually attached to O-glycans on the surface of cells. It is known to play a vital role in cell-to-cell recognition processes. It is also a tumor marker used primarily in the management of pancreatic cancer.[1]
 | |
| Names | |
|---|---|
| Other names
sialyl LeA, SLeA, cancer antigen 19-9, CA19-9 | |
| Identifiers | |
3D model (JSmol) |
|
| ChEBI | |
| ChemSpider | |
| MeSH | sialyl+Lewis+A |
PubChem CID |
|
| UNII | |
| |
| Properties | |
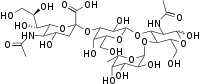
| C31H52N2O23 | |
| Molar mass | 820.748 g·mol−1 |
Except where otherwise noted, data are given for materials in their standard state (at 25 °C [77 °F], 100 kPa). | |
| Infobox references | |
Structure
CA19-9 is the sialylated form of Lewis AntigenA. It is a tetrasaccharide with the sequence Neu5Acα2-3Galβ1-3[Fucα1-4]GlcNAcβ.
Clinical significance
Tumor marker
Guidelines from the American Society of Clinical Oncology discourage the use of CA19-9 as a screening test for cancer, particularly pancreatic cancer. The reason is that the test may be falsely normal (false negative) in many cases, or abnormally elevated in people who have no cancer at all (false positive). The main use of CA19-9 is therefore to see whether a pancreatic tumor is secreting it; if that is the case, then the levels should fall when the tumor is treated, and they may rise again if the disease recurs.[2] Therefore it is useful as a surrogate marker for relapse.
In people with pancreatic masses, CA19-9 can be useful in distinguishing between cancer and other diseases of the gland.[1][3]
Limitations
CA19-9 can be elevated in many types of gastrointestinal cancer, such as colorectal cancer, esophageal cancer and hepatocellular carcinoma.[1] Apart from cancer, elevated levels may occur in pancreatitis, cirrhosis,[1] and diseases of the bile ducts.[1][3] It can also be elevated in people with obstruction of the bile ducts.[3]
In patients who lack the Lewis antigen A (a blood type antigen on red blood cells), which is about 10% of the Caucasian population, CA19-9 is not produced by any cells,[3] even in those with large tumors.[2] This is because of a deficiency of a fucosyltransferase enzyme that is needed to produce Lewis antigen A.[2]
History
CA19-9 was discovered in the serum of patients with colon cancer and pancreatic cancer in 1981.[4] It was characterized shortly after, and it was found to be carried primarily by mucins.[5]
See also
References
- Perkins, G.; Slater, E.; Sanders, G.; Prichard, J. (2003). "Serum tumor markers". American Family Physician. 68 (6): 1075–1082. PMID 14524394.
- Locker G, Hamilton S, Harris J, Jessup J, Kemeny N, Macdonald J, Somerfield M, Hayes D, Bast R (2006). "ASCO 2006 update of recommendations for the use of tumor markers in gastrointestinal cancer". J. Clin. Oncol. 24 (33): 5313–27. doi:10.1200/JCO.2006.08.2644. PMID 17060676.
- Goonetilleke KS, Siriwardena AK (April 2007). "Systematic review of carbohydrate antigen (CA19-9) as a biochemical marker in the diagnosis of pancreatic cancer". Eur J Surg Oncol. 33 (3): 266–70. doi:10.1016/j.ejso.2006.10.004. PMID 17097848.
- Koprowski H, Herlyn M, Steplewski Z, Sears HF (1981). "Specific antigen in serum of patients with colon carcinoma". Science. 212 (4490): 53–5. Bibcode:1981Sci...212...53K. doi:10.1126/science.6163212. PMID 6163212.
- Magnani, JL (15 June 2004). "The discovery, biology, and drug development of sialyl Lea and sialyl Lex". Archives of Biochemistry and Biophysics. 426 (2): 122–31. doi:10.1016/j.abb.2004.04.008. PMID 15158662.
External links
- CA-19-9+Antigen at the US National Library of Medicine Medical Subject Headings (MeSH)
- CA19-9 at Lab Tests Online
- CA19-9: analyte monograph - The Association for Clinical Biochemistry and Laboratory Medicine
- Essentials of Glycobiology 3rd Edition, Chapter 14: "Structures Common to Different Glycans" https://www.ncbi.nlm.nih.gov/books/NBK453042/#_Ch14_s2_
