Health effects of wine
The health effects of wine are mainly determined by its active ingredient alcohol.[1][2] Some studies found that, when comparing people who consume alcohol, drinking small quantities of alcohol (up to one standard drink per day for women and one to two drinks per day for men) is associated with a decreased risk of heart disease, stroke, diabetes mellitus, metabolic syndrome and early death.[2][3] However, other studies found no such effect.[4]


Drinking more than the standard drink amount increases the risk of heart disease, high blood pressure, atrial fibrillation, stroke[3] and cancer.[5] Mixed results are also observed in light drinking and cancer mortality.[5][6][7][8]
Risk is greater in young people due to binge drinking which may result in violence or accidents.[3] About 88,000 deaths in the US are estimated to be due to alcohol each year.[9] Alcoholism reduces a person's life expectancy by around ten years[10] and excessive alcohol use is the third leading cause of early death in the United States.[3] According to systematic reviews and medical associations, people who are nondrinkers should not start drinking wine.[3][7][11]
Wine has a long history of use as an early form of medication, being recommended variously as a safe alternative to drinking water, an antiseptic for treating wounds, a digestive aid, and as a cure for a wide range of ailments including lethargy, diarrhea and pain from child birth.[12] Ancient Egyptian papyri and Sumerian tablets dating back to 2200 BC detail the medicinal role of wine, making it the world's oldest documented human-made medicine.[13]:433 Wine continued to play a major role in medicine until the late 19th and early 20th century, when changing opinions and medical research on alcohol and alcoholism cast doubt on its role as part of a healthy lifestyle.
Moderate consumption

Nearly all research into the positive medical benefits of wine consumption makes a distinction between moderate consumption and heavy or binge drinking.[3] Moderate levels of consumption vary by the individual according to age, sex, genetics, weight and body stature, as well as situational conditions, such as food consumption or use of drugs.[3] In general, women absorb alcohol more quickly than men due to their lower body water content, so their moderate levels of consumption may be lower than those for a male of equal age.[13]:341–2 Some experts define "moderate consumption" as less than one 5-US-fluid-ounce (150 ml) glass of wine per day for women and two glasses per day for men.[3][14]
The view of consuming wine in moderation has a history recorded as early as the Greek poet Eubulus (360 BC) who believed that three bowls (kylix) were the ideal amount of wine to consume. The number of three bowls for moderation is a common theme throughout Greek writing; today the standard 750 ml wine bottle contains roughly the volume of three kylix cups (250 ml or 8 fl oz each).[15] However, the kylix cups would have contained a diluted wine, at a 1:2 or 1:3 dilution with water. In his circa 375 BC play Semele or Dionysus, Eubulus has Dionysus say:
Three bowls do I mix for the temperate: one to health, which they empty first, the second to love and pleasure, the third to sleep. When this bowl is drunk up, wise guests go home. The fourth bowl is ours no longer, but belongs to violence; the fifth to uproar, the sixth to drunken revel, the seventh to black eyes, the eighth is the policeman's, the ninth belongs to biliousness, and the tenth to madness and hurling the furniture.[16]
Effect on the body
Bones
Heavy alcohol consumption has been shown to have a damaging effect on the cellular processes that create bone tissue, and long-term alcoholic consumption at high levels increases the frequency of fractures.[17] Epidemiological studies (studies done by interviewing subjects and studying their health records) have found a positive association between moderate alcohol consumption and increased bone mineral density (BMD). Most of this research has been conducted with postmenopausal women, but one study in men concluded that moderate consumption of alcohol may also be beneficial to BMD in men.[18]
Cancer
The International Agency for Research on Cancer of the World Health Organization has classified alcohol as a Group 1 carcinogen.[19]
A 2019 study found that drinking one bottle of wine per week is associated with an increased lifetime cancer risk for non-smokers of 1% for men and 1.4% for women, while consuming three bottles of wine per week approximately doubled the cancer risk for men and women.[20] The study equated the cancer risk of consuming one bottle of wine per week to smoking five cigarettes per week for men or 10 for women.[20]
Cardiovascular system
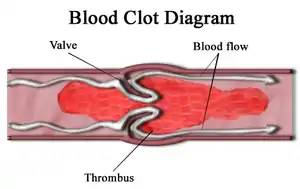
Studies have shown that heavy drinkers put themselves at greater risk for heart disease and developing potentially fatal cardiac arrhythmias. Excessive alcohol consumption can cause higher blood pressure, increased cholesterol levels and weakened heart muscles. Studies have shown that moderate wine drinking can improve the balance of low-density lipoprotein (LDL or "bad" cholesterol) to high-density lipoprotein (HDL or "good" cholesterol), which has been theorized as to clean up or remove LDL from blocking arteries.[21] The main cause of heart attacks and the pain of angina is the lack of oxygen caused by blood clots and atheromatous plaque build up in the arteries. The alcohol in wine has anticoagulant properties that limit blood clotting by making the platelets in the blood less prone to stick together and reducing the levels of fibrin protein that binds them together.[22]
Professional cardiology associations recommend that people who are currently nondrinkers should not start drinking alcohol.[11]
Diabetes
Research has shown that moderate levels of alcohol consumed with meals does not have a substantial impact on blood sugar levels. A 2005 study presented to the American Diabetes Association suggest that moderate consumption may lower the risk of developing Type 2 diabetes.[13]:341–2[23]
Digestive system

The risk of infection from the bacterium Helicobacter pylori, which is associated with gastritis and peptic ulcers, appears to be lower with moderate alcohol consumption.[24][25]
Headaches
There are several potential causes of so-called "red wine headaches", including histamine and tannins from grape skin or other phenolic compounds in wine.[26] Sulfites – which are used as a preservative in wine – are unlikely to be a headache factor.[26] Wine, like other alcoholic beverages, is a diuretic which promotes dehydration that can lead to headaches (such as the case often experienced with hangovers),[12] indicating a need to maintain hydration when drinking wine and to consume in moderation.[26] A 2017 review found that 22% of people experiencing migraine or tension headaches identified alcohol as a precipitating factor, and red wine as three times more likely to trigger a headache than beer.[27]
Food intake

Alcohol can stimulate the appetite so it is better to drink it with food. When alcohol is mixed with food, it can slow the stomach's emptying time and potentially decrease the amount of food consumed at the meal.[21]
A 150-millilitre (5-US-fluid-ounce) serving of red or white wine provides about 500 to 540 kilojoules (120 to 130 kilocalories) of food energy, while dessert wines provide more.[28] Most wines have an alcohol by volume (ABV) percentage of about 11%; the higher the ABV, the higher the energy content of a wine.[28]
Psychological and social
Danish epidemiological studies suggest that a number of psychological health benefits are associated with drinking wine. In a study testing this idea, Mortensen et al. (2001) measured socioeconomic status, education, IQ, personality, psychiatric symptoms, and health related behaviors, which included alcohol consumption. The analysis was then broken down into groups of those who drank beer, those who drank wine, and then those who did and did not drink at all. The results showed that for both men and women drinking wine was related to higher parental social status, parental education and the social status of the subjects. When the subjects were given an IQ test, wine drinkers consistently scored higher IQs than their counterpart beer drinkers. The average difference of IQ between wine and beer drinkers was 18 points. In regards to psychological functioning, personality, and other health-related behaviors, the study found wine drinkers to operate at optimal levels while beer drinkers performed below optimal levels. As these social and psychological factors also correlate with health outcomes, they represent a plausible explanation for at least some of the apparent health benefits of wine.
However, more research should be conducted as to the relationship between wine consumption and IQ along with the apparent correlations between beer drinkers and wine drinkers and how they are different psychologically. The study conducted by Mortensen should not be read as gospel. Wine and Beer being an indicator of a persons IQ level should be viewed with a very cautious lens. This study, from what we know, does not take into account the genetic, prenatal and environmental influences of how a persons generalized intelligence is formed. In current scientific literature, it is still a matter of debate and discovery as to what are true and reliable indicators of intelligence. Regular wine consumption being an indicator of higher intelligence while beer being an indicator of low intelligence according to Mortensen et al. (2009) should be looked at with a very critical lens. There should be future research into the validity of whether or not individuals who regularly consume wine have higher IQ scores in comparison to those who drink beer. [29]
Heavy metals
In 2008, researchers from Kingston University in London discovered red wine[30] to contain high levels of toxic metals relative to other beverages in the sample. Although the metal ions, which included chromium, copper, iron, manganese, nickel, vanadium and zinc, were also present in other plant-based beverages, the sample wine tested significantly higher for all metal ions, especially vanadium.[31] Risk assessment was calculated using "target hazard quotients" (THQ), a method of quantifying health concerns associated with lifetime exposure to chemical pollutants. Developed by the Environmental Protection Agency in the US and used mainly to examine seafood, a THQ of less than 1 represents no concern while, for example, mercury levels in fish calculated to have THQs of between 1 and 5 would represent cause for concern.[32]
The researchers stressed that a single glass of wine would not lead to metal poisoning, pointing out that their THQ calculations were based on the average person drinking one-third of a bottle of wine (250 ml) every day between the ages of 18 and 80. However the "combined THQ values" for metal ions in the red wine they analyzed were reported to be as high as 125.[31] A subsequent study by the same university using a meta analysis of data based on wine samples from a selection of mostly European countries found equally high levels of vanadium in many red wines, showing combined THQ values in the range of 50 to 200, with some as high as 350.[33]
The findings sparked immediate controversy due to several issues: the study's reliance on secondary data; the assumption that all wines contributing to that data were representative of the countries stated; and the grouping together of poorly understood high-concentration ions, such as vanadium, with relatively low-level, common ions such as copper and manganese. Some publications pointed out that the lack of identifiable wines and grape varieties, specific producers or even wine regions, provided only misleading generalizations that should not be relied upon in choosing wines.[34][35]
In a news bulletin following the widespread reporting of the findings, the UK's National Health Service (NHS) were also concerned that "the way the researchers added together hazards from different metals to produce a final score for individual wines may not be particularly meaningful".[35] Commentators in the US questioned the relevance of seafood-based THQ assessments to agricultural produce, with the TTB, responsible for testing imports for metal ion contamination, have not detected an increased risk. George Solas, quality assessor for the Canadian Liquor Control Board of Ontario (LCBO) claimed that the levels of heavy metal contamination reported were within the permitted levels for drinking water in tested reservoirs.[34]
Whereas the NHS also described calls for improved wine labeling as an "extreme response" to research which provided "few solid answers", they acknowledged the authors call for further research to investigate wine production, including the influence that grape variety, soil type, geographical region, insecticides, containment vessels and seasonal variations may have on metal ion uptake.[35]
Chemical composition
Natural phenols and polyphenols
Although red wine contains many chemicals under basic research for their potential health benefits, resveratrol has been particularly well studied and evaluated by regulatory authorities, such as the European Food Safety Authority and US Food and Drug Administration which identified it and other such phenolic compounds as not sufficiently understood to confirm their role as physiological antioxidants.[36][37]
Cinnamates have been shown to have more antioxidant activity when exposed in vitro to the Fenton reaction (catalytic Fe(II) with hydrogen peroxide) than the other natural phenols present in wine.[38]
Resveratrol
Research on potential health effects of resveratrol is in its infancy and the long-term effects of supplementation in humans are not known.[36][39][40]
Resveratrol is a stilbenoid phenolic compound found in wine produced in the grape skins and leaves of grape vines. It has received considerable attention in both the media and medical research community for its potential health benefits[13]:569 which remain unproven in humans.[41][37]
The production and concentration of resveratrol is not equal among all the varieties of wine grapes. Differences in clones, rootstock, Vitis species as well as climate conditions can affect the production of resveratrol. Also, because resveratrol is part of the defence mechanism in grapevines against attack by fungi or grape disease, the degree of exposure to fungal infection and grape diseases also appear to play a role. The Muscadinia family of vines, which has adapted over time through exposure to North American grape diseases such as phylloxera, has some of the highest concentrations of resveratrol among wine grapes. Among the European Vitis vinifera, grapes derived from the Burgundian Pinot family tend to have substantially higher amounts of resveratrol than grapes derived from the Cabernet family of Bordeaux. Wine regions with cooler, wetter climates that are more prone to grape disease and fungal attacks such as Oregon and New York tend to produce grapes with higher concentrations of resveratrol than warmer, dry climates like California and Australia.[13]:569
Although red wine and white vine varieties produce similar amounts of resveratrol, red wine contains more than white, since red wines are produced by maceration (soaking the grape skins in the mash). Other winemaking techniques, such as the use of certain strains of yeast during fermentation or lactic acid bacteria during malolactic fermentation, can have an influence on the amount of resveratrol left in the resulting wines. Similarly, the use of certain fining agents during the clarification and stabilization of wine can strip the wine of some resveratrol molecules.[13]:569
The prominence of resveratrol in the news and its association with positive health benefits has encouraged some wineries to highlight it in their marketing. In the early 21st century, the Oregon producer Willamette Valley Vineyards sought approval from the Alcohol and Tobacco Tax and Trade Bureau (TTB) to state on their wine labels the resveratrol levels of their wines which ranged from 19 to 71 micromoles per liter (higher than the average 10 micromoles per liter in most red wines). The TTB gave preliminary approval to the winery, making it the first to use such information on its labels.[12] While resveratrol is the most widely publicized, there are other phenolic components in wine that have been the focus of medical research for potential health benefits, including the compounds catechin and quercetin,[13]:569 none of which has been proven to have any health value in humans.[36][37]
Anthocyanins
Red grapes are high in anthocyanins which are the source of the color of various fruits, such as red grapes. The darker the red wine, the more anthocyanins present.[42]
Following dietary ingestion, anthocyanins undergo rapid and extensive metabolism that makes the biological effects presumed from in vitro studies unlikely to apply in vivo.[37][43]
Although anthocyanins are under basic and early-stage clinical research for a variety of disease conditions, there exists no sufficient evidence that they have any beneficial effect in the human body.[37] The US FDA has issued warning letters, e.g.,[44] to emphasize that anthocyanins are not a defined nutrient, cannot be assigned a dietary content level and are not regulated as a drug to treat any human disease.[37]
History of wine in medicine
Early medicine was intimately tied with religion and the supernatural, with early practitioners often being priests and magicians. Wine's close association with ritual made it a logical tool for these early medical practices. Tablets from Sumeria and papyri from Egypt dating to 2200 BC include recipes for wine based medicines, making wine the oldest documented human-made medicine.[13]:433
Early history
When the Greeks introduced a more systematized approach to medicine, wine retained its prominent role. The Greek physician Hippocrates considered wine a part of a healthy diet, and advocated its use as a disinfectant for wounds, as well as a medium in which to mix other drugs for consumption by the patient. He also prescribed wine as a cure for various ailments ranging from diarrhea and lethargy to pain during childbirth.[13]:433
The medical practices of the Romans involved the use of wine in a similar manner. In his 1st-century work De Medicina, the Roman encyclopedist Aulus Cornelius Celsus detailed a long list of Greek and Roman wines used for medicinal purposes. While treating gladiators in Asia Minor, the Roman physician Galen would use wine as a disinfectant for all types of wounds, and even soaked exposed bowels before returning them to the body. During his four years with the gladiators, only five deaths occurred, compared to sixty deaths under the watch of the physician before him.[45]
Religion still played a significant role in promoting wine's use for health. The Jewish Talmud noted wine to be "the foremost of all medicines: wherever wine is lacking, medicines become necessary." In his first epistle to Timothy, Paul the Apostle recommended that his young colleague drink a little wine every now and then for the benefit of his stomach and digestion. While the Islamic Koran contained restrictions on all alcohol, Islamic doctors such as the Persian Avicenna in the 11th century AD noted that wine was an efficient digestive aid but, because of the laws, were limited to use as a disinfectant while dressing wounds. Catholic monasteries during the Middle Ages also regularly used wine for medical treatments.[13]:433 So closely tied was the role of wine and medicine, that the first printed book on wine was written in the 14th century by a physician, Arnaldus de Villa Nova, with lengthy essays on wine's suitability for treatment of a variety of medical ailments such dementia and sinus problems.[46]
Risks of consumption
The lack of safe drinking water may have been one reason for wine's popularity in medicine. Wine was still being used to sterilize water as late as the Hamburg cholera epidemic of 1892 in order to control the spread of the disease. However, the late 19th century and early 20th century ushered in a period of changing views on the role of alcohol and, by extension, wine in health and society. The Temperance movement began to gain steam by touting the ills of alcoholism, which was eventually defined by the medical establishment as a disease. Studies of the long- and Short-term effects of alcohol consumption caused many in the medical community to reconsider the role of wine in medicine and diet.[13]:433 Soon, public opinion turned against consumption of alcohol in any form, leading to Prohibition in the United States and other countries. In some areas, wine was able to maintain a limited role, such as an exemption from Prohibition in the United States for "therapeutic wines" that were sold legally in drug stores. These wines were marketed for their supposed medicinal benefits, but some wineries used this measure as a loophole to sell large quantities of wine for recreational consumption. In response, the United States government issued a mandate requiring producers to include an emetic additive that would induce vomiting above the consumption of a certain dosage level.[12]
Throughout the mid to early 20th century, health advocates pointed to the risk of alcohol consumption and the role it played in a variety of ailments such as blood disorders, high blood pressure, cancer, infertility, liver damage, muscle atrophy, psoriasis, skin infections, strokes, and long-term brain damage. Studies showed a connection between alcohol consumption among pregnant mothers and an increased risk of mental retardation and physical abnormalities in what became known as fetal alcohol syndrome, prompting the use of alcohol packaging warning messages in several countries.[13]:341–2
French paradox and the benefits of consumption

The 1990s and early 21st century saw a renewed interest in the health benefits of wine, ushered in by increasing research suggesting that moderate wine drinkers have lower mortality rates than heavy drinkers or teetotalers.[13]:341–2 In November 1991, the U.S. news program 60 Minutes aired a broadcast on the so-called "French Paradox". Featuring the research work of Bordeaux scientist Serge Renaud, the broadcast dealt with the seemingly paradoxical relationship between the high fat/high dairy diets of French people and the low occurrence of cardiovascular disease among them. The broadcast drew parallels to the American and British diets which also contained high levels of fat and dairy but which featured high incidences of heart disease. One of the theories proposed by Renaud in the broadcast was that moderate consumption of red wine was a risk-reducing factor for the French and that wine could have more positive health benefits yet to be studied.[47] Following the 60 Minutes broadcast, sales of red wine in the United States jumped 44% over previous years.[48]
This changing view of wine can be seen in the evolution of the language used in the U.S. Food and Drug Administration Dietary Guidelines. The 1990 edition of the guidelines contained the blanket statement that "wine has no net health benefit". By 1995, the wording had been changed to allow moderate consumption with meals providing the individual had no other alcohol-related health risk. From a research perspective, scientists began differentiating alcohol consumption among the various classes of beverages – wine, beer, and spirits. This distinction allowed studies to highlight potentially positive medical benefits of wine apart from the mere presence of alcohol, though these studies are increasingly being called into question.[49] Wine drinkers tend to share similar lifestyle habits – better diets, regular exercise, non-smoking – that may in themselves be a factor in the supposed positive health benefits compared to drinkers of beer and spirits or those who abstain completely.[50]
References
- Trichopoulou A, Lagiou P (November 1997). "Healthy traditional Mediterranean diet: an expression of culture, history, and lifestyle". Nutrition Reviews. 55 (11 Pt 1): 383–9. doi:10.1111/j.1753-4887.1997.tb01578.x. PMID 9420448.
- Shen J, Wilmot KA, Ghasemzadeh N, Molloy DL, Burkman G, Mekonnen G, Gongora MC, Quyyumi AA, Sperling LS (2015). "Mediterranean Dietary Patterns and Cardiovascular Health". Annual Review of Nutrition. 35: 425–49. doi:10.1146/annurev-nutr-011215-025104. PMID 25974696.
- O'Keefe JH, Bhatti SK, Bajwa A, DiNicolantonio JJ, Lavie CJ (March 2014). "Alcohol and cardiovascular health: the dose makes the poison…or the remedy". Mayo Clinic Proceedings. 89 (3): 382–93. doi:10.1016/j.mayocp.2013.11.005. PMID 24582196.
- Stockwell T, Zhao J, Panwar S, Roemer A, Naimi T, Chikritzhs T (March 2016). "Do "Moderate" Drinkers Have Reduced Mortality Risk? A Systematic Review and Meta-Analysis of Alcohol Consumption and All-Cause Mortality". Journal of Studies on Alcohol and Drugs. 77 (2): 185–98. doi:10.15288/jsad.2016.77.185. PMC 4803651. PMID 26997174.
- Jin M, Cai S, Guo J, Zhu Y, Li M, Yu Y, Zhang S, Chen K (March 2013). "Alcohol drinking and all cancer mortality: a meta-analysis". Annals of Oncology. 24 (3): 807–16. doi:10.1093/annonc/mds508. PMID 23104725.
- Bagnardi V, Rota M, Botteri E, Tramacere I, Islami F, Fedirko V, Scotti L, Jenab M, Turati F, Pasquali E, Pelucchi C, Bellocco R, Negri E, Corrao G, Rehm J, Boffetta P, La Vecchia C (February 2013). "Light alcohol drinking and cancer: a meta-analysis". Annals of Oncology. 24 (2): 301–8. doi:10.1093/annonc/mds337. PMID 22910838.
- Poli A, Marangoni F, Avogaro A, Barba G, Bellentani S, Bucci M, Cambieri R, Catapano AL, Costanzo S, Cricelli C, de Gaetano G, Di Castelnuovo A, Faggiano P, Fattirolli F, Fontana L, Forlani G, Frattini S, Giacco R, La Vecchia C, Lazzaretto L, Loffredo L, Lucchin L, Marelli G, Marrocco W, Minisola S, Musicco M, Novo S, Nozzoli C, Pelucchi C, Perri L, Pieralli F, Rizzoni D, Sterzi R, Vettor R, Violi F, Visioli F (June 2013). "Moderate alcohol use and health: a consensus document" (PDF). Nutrition, Metabolism, and Cardiovascular Diseases. 23 (6): 487–504. doi:10.1016/j.numecd.2013.02.007. hdl:10447/94503. PMID 23642930.
- Noelle K. LoConte, Abenaa M. Brewster, Judith S. Kaur, Janette K. Merrill, and Anthony J. Alberg (7 November 2017). "Alcohol and Cancer: A Statement of the American Society of Clinical Oncology". Journal of Clinical Oncology. 36 (1).
Clearly, the greatest cancer risks are concentrated in the heavy and moderate drinker categories. Nevertheless, some cancer risk persists even at low levels of consumption. A meta-analysis that focused solely on cancer risks associated with drinking one drink or fewer per day observed that this level of alcohol consumption was still associated with some elevated risk for squamous cell carcinoma of the esophagus (sRR, 1.30; 95% CI, 1.09 to 1.56), oropharyngeal cancer (sRR, 1.17; 95% CI, 1.06 to 1.29), and breast cancer (sRR, 1.05; 95% CI, 1.02 to 1.08), but no discernable associations were seen for cancers of the colorectum, larynx, and liver.
CS1 maint: multiple names: authors list (link) - "Alcohol Facts and Statistics". Retrieved 9 May 2015.
- Schuckit MA (November 2014). "Recognition and management of withdrawal delirium (delirium tremens)". The New England Journal of Medicine. 371 (22): 2109–13. doi:10.1056/NEJMra1407298. PMID 25427113.
- "Alcohol and heart health". American Heart Association. 2016. Retrieved 12 December 2016.
- Harding G (2005). A Wine Miscellany. New York: Clarkson Potter. pp. 66–70, 90 & 108. ISBN 978-0-307-34635-3.
- Robinson J, ed. (2006). The Oxford Companion to Wine (3rd ed.). Oxford University Press. ISBN 978-0-19-860990-2.
- Shuman TC, ed. (October 1, 2005). "Alcohol and Heart disease". WebMD.
- Johnson H (1989). Vintage: The Story of Wine. Simon and Schuster. pp. 35–46. ISBN 978-0-671-68702-1.
- Eubulus. Semele or Dionysus, fr. 93.
- Walker-Bone K (August 2012). "Recognizing and treating secondary osteoporosis". Nature Reviews. Rheumatology. 8 (8): 480–92. doi:10.1038/nrrheum.2012.93. PMID 22782006.
- McLernon DJ, Powell JJ, Jugdaohsingh R, Macdonald HM (May 2012). "Do lifestyle choices explain the effect of alcohol on bone mineral density in women around menopause?". The American Journal of Clinical Nutrition. 95 (5): 1261–9. doi:10.3945/ajcn.111.021600. PMID 22456655.
- Alcohol drinking. Lyon: World Health Organization, International Agency for Research on Cancer. 1988. pp. 2–3. ISBN 978-92-832-1244-7.
- Hydes, Theresa J.; Burton, Robyn; Inskip, Hazel; Bellis, Mark A.; Sheron, Nick (28 March 2019). "A comparison of gender-linked population cancer risks between alcohol and tobacco: how many cigarettes are there in a bottle of wine?". BMC Public Health. 19 (1): 316. doi:10.1186/s12889-019-6576-9. ISSN 1471-2458.
- Zelman, Kathleen M. (January 26, 2005). "Wine: How Much Is Good for You?". WebMD.
- Guilford JM, Pezzuto JM (2011). "Wine and Health: A Review". American Journal of Enology and Viticulture. 62 (4): 471–86. doi:10.5344/ajev.2011.11013.
- Koppes LL, Dekker JM, Hendriks HF, Bouter LM, Heine RJ (March 2005). "Moderate alcohol consumption lowers the risk of type 2 diabetes: a meta-analysis of prospective observational studies". Diabetes Care. 28 (3): 719–25. doi:10.2337/diacare.28.3.719. PMID 15735217.
- Brenner H, Berg G, Lappus N, Kliebsch U, Bode G, Boeing H (May 1999). "Alcohol consumption and Helicobacter pylori infection: results from the German National Health and Nutrition Survey". Epidemiology. 10 (3): 214–8. doi:10.1097/00001648-199905000-00004. JSTOR 3703585. PMID 10230827.
- Liu, Shi-Yu; Han, Xin-Chen; Sun, Jan; Chen, Guang-Xia; Zhou, Xiao-Ying; Zhang, Guo-Xin (2016). "Alcohol intake and Helicobacter pylori infection: a dose–response meta-analysis of observational studies". Infectious Diseases. 48 (4): 303–309. doi:10.3109/23744235.2015.1113556. ISSN 2374-4235. PMID 26585858.
- "Ask the doctor: What causes red wine headaches?". Harvard Health Publishing, Harvard Medical School. 2019. Retrieved 15 May 2019.
- Davis-Martin, Rachel E.; Polk, Ashley N.; Smitherman, Todd A. (26 August 2017). "Alcohol use as a comorbidity and precipitant of primary headache: Review and meta-analysis". Current Pain and Headache Reports. 21 (10). doi:10.1007/s11916-017-0642-8. ISSN 1531-3433. PMID 28844083.
- Locke Hughes (22 March 2017). "How Many Calories Are in Your Wine?". WebMD. Retrieved 15 May 2019.
- Mortensen EL, Jensen HH, Sanders SA, Reinisch JM (2001). "Better psychological functioning and higher social status may largely explain the apparent health benefits of wine: a study of wine and beer drinking in young Danish adults". Archives of Internal Medicine. 161 (15): 1844–8. doi:10.1001/archinte.161.15.1844. PMID 11493125.
- The sample wine was declared to be "a Shiraz from Southeast Australia", although no specific vintage, producer or wine region was stated in the report.
- Hague T, Petroczi A, Andrews PL, Barker J, Naughton DP (June 2008). "Determination of metal ion content of beverages and estimation of target hazard quotients: a comparative study". Chemistry Central Journal. 2: 13. doi:10.1186/1752-153X-2-13. PMC 2443149. PMID 18578877.
- Wang X, Sato T, Xing B, Tao S (November 2005). "Health risks of heavy metals to the general public in Tianjin, China via consumption of vegetables and fish". The Science of the Total Environment. 350 (1–3): 28–37. doi:10.1016/j.scitotenv.2004.09.044. PMID 16227070.
- Naughton DP, Petróczi A (October 2008). "Heavy metal ions in wines: meta-analysis of target hazard quotients reveal health risks". Chemistry Central Journal. 2: 22. doi:10.1186/1752-153X-2-22. PMC 2628338. PMID 18973648.
- Study of Wine's Heavy Metal Hazard Raises Doubts Among Other Experts Wine Spectator, November 2008
- Metal in wine, UK NHS news bulletin, October 2008
- "Scientific Opinion on the substantiation of health claims related to various food(s)/food constituent(s) and protection of cells from premature aging, antioxidant activity, antioxidant content and antioxidant properties, and protection of DNA, proteins and lipids from oxidative damage pursuant to Article 13(1) of Regulation (EC) No 1924/20061". EFSA Journal. 8 (2). 2010. doi:10.2903/j.efsa.2010.1489.
- Gross P (March 1, 2009), New Roles for Polyphenols. A 3-Part report on Current Regulations & the State of Science, Nutraceuticals World
- Gislason NE, Currie BL, Waterhouse AL (June 2011). "Novel antioxidant reactions of cinnamates in wine". Journal of Agricultural and Food Chemistry. 59 (11): 6221–6. doi:10.1021/jf200115y. PMID 21561133.
- The Connecticut Post, "Selling resveratrol: Wonder drug or snake oil?," 08/04/2009, by Melissa Healy for the Los Angeles Times news service
- Gehm BD, McAndrews JM, Chien PY, Jameson JL (December 1997). "Resveratrol, a polyphenolic compound found in grapes and wine, is an agonist for the estrogen receptor". Proceedings of the National Academy of Sciences of the United States of America. 94 (25): 14138–43. doi:10.1073/pnas.94.25.14138. PMC 28446. PMID 9391166.
- EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA) (2010-02-01). "Scientific Opinion on the substantiation of health claims related to various food(s)/food constituent(s) and protection of cells from premature aging, antioxidant activity, antioxidant content and antioxidant properties, and protection of DNA, proteins and lipids from oxidative damage pursuant to Article 13(1) of Regulation (EC) No 1924/2006". EFSA Journal. 8 (2): n/a. doi:10.2903/j.efsa.2010.1489. ISSN 1831-4732.
- Muñoz-Espada AC, Wood KV, Bordelon B, Watkins BA (November 2004). "Anthocyanin quantification and radical scavenging capacity of Concord, Norton, and Marechal Foch grapes and wines". Journal of Agricultural and Food Chemistry. 52 (22): 6779–86. doi:10.1021/jf040087y. PMID 15506816.
- Williams RJ, Spencer JP, Rice-Evans C (April 2004). "Flavonoids: antioxidants or signalling molecules?". Free Radical Biology & Medicine. 36 (7): 838–49. doi:10.1016/j.freeradbiomed.2004.01.001. PMID 15019969.
- "Redco Foods, Inc". Wagner, RF, Inspections, Compliance, Enforcement, and Criminal Investigations, US FDA. 22 February 2010. Retrieved 10 November 2014.
- Nutton V (May 1973). "The chronology of Galen's early career". Classical Quarterly. 23 (1): 158–71. doi:10.1017/S0009838800036600. JSTOR 638137. PMID 11624046.
- Johnson H (1989). Vintage: The Story of Wine. Simon and Schuster. p. 126.
- Mansoon, P. (March 15, 1994). "The Father of the French Paradox". Wine Spectator. Archived from the original on October 12, 2008. Retrieved July 30, 2009.
- Franz M (May 4, 2005). "Merlot's Bad Press". Washington Post.
- Frank M (September 26, 2018). "Bad Wine Health News: You're Going To Die ... Someday". Wine Spectator.
- Mansson P (November 29, 2001). "Eat Well, Drink Wisely, Live Longer". Wine Spectator. Archived from the original on August 4, 2004. Retrieved July 30, 2009.
| Alcohol use |
| ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alcohol control |
| ||||||||||||||||
| Related | |||||||||||||||||
| |||||||||||||||||