Tenecteplase
Tenecteplase (sold under the trade names TNKase and Metalyse) is an enzyme used as a thrombolytic drug.
| Clinical data | |
|---|---|
| Trade names | TNKase |
| AHFS/Drugs.com | Monograph |
| License data | |
| ATC code | |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Excretion | Liver |
| Identifiers | |
| |
| CAS Number | |
| DrugBank | |
| ChemSpider |
|
| UNII | |
| KEGG | |
| Chemical and physical data | |
| Formula | C2561H3919N747O781S40 |
| Molar mass | 58951.37 g·mol−1 |
| | |
Tenecteplase is a tissue plasminogen activator (tPA) produced by recombinant DNA technology using an established mammalian cell line (Chinese hamster ovary cells). Tenecteplase is a 527 amino acid glycoprotein developed by introducing the following modifications to the complementary DNA (cDNA) for natural human tPA: a substitution of threonine 103 with asparagine, and a substitution of asparagine 117 with glutamine, both within the kringle 1 domain, and a tetra-alanine substitution at amino acids 296–299 in the protease domain.
Tenecteplase is a recombinant fibrin-specific plasminogen activator that is derived from native t-PA by modifications at three sites of the protein structure. It binds to the fibrin component of the thrombus (blood clot) and selectively converts thrombus-bound plasminogen to plasmin, which degrades the fibrin matrix of the thrombus. Tenecteplase has a higher fibrin specificity and greater resistance to inactivation by its endogenous inhibitor (PAI-1) compared to native t-PA.
The abbreviation TNK is common for referring to tenecteplase, but abbreviating drug names is not best practice in medicine, and in fact "TNK" is one of the examples given on the Institute for Safe Medication Practices (ISMP) do-not-use list.
Research
Researchers at Newcastle University in Australia say they have had a significant breakthrough in treating stroke patients using the commonly used drug.[1] The findings were published in the New England Medical Journal. There is ongoing controversy about whether this is a harmful treatment, and significant ongoing discussion between Emergency Physicians and Neurologists about whether this treatment should be used at all.
Pharmacokinetics
Distribution: approximates plasma volume
Metabolism: Primarily hepatic
Half-life elimination: Biphasic: Initial: 20–24 minutes; Terminal: 90–130 minutes
Excretion: Clearance: Plasma: 99-119 mL/minute
Gallery
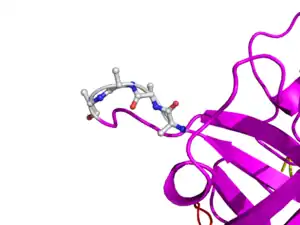
 Here is TNK-tPA. It is very similar to t-PA, but the glycosylation occurring in Kringle 1 is manipulated. The mutation T103N means that glycosylation occurs at that point. The mutation N117E means that the high mannose sugar residue is absent at that point
Here is TNK-tPA. It is very similar to t-PA, but the glycosylation occurring in Kringle 1 is manipulated. The mutation T103N means that glycosylation occurs at that point. The mutation N117E means that the high mannose sugar residue is absent at that point
References
- Parsons M, Spratt N, Bivard A, Campbell B, Chung K, Miteff F, O'Brien B, Bladin C, McElduff P, Allen C, Bateman G, Donnan G, Davis S, Levi C (Mar 2012). "A randomized trial of tenecteplase versus alteplase for acute ischemic stroke". The New England Journal of Medicine. 366 (12): 1099–107. doi:10.1056/NEJMoa1109842. hdl:1959.13/1039697. PMID 22435369.
Further reading
- Gurbel PA, Hayes K, Bliden KP, Yoho J, Tantry US (Jan 2005). "The platelet-related effects of tenecteplase versus alteplase versus reteplase". Blood Coagulation & Fibrinolysis. 16 (1): 1–7. doi:10.1097/00001721-200501000-00001. PMID 15650539. S2CID 44664652.
- Melzer C, Richter C, Rogalla P, Borges AC, Theres H, Baumann G, Laule M (Aug 2004). "Tenecteplase for the treatment of massive and submassive pulmonary embolism". Journal of Thrombosis and Thrombolysis. 18 (1): 47–50. doi:10.1007/s11239-004-0174-z. PMID 15744554. S2CID 10947258.
- Ohman EM, Van de Werf F, Antman EM, Califf RM, de Lemos JA, Gibson CM, Oliverio RL, Harrelson L, McCabe C, DiBattiste P, Braunwald E (Jul 2005). "Tenecteplase and tirofiban in ST-segment elevation acute myocardial infarction: results of a randomized trial". American Heart Journal. 150 (1): 79–88. doi:10.1016/j.ahj.2005.01.007. PMID 16084152.
- De Luca G, Suryapranata H, Chiariello M (Dec 2005). "Tenecteplase followed by immediate angioplasty is more effective than tenecteplase alone for people with STEMI. Commentary". Evidence-Based Cardiovascular Medicine. 9 (4): 284–7. doi:10.1016/j.ebcm.2005.09.021. PMID 16380055.
- Assessment of the Safety Efficacy of a New Treatment Strategy with Percutaneous Coronary Intervention (ASSENT-4 PCI) investigators. (Feb 2006). "Primary versus tenecteplase-facilitated percutaneous coronary intervention in patients with ST-segment elevation acute myocardial infarction (ASSENT-4 PCI): randomised trial". Lancet. 367 (9510): 569–78. doi:10.1016/S0140-6736(06)68147-6. PMID 16488800. S2CID 23972378.
- Bozeman WP, Kleiner DM, Ferguson KL (Jun 2006). "Empiric tenecteplase is associated with increased return of spontaneous circulation and short term survival in cardiac arrest patients unresponsive to standard interventions". Resuscitation. 69 (3): 399–406. doi:10.1016/j.resuscitation.2005.09.027. PMID 16563599.
- Hull JE, Hull MK, Urso JA, Park HA (Apr 2006). "Tenecteplase in acute lower-leg ischemia: efficacy, dose, and adverse events". Journal of Vascular and Interventional Radiology. 17 (4): 629–36. doi:10.1097/01.RVI.0000202751.74625.79. PMID 16614145.
- http://www.abc.net.au/news/2012-03-22/stroke-study-makes-treatment-breakthrough/3905512
- Parsons M, Spratt N, Bivard A, Campbell B, Chung K, Miteff F, O'Brien B, Bladin C, McElduff P, Allen C, Bateman G, Donnan G, Davis S, Levi C (Mar 2012). "A randomized trial of tenecteplase versus alteplase for acute ischemic stroke". The New England Journal of Medicine. 366 (12): 1099–107. doi:10.1056/NEJMoa1109842. hdl:1959.13/1039697. PMID 22435369.
