Diarrhea
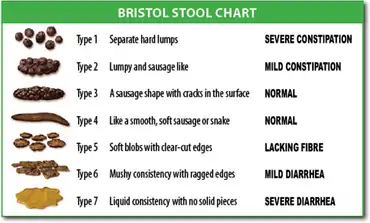
Diarrhea, also spelled diarrhoea, is the condition of having at least three loose, liquid, or watery bowel movements each day.[2] It often lasts for a few days and can result in dehydration due to fluid loss.[2] Signs of dehydration often begin with loss of the normal stretchiness of the skin and irritable behaviour.[2] This can progress to decreased urination, loss of skin color, a fast heart rate, and a decrease in responsiveness as it becomes more severe.[2] Loose but non-watery stools in babies who are exclusively breastfed, however, are normal.[2]
| Diarrhea | |
|---|---|
| Other names | Diarrhoea |
 | |
| An electron micrograph of rotavirus, the cause of nearly 40% of hospitalizations from diarrhea in children under five[1] | |
| Specialty | Infectious disease, gastroenterology |
| Symptoms | Loose frequent bowel movements, dehydration[2] |
| Causes | Usually infection (viral, bacterial, parasitic)[2] |
| Risk factors | Contaminated food or water[2] |
| Prevention | Handwashing, rotavirus vaccination, breastfeeding[2] |
| Treatment | Oral rehydration solution, zinc supplementation[2] |
| Frequency | ≈2.4 billion (2015)[3] |
| Deaths | 1.3 million (2015)[4] |
The most common cause is an infection of the intestines due to either a virus, bacterium, or parasite—a condition also known as gastroenteritis.[2] These infections are often acquired from food or water that has been contaminated by feces, or directly from another person who is infected.[2] The three types of diarrhea are: short duration watery diarrhea, short duration bloody diarrhea, and persistent diarrhea (lasting more than two weeks, which can be either watery or bloody).[2] The short duration watery diarrhea may be due to cholera, although this is rare in the developed world.[2] If blood is present, it is also known as dysentery.[2] A number of non-infectious causes can result in diarrhea.[5] These include lactose intolerance, irritable bowel syndrome, non-celiac gluten sensitivity, celiac disease, inflammatory bowel disease such as ulcerative colitis, hyperthyroidism, bile acid diarrhea, and a number of medications.[5][6][7] In most cases, stool cultures to confirm the exact cause are not required.[8]
Diarrhea can be prevented by improved sanitation, clean drinking water, and hand washing with soap.[2] Breastfeeding for at least six months and vaccination against rotavirus is also recommended.[2] Oral rehydration solution (ORS)—clean water with modest amounts of salts and sugar—is the treatment of choice.[2] Zinc tablets are also recommended.[2] These treatments have been estimated to have saved 50 million children in the past 25 years.[1] When people have diarrhea it is recommended that they continue to eat healthy food and babies continue to be breastfed.[2] If commercial ORS is not available, homemade solutions may be used.[9] In those with severe dehydration, intravenous fluids may be required.[2] Most cases; however, can be managed well with fluids by mouth.[10] Antibiotics, while rarely used, may be recommended in a few cases such as those who have bloody diarrhea and a high fever, those with severe diarrhea following travelling, and those who grow specific bacteria or parasites in their stool.[8] Loperamide may help decrease the number of bowel movements but is not recommended in those with severe disease.[8]
About 1.7 to 5 billion cases of diarrhea occur per year.[2][5][11] It is most common in developing countries, where young children get diarrhea on average three times a year.[2] Total deaths from diarrhea are estimated at 1.26 million in 2013—down from 2.58 million in 1990.[12] In 2012, it was the second most common cause of deaths in children younger than five (0.76 million or 11%).[2][13] Frequent episodes of diarrhea are also a common cause of malnutrition and the most common cause in those younger than five years of age.[2] Other long term problems that can result include stunted growth and poor intellectual development.[13]
Definition
Diarrhea is defined by the World Health Organization as having three or more loose or liquid stools per day, or as having more stools than is normal for that person.[2]
Acute diarrhea is defined as an abnormally frequent discharge of semisolid or fluid fecal matter from the bowel, lasting less than 14 days, by World Gastroenterology Organization.[14]
Secretory
Secretory diarrhea means that there is an increase in the active secretion, or there is an inhibition of absorption. There is little to no structural damage. The most common cause of this type of diarrhea is a cholera toxin that stimulates the secretion of anions, especially chloride ions (Cl–). Therefore, to maintain a charge balance in the gastrointestinal tract, sodium (Na+) is carried with it, along with water. In this type of diarrhea intestinal fluid secretion is isotonic with plasma even during fasting.[15][16] It continues even when there is no oral food intake.
Osmotic
Osmotic diarrhea occurs when too much water is drawn into the bowels. If a person drinks solutions with excessive sugar or excessive salt, these can draw water from the body into the bowel and cause osmotic diarrhea.[17][16] Osmotic diarrhea can also result from maldigestion, e.g. pancreatic disease or coeliac disease in which the nutrients are left in the lumen to pull in water. Or it can be caused by osmotic laxatives (which work to alleviate constipation by drawing water into the bowels). In healthy individuals, too much magnesium or vitamin C or undigested lactose can produce osmotic diarrhea and distention of the bowel. A person who has lactose intolerance can have difficulty absorbing lactose after an extraordinarily high intake of dairy products. In persons who have fructose malabsorption, excess fructose intake can also cause diarrhea. High-fructose foods that also have a high glucose content are more absorbable and less likely to cause diarrhea. Sugar alcohols such as sorbitol (often found in sugar-free foods) are difficult for the body to absorb and, in large amounts, may lead to osmotic diarrhea.[15] In most of these cases, osmotic diarrhea stops when the offending agent, e.g. milk or sorbitol, is stopped.
Exudative
Exudative diarrhea occurs with the presence of blood and pus in the stool. This occurs with inflammatory bowel diseases, such as Crohn's disease or ulcerative colitis, and other severe infections such as E. coli or other forms of food poisoning.[16][15]
Inflammatory
Inflammatory diarrhea occurs when there is damage to the mucosal lining or brush border, which leads to a passive loss of protein-rich fluids and a decreased ability to absorb these lost fluids. Features of all three of the other types of diarrhea can be found in this type of diarrhea.[18] It can be caused by bacterial infections, viral infections, parasitic infections, or autoimmune problems such as inflammatory bowel diseases. It can also be caused by tuberculosis, colon cancer, and enteritis.[16]
Dysentery
If there is blood visible in the stools, it is also known as dysentery. The blood is a trace of an invasion of bowel tissue. Dysentery is a symptom of, among others, Shigella, Entamoeba histolytica, and Salmonella.[16]
Health effects
Diarrheal disease may have a negative impact on both physical fitness and mental development. "Early childhood malnutrition resulting from any cause reduces physical fitness and work productivity in adults,"[19] and diarrhea is a primary cause of childhood malnutrition.[20] Further, evidence suggests that diarrheal disease has significant impacts on mental development and health; it has been shown that, even when controlling for helminth infection and early breastfeeding, children who had experienced severe diarrhea had significantly lower scores on a series of tests of intelligence.[19][21]
Diarrhea can cause electrolyte imbalances, kidney impairment, dehydration, and defective immune system responses. When oral drugs are administered, the efficiency of the drug is to produce a therapeutic effect and the lack of this effect may be due to the medication travelling too quickly through the digestive system, limiting the time that it can be absorbed. Clinicians try to treat the diarrheas by reducing the dosage of medication, changing the dosing schedule, discontinuation of the drug, and rehydration. The interventions to control the diarrhea are not often effective. Diarrhea can have a profound effect on the quality of life because fecal incontinence is one of the leading factors for placing older adults in long term care facilities (nursing homes).[16]
Causes
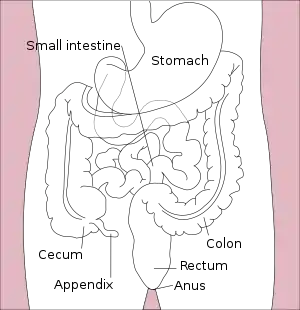
In the latter stages of human digestion, ingested materials are inundated with water and digestive fluids such as gastric acid, bile, and digestive enzymes in order to break them down into their nutrient components, which are then absorbed into the bloodstream via the intestinal tract in the small intestine. Prior to defecation, the large intestine reabsorbs the water and other digestive solvents in the waste product in order to maintain proper hydration and overall equilibrium.[22] Diarrhea occurs when the large intestine is prevented, for any number of reasons, from sufficiently absorbing the water or other digestive fluids from fecal matter, resulting in a liquid, or "loose", bowel movement.
Acute diarrhea is most commonly due to viral gastroenteritis with rotavirus, which accounts for 40% of cases in children under five.[1] In travelers, however, bacterial infections predominate.[23] Various toxins such as mushroom poisoning and drugs can also cause acute diarrhea.
Chronic diarrhea can be the part of the presentations of a number of chronic medical conditions affecting the intestine. Common causes include ulcerative colitis, Crohn disease, microscopic colitis, celiac disease, irritable bowel syndrome, and bile acid malabsorption.
Infections
There are many causes of infectious diarrhea, which include viruses, bacteria and parasites.[24] Infectious diarrhea is frequently referred to as gastroenteritis.[25] Norovirus is the most common cause of viral diarrhea in adults,[26] but rotavirus is the most common cause in children under five years old.[27] Adenovirus types 40 and 41,[28] and astroviruses cause a significant number of infections.[29] Shiga-toxin producing Escherichia coli, such as E coli o157:h7, are the most common cause of infectious bloody diarrhea in the United States.
Campylobacter spp. are a common cause of bacterial diarrhea, but infections by Salmonella spp., Shigella spp. and some strains of Escherichia coli are also a frequent cause.[30]
In the elderly, particularly those who have been treated with antibiotics for unrelated infections, a toxin produced by Clostridioides difficile often causes severe diarrhea.[31]
Parasites, particularly protozoa e.g., Cryptosporidium spp., Giardia spp., Entamoeba histolytica, Blastocystis spp., Cyclospora cayetanensis, are frequently the cause of diarrhea that involves chronic infection. The broad-spectrum antiparasitic agent nitazoxanide has shown efficacy against many diarrhea-causing parasites.[32]
Other infectious agents, such as parasites or bacterial toxins, may exacerbate symptoms.[23] In sanitary living conditions where there is ample food and a supply of clean water, an otherwise healthy person usually recovers from viral infections in a few days. However, for ill or malnourished individuals, diarrhea can lead to severe dehydration and can become life-threatening.[33]
Sanitation

Open defecation is a leading cause of infectious diarrhea leading to death.[34]
Poverty is a good indicator of the rate of infectious diarrhea in a population. This association does not stem from poverty itself, but rather from the conditions under which impoverished people live. The absence of certain resources compromises the ability of the poor to defend themselves against infectious diarrhea. "Poverty is associated with poor housing, crowding, dirt floors, lack of access to clean water or to sanitary disposal of fecal waste (sanitation), cohabitation with domestic animals that may carry human pathogens, and a lack of refrigerated storage for food, all of which increase the frequency of diarrhea ... Poverty also restricts the ability to provide age-appropriate, nutritionally balanced diets or to modify diets when diarrhea develops so as to mitigate and repair nutrient losses. The impact is exacerbated by the lack of adequate, available, and affordable medical care."[35]
One of the most common causes of infectious diarrhea is a lack of clean water. Often, improper fecal disposal leads to contamination of groundwater. This can lead to widespread infection among a population, especially in the absence of water filtration or purification. Human feces contains a variety of potentially harmful human pathogens.[36]
Nutrition
Proper nutrition is important for health and functioning, including the prevention of infectious diarrhea. It is especially important to young children who do not have a fully developed immune system. Zinc deficiency, a condition often found in children in developing countries can, even in mild cases, have a significant impact on the development and proper functioning of the human immune system.[37][38] Indeed, this relationship between zinc deficiency and reduced immune functioning corresponds with an increased severity of infectious diarrhea. Children who have lowered levels of zinc have a greater number of instances of diarrhea, severe diarrhea, and diarrhea associated with fever.[39] Similarly, vitamin A deficiency can cause an increase in the severity of diarrheal episodes. However, there is some discrepancy when it comes to the impact of vitamin A deficiency on the rate of disease. While some argue that a relationship does not exist between the rate of disease and vitamin A status,[40] Others suggest an increase in the rate associated with deficiency.[41] Given that estimates suggest 127 million preschool children worldwide are vitamin A deficient, this population has the potential for increased risk of disease contraction.[42]
Malabsorption
Malabsorption is the inability to absorb food fully, mostly from disorders in the small bowel, but also due to maldigestion from diseases of the pancreas.
Causes include:
- enzyme deficiencies or mucosal abnormality, as in food allergy and food intolerance, e.g. celiac disease (gluten intolerance), lactose intolerance (intolerance to milk sugar, common in non-Europeans), and fructose malabsorption.
- pernicious anemia, or impaired bowel function due to the inability to absorb vitamin B12,
- loss of pancreatic secretions, which may be due to cystic fibrosis or pancreatitis,
- structural defects, like short bowel syndrome (surgically removed bowel) and radiation fibrosis, such as usually follows cancer treatment and other drugs, including agents used in chemotherapy; and
- certain drugs, like orlistat, which inhibits the absorption of fat.
Inflammatory bowel disease
The two overlapping types here are of unknown origin:
- Ulcerative colitis is marked by chronic bloody diarrhea and inflammation mostly affects the distal colon near the rectum.
- Crohn's disease typically affects fairly well demarcated segments of bowel in the colon and often affects the end of the small bowel.
Irritable bowel syndrome
Another possible cause of diarrhea is irritable bowel syndrome (IBS), which usually presents with abdominal discomfort relieved by defecation and unusual stool (diarrhea or constipation) for at least three days a week over the previous three months.[43] Symptoms of diarrhea-predominant IBS can be managed through a combination of dietary changes, soluble fiber supplements and medications such as loperamide or codeine. About 30% of patients with diarrhea-predominant IBS have bile acid malabsorption diagnosed with an abnormal SeHCAT test.[44]
Other diseases
Diarrhea can be caused by other diseases and conditions, namely:
- Chronic ethanol ingestion[45]
- Hyperthyroidism[46]
- Certain medications[46]
- Bile acid malabsorption[46]
- Ischemic bowel disease: This usually affects older people and can be due to blocked arteries.
- Microscopic colitis, a type of inflammatory bowel disease where changes are seen only on histological examination of colonic biopsies.
- Bile salt malabsorption (primary bile acid diarrhea) where excessive bile acids in the colon produce a secretory diarrhea.
- Hormone-secreting tumors: some hormones, e.g. serotonin), can cause diarrhea if excreted in excess (usually from a tumor).
- Chronic mild diarrhea in infants and toddlers may occur with no obvious cause and with no other ill effects; this condition is called toddler's diarrhea.
- Environmental enteropathy
- Radiation enteropathy following treatment for pelvic and abdominal cancers.
Medications
Some medications, such as the penicillum can cause diarrhea.[47][48] Over 700 medications are known to cause diarrhea. The classes of medications that are known to cause diarrhea are laxatives, antacids, heartburn medications, antibiotics, anti-neoplastic drugs, anti-inflammatories as well as many dietary supplements.[16]
Pathophysiology
| Function | Transporter |
|---|---|
| Absorption | NHE, SGLT1, ENaC, DRA |
| Secretion | CaCC, NKCC1, CFTR |
| Absorption and secretion | Sodium potassium ATPase |
Evolution
According to two researchers, Nesse and Williams, diarrhea may function as an evolved expulsion defense mechanism. As a result, if it is stopped, there might be a delay in recovery.[50] They cite in support of this argument research published in 1973 that found that treating Shigella with the anti-diarrhea drug (Co-phenotrope, Lomotil) caused people to stay feverish twice as long as those not so treated. The researchers indeed themselves observed that: "Lomotil may be contraindicated in shigellosis. Diarrhea may represent a defense mechanism".[51]
Diagnostic approach
The following types of diarrhea may indicate further investigation is needed:
- In infants
- Moderate or severe diarrhea in young children
- Associated with blood
- Continues for more than two days
- Associated non-cramping abdominal pain, fever, weight loss, etc.
- In travelers
- In food handlers, because of the potential to infect others;
- In institutions such as hospitals, child care centers, or geriatric and convalescent homes.
A severity score is used to aid diagnosis in children.[52]
Chronic diarrhea
When diarrhea lasts for more than four weeks a number of further tests may be recommended including:[53]
- Complete blood count and a ferritin if anemia is present
- Thyroid stimulating hormone
- Tissue transglutaminase for celiac disease
- Fecal calprotectin to exclude inflammatory bowel disease
- Stool tests for ova and parasites as well as for Clostridioides difficile
- A colonoscopy or fecal immunochemical testing for cancer, including biopsies to detect microscopic colitis
- Testing for bile acid diarrhea with SeHCAT, 7α-hydroxy-4-cholesten-3-one or fecal bile acids depending on availability
- Hydrogen breath test looking for lactose intolerance
- Further tests if immunodeficiency, pelvic radiation disease or small intestinal bacterial overgrowth suspected.
A 2019 guideline recommended that testing for ova and parasites was only needed in people who are at high risk though they recommend routine testing for giardia.[54] Erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) were not recommended.[54]
Prevention
Sanitation
Numerous studies have shown that improvements in drinking water and sanitation (WASH) lead to decreased risks of diarrhoea.[55] Such improvements might include for example use of water filters, provision of high-quality piped water and sewer connections.[55]
In institutions, communities, and households, interventions that promote hand washing with soap lead to significant reductions in the incidence of diarrhea.[56] The same applies to preventing open defecation at a community-wide level and providing access to improved sanitation.[57][58] This includes use of toilets and implementation of the entire sanitation chain connected to the toilets (collection, transport, disposal or reuse of human excreta).
There is limited evidence that safe disposal of child or adult feces can prevent diarrheal disease.[59][60]
Hand washing
Basic sanitation techniques can have a profound effect on the transmission of diarrheal disease. The implementation of hand washing using soap and water, for example, has been experimentally shown to reduce the incidence of disease by approximately 42–48%.[61][62] Hand washing in developing countries, however, is compromised by poverty as acknowledged by the CDC: "Handwashing is integral to disease prevention in all parts of the world; however, access to soap and water is limited in a number of less developed countries. This lack of access is one of many challenges to proper hygiene in less developed countries." Solutions to this barrier require the implementation of educational programs that encourage sanitary behaviours.[63]
Water
Given that water contamination is a major means of transmitting diarrheal disease, efforts to provide clean water supply and improved sanitation have the potential to dramatically cut the rate of disease incidence. In fact, it has been proposed that we might expect an 88% reduction in child mortality resulting from diarrheal disease as a result of improved water sanitation and hygiene.[36][64] Similarly, a meta-analysis of numerous studies on improving water supply and sanitation shows a 22–27% reduction in disease incidence, and a 21–30% reduction in mortality rate associated with diarrheal disease.[65]
Chlorine treatment of water, for example, has been shown to reduce both the risk of diarrheal disease, and of contamination of stored water with diarrheal pathogens.[66]
Vaccination
Immunization against the pathogens that cause diarrheal disease is a viable prevention strategy, however it does require targeting certain pathogens for vaccination. In the case of Rotavirus, which was responsible for around 6% of diarrheal episodes and 20% of diarrheal disease deaths in the children of developing countries, use of a Rotavirus vaccine in trials in 1985 yielded a slight (2–3%) decrease in total diarrheal disease incidence, while reducing overall mortality by 6–10%. Similarly, a Cholera vaccine showed a strong reduction in morbidity and mortality, though the overall impact of vaccination was minimal as Cholera is not one of the major causative pathogens of diarrheal disease.[67] Since this time, more effective vaccines have been developed that have the potential to save many thousands of lives in developing nations, while reducing the overall cost of treatment, and the costs to society.[68][69]
Rotavirus vaccine decrease the rates of diarrhea in a population.[1][70] New vaccines against rotavirus, Shigella, Enterotoxigenic Escherichia coli (ETEC), and cholera are under development, as well as other causes of infectious diarrhea.
Nutrition
Dietary deficiencies in developing countries can be combated by promoting better eating practices. Zinc supplementation proved successful showing a significant decrease in the incidence of diarrheal disease compared to a control group.[71][72] The majority of the literature suggests that vitamin A supplementation is advantageous in reducing disease incidence.[73] Development of a supplementation strategy should take into consideration the fact that vitamin A supplementation was less effective in reducing diarrhea incidence when compared to vitamin A and zinc supplementation, and that the latter strategy was estimated to be significantly more cost effective.[74]
Breastfeeding
Breastfeeding practices have been shown to have a dramatic effect on the incidence of diarrheal disease in poor populations. Studies across a number of developing nations have shown that those who receive exclusive breastfeeding during their first 6 months of life are better protected against infection with diarrheal diseases.[75] One study in Brazil found that non-breastfed infants were 14 times more likely to die from diarrhea than exclusively breastfed infants.[76] Exclusive breastfeeding is currently recommended for the first six months of an infant's life by the WHO,[77][78] with continued breastfeeding until at least two years of age.[78]
Others
Probiotics decrease the risk of diarrhea in those taking antibiotics.[79] Insecticide spraying may reduce fly numbers and the risk of diarrhea in children in a setting where there is seasonal variations in fly numbers throughout the year.[80]
Management
In many cases of diarrhea, replacing lost fluid and salts is the only treatment needed. This is usually by mouth – oral rehydration therapy – or, in severe cases, intravenously.[1] Diet restrictions such as the BRAT diet are no longer recommended.[81] Research does not support the limiting of milk to children as doing so has no effect on duration of diarrhea.[82] To the contrary, WHO recommends that children with diarrhea continue to eat as sufficient nutrients are usually still absorbed to support continued growth and weight gain, and that continuing to eat also speeds up recovery of normal intestinal functioning.[17] CDC recommends that children and adults with cholera also continue to eat.[83] There is no evidence that early refeeding in children can cause an increase in inappropriate use of intravenous fluid, episodes of vomiting, and risk of having persistent diarrhea.[84]
Medications such as loperamide (Imodium) and bismuth subsalicylate may be beneficial; however they may be contraindicated in certain situations.[85]
Fluids

Oral rehydration solution (ORS) (a slightly sweetened and salty water) can be used to prevent dehydration. Standard home solutions such as salted rice water, salted yogurt drinks, vegetable and chicken soups with salt can be given. Home solutions such as water in which cereal has been cooked, unsalted soup, green coconut water, weak tea (unsweetened), and unsweetened fresh fruit juices can have from half a teaspoon to full teaspoon of salt (from one-and-a-half to three grams) added per liter. Clean plain water can also be one of several fluids given.[17] There are commercial solutions such as Pedialyte, and relief agencies such as UNICEF widely distribute packets of salts and sugar. A WHO publication for physicians recommends a homemade ORS consisting of one liter water with one teaspoon salt (3 grams) and two tablespoons sugar (18 grams) added[17] (approximately the "taste of tears"[86]). Rehydration Project recommends adding the same amount of sugar but only one-half a teaspoon of salt, stating that this more dilute approach is less risky with very little loss of effectiveness.[87] Both agree that drinks with too much sugar or salt can make dehydration worse.[17][87]
Appropriate amounts of supplemental zinc and potassium should be added if available. But the availability of these should not delay rehydration. As WHO points out, the most important thing is to begin preventing dehydration as early as possible.[17] In another example of prompt ORS hopefully preventing dehydration, CDC recommends for the treatment of cholera continuing to give Oral Rehydration Solution during travel to medical treatment.[83]
Vomiting often occurs during the first hour or two of treatment with ORS, especially if a child drinks the solution too quickly, but this seldom prevents successful rehydration since most of the fluid is still absorbed. WHO recommends that if a child vomits, to wait five or ten minutes and then start to give the solution again more slowly.[17]
Drinks especially high in simple sugars, such as soft drinks and fruit juices, are not recommended in children under five as they may increase dehydration. A too rich solution in the gut draws water from the rest of the body, just as if the person were to drink sea water.[17][88] Plain water may be used if more specific and effective ORT preparations are unavailable or are not palatable.[88] Additionally, a mix of both plain water and drinks perhaps too rich in sugar and salt can alternatively be given to the same person, with the goal of providing a medium amount of sodium overall.[17] A nasogastric tube can be used in young children to administer fluids if warranted.[89]
Eating
The WHO recommends a child with diarrhea continue to be fed. Continued feeding speeds the recovery of normal intestinal function. In contrast, children whose food is restricted have diarrhea of longer duration and recover intestinal function more slowly. The WHO states "Food should never be withheld and the child's usual foods should not be diluted. Breastfeeding should always be continued."[17] And in the specific example of cholera, CDC also makes the same recommendation.[83] Breastfed infants with diarrhea often choose to breastfeed more, and should be encouraged to do so.[17] In young children who are not breast-fed and live in the developed world, a lactose-free diet may be useful to speed recovery.[90] Eating food containing fibers may help.[91]
Medications
Antidiarrheal agents can be classified into four different groups: antimotility, antisecretory, adsorbent, and anti-infectious.[92] While antibiotics are beneficial in certain types of acute diarrhea, they are usually not used except in specific situations.[93][94] There are concerns that antibiotics may increase the risk of hemolytic uremic syndrome in people infected with Escherichia coli O157:H7.[95] In resource-poor countries, treatment with antibiotics may be beneficial.[94] However, some bacteria are developing antibiotic resistance, particularly Shigella.[96] Antibiotics can also cause diarrhea, and antibiotic-associated diarrhea is the most common adverse effect of treatment with general antibiotics.
While bismuth compounds (Pepto-Bismol) decreased the number of bowel movements in those with travelers' diarrhea, they do not decrease the length of illness.[97] Anti-motility agents like loperamide are also effective at reducing the number of stools but not the duration of disease.[8] These agents should be used only if bloody diarrhea is not present.[98]
Diosmectite, a natural aluminomagnesium silicate clay, is effective in alleviating symptoms of acute diarrhea in children,[99] and also has some effects in chronic functional diarrhea, radiation-induced diarrhea, and chemotherapy-induced diarrhea.[46] Another absorbent agent used for the treatment of mild diarrhea is kaopectate.
Racecadotril an antisecretory medication may be used to treat diarrhea in children and adults.[92] It has better tolerability than loperamide, as it causes less constipation and flatulence.[100] However, it has little benefit in improving acute diarrhea in children.[101]
Bile acid sequestrants such as cholestyramine can be effective in chronic diarrhea due to bile acid malabsorption. Therapeutic trials of these drugs are indicated in chronic diarrhea if bile acid malabsorption cannot be diagnosed with a specific test, such as SeHCAT retention.[102]
Alternative therapies
Zinc supplementation may benefit children over six months old with diarrhea in areas with high rates of malnourishment or zinc deficiency.[103] This supports the World Health Organization guidelines for zinc, but not in the very young.
A Cochrane Review from 2020 concludes that probiotics make little or no difference to people who have diarrhoea lasting 2 days or longer and that there is no proof that they reduce its duration.[104] The probiotic lactobacillus can help prevent antibiotic-associated diarrhea in adults but possibly not children.[105] For those with lactose intolerance, taking digestive enzymes containing lactase when consuming dairy products often improves symptoms.
Epidemiology
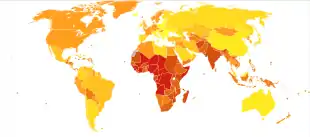
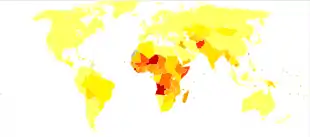
Worldwide in 2004, approximately 2.5 billion cases of diarrhea occurred, which resulted in 1.5 million deaths among children under the age of five.[1] Greater than half of these were in Africa and South Asia.[1] This is down from a death rate of 4.5 million in 1980 for gastroenteritis.[107] Diarrhea remains the second leading cause of infant mortality (16%) after pneumonia (17%) in this age group.[1]
The majority of such cases occur in the developing world, with over half of the recorded cases of childhood diarrhea occurring in Africa and Asia, with 696 million and 1.2 billion cases, respectively, compared to only 480 million in the rest of the world.[108]
Infectious diarrhea resulted in about 0.7 million deaths in children under five years old in 2011 and 250 million lost school days.[57][109] In the Americas, diarrheal disease accounts for a total of 10% of deaths among children aged 1–59 months while in South East Asia, it accounts for 31.3% of deaths.[110] It is estimated that around 21% of child mortalities in developing countries are due to diarrheal disease.[111]
Terminology
The word diarrhea is from the Ancient Greek διάρροια from διά dia "through" and ῥέω rheo "flow".
Diarrhea is the spelling in American English, whereas diarrhoea is the spelling in British English.
Slang terms for the condition include "the runs", "the squirts" (or "squits" in Britain[112]) and "the trots".[113][114]
See also
References
- "whqlibdoc.who.int" (PDF). World Health Organization. Archived (PDF) from the original on 8 November 2010.
- "Diarrhoeal disease Factsheet". World Health Organization. 2 May 2017. Retrieved 29 October 2020.
- GBD 2015 Disease and Injury Incidence and Prevalence Collaborators (October 2016). "Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
- GBD 2015 Mortality and Causes of Death Collaborators (October 2016). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1459–1544. doi:10.1016/s0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
- Abdelmalak B, Doyle J, eds. (2013). Anesthesia for otolaryngologic surgery. Cambridge University Press. pp. 282–287. ISBN 978-1-107-01867-9.
- Sapone A, Bai JC, Ciacci C, Dolinsek J, Green PH, Hadjivassiliou M, et al. (February 2012). "Spectrum of gluten-related disorders: consensus on new nomenclature and classification". BMC Medicine (Review). 10: 13. doi:10.1186/1741-7015-10-13. PMC 3292448. PMID 22313950.

- Slattery SA, Niaz O, Aziz Q, Ford AC, Farmer AD (July 2015). "Systematic review with meta-analysis: the prevalence of bile acid malabsorption in the irritable bowel syndrome with diarrhoea" (PDF). Alimentary Pharmacology & Therapeutics. 42 (1): 3–11. doi:10.1111/apt.13227. PMID 25913530. S2CID 34603226.
- DuPont HL (April 2014). "Acute infectious diarrhea in immunocompetent adults". The New England Journal of Medicine. 370 (16): 1532–40. doi:10.1056/nejmra1301069. PMID 24738670.
- Crockett ME, Keystone JS (2012). "Protection of Travelers". In Fischer M, Long SS, Prober CG (eds.). Principles and practice of pediatric infectious diseases (4th ed.). Edinburgh: Elsevier Saunders. p. 82. ISBN 978-1-4557-3985-1.
- ACEP. "Nation's Emergency Physicians Announce List of Test and Procedures to Question as Part of Choosing Wisely Campaign". Choosing Wisely. Archived from the original on 17 May 2014. Retrieved 18 June 2014.
- Global Burden of Disease Study 2013 Collaborators (August 2015). "Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013". Lancet. 386 (9995): 743–800. doi:10.1016/s0140-6736(15)60692-4. PMC 4561509. PMID 26063472.
- GBD 2013 Mortality and Causes of Death Collaborators (January 2015). "Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013". Lancet. 385 (9963): 117–71. doi:10.1016/S0140-6736(14)61682-2. PMC 4340604. PMID 25530442.
- "Global Diarrhea Burden". CDC. 24 January 2013. Archived from the original on 7 July 2014. Retrieved 18 June 2014.
- "WGO Practice Guideline – Acute diarrhea". Archived from the original on 22 February 2011. Retrieved 9 March 2011.
- "The Basics of Diarrhea". Webmd.com. 17 February 2011. Archived from the original on 11 March 2011. Retrieved 9 March 2011.
- Moon C, Zhang W, Sundaram N, Yarlagadda S, Reddy VS, Arora K, Helmrath MA, Naren AP (December 2015). "Drug-induced secretory diarrhea: A role for CFTR". Pharmacological Research. 102: 107–112. doi:10.1016/j.phrs.2015.08.024. PMC 4684461. PMID 26429773.
- "The Treatment Of Diarrhea, A manual for physicians and other senior health workers" (PDF). Sometimes needs to be downloaded twice. See "4.2 Treatment Plan A: home therapy to prevent dehydration and malnutrition," "4.3 Treatment Plan B: oral rehydration therapy for children with some dehydration," and "4.4 Treatment Plan C: for patients with severe dehydration" on pages 8 to 16 (12–20 in PDF). See also "8. Management of Diarrhoea with Severe Malnutrition" on pages 22–24 (26–30 in PDF) and "Annex 2: Oral and Intravenous Rehydration Solutions" on pages 33–37 (37–41 in PDF). World Health Organization. 2005. Archived (PDF) from the original on 19 October 2011.
- Sweetser S (June 2012). "Evaluating the patient with diarrhea: a case-based approach". Mayo Clinic Proceedings. 87 (6): 596–602. doi:10.1016/j.mayocp.2012.02.015. PMC 3538472. PMID 22677080.
- Disease Control Priorities Project. "Public Health Significance of Diarrheal Illnesses". The World Bank Group. Archived from the original on 25 January 2014. Retrieved 12 October 2013.
- Guerrant RL, Schorling JB, McAuliffe JF, de Souza MA (July 1992). "Diarrhea as a cause and an effect of malnutrition: diarrhea prevents catch-up growth and malnutrition increases diarrhea frequency and duration". The American Journal of Tropical Medicine and Hygiene. 47 (1 Pt 2): 28–35. doi:10.4269/ajtmh.1992.47.28. PMID 1632474.
- Grantham-McGregor SM, Walker SP, Chang S (February 2000). "Nutritional deficiencies and later behavioural development". The Proceedings of the Nutrition Society. 59 (1): 47–54. doi:10.1017/S0029665100000069. PMID 10828173.
- Maton, Anthea; Jean Hopkins; Charles William McLaughlin; Susan Johnson; Maryanna Quon Warner; David LaHart; Jill D. Wright (1993). Human Biology and Health. Englewood Cliffs, NJ: Prentice Hall. ISBN 978-0-13-981176-0. OCLC 32308337.
- Wilson ME (December 2005). "Diarrhea in nontravelers: risk and etiology". Clinical Infectious Diseases. 41. 41 Suppl 8 (Suppl 8): S541-6. doi:10.1086/432949. PMID 16267716.
- Navaneethan U, Giannella RA (November 2008). "Mechanisms of infectious diarrhea". Nature Clinical Practice. Gastroenterology & Hepatology. 5 (11): 637–47. doi:10.1038/ncpgasthep1264. PMID 18813221. S2CID 34096072.
- Schlossberg D (2008). Clinical Infectious Disease. Cambridge University Press. p. 349. ISBN 978-1-139-57665-9.
- Patel MM, Hall AJ, Vinjé J, Parashar UD (January 2009). "Noroviruses: a comprehensive review". Journal of Clinical Virology. 44 (1): 1–8. doi:10.1016/j.jcv.2008.10.009. PMID 19084472.
- Greenberg HB, Estes MK (May 2009). "Rotaviruses: from pathogenesis to vaccination". Gastroenterology. 136 (6): 1939–51. doi:10.1053/j.gastro.2009.02.076. PMC 3690811. PMID 19457420.
- Uhnoo I, Svensson L, Wadell G (September 1990). "Enteric adenoviruses". Baillière's Clinical Gastroenterology. 4 (3): 627–42. doi:10.1016/0950-3528(90)90053-J. PMID 1962727.
- Mitchell DK (November 2002). "Astrovirus gastroenteritis". The Pediatric Infectious Disease Journal. 21 (11): 1067–9. doi:10.1097/00006454-200211000-00018. PMID 12442031.
- Viswanathan VK, Hodges K, Hecht G (February 2009). "Enteric infection meets intestinal function: how bacterial pathogens cause diarrhoea". Nature Reviews. Microbiology. 7 (2): 110–9. doi:10.1038/nrmicro2053. PMC 3326399. PMID 19116615.
- Rupnik M, Wilcox MH, Gerding DN (July 2009). "Clostridium difficile infection: new developments in epidemiology and pathogenesis". Nature Reviews. Microbiology. 7 (7): 526–36. doi:10.1038/nrmicro2164. PMID 19528959. S2CID 23376891.
- Rossignol JF, Lopez-Chegne N, Julcamoro LM, Carrion ME, Bardin MC (March 2012). "Nitazoxanide for the empiric treatment of pediatric infectious diarrhea". Transactions of the Royal Society of Tropical Medicine and Hygiene. 106 (3): 167–73. doi:10.1016/j.trstmh.2011.11.007. PMID 22301075.
- Alam NH, Ashraf H (2003). "Treatment of infectious diarrhea in children". Paediatric Drugs. 5 (3): 151–65. doi:10.2165/00128072-200305030-00002. PMID 12608880. S2CID 26076784.
- "WHO | Diarrhoeal disease". Who.int. Archived from the original on 1 April 2014. Retrieved 10 March 2014.
- Jamison, Dean T. (2006). Disease control priorities in developing countries (2nd ed.). New York: Oxford Univ. Press. ISBN 978-0-8213-6179-5.
- Brown J, Cairncross S, Ensink JH (August 2013). "Water, sanitation, hygiene and enteric infections in children". Archives of Disease in Childhood. 98 (8): 629–34. doi:10.1136/archdischild-2011-301528. PMC 3717778. PMID 23761692.
- Black RE, Sazawal S (May 2001). "Zinc and childhood infectious disease morbidity and mortality". The British Journal of Nutrition. 85 Suppl 2: S125-9. doi:10.1079/bjn2000304. PMID 11509100.
- Shankar AH, Prasad AS (August 1998). "Zinc and immune function: the biological basis of altered resistance to infection". The American Journal of Clinical Nutrition. 68 (2 Suppl): 447S–463S. doi:10.1093/ajcn/68.2.447S. PMID 9701160.
- Bahl R, Bhandari N, Hambidge KM, Bhan MK (August 1998). "Plasma zinc as a predictor of diarrheal and respiratory morbidity in children in an urban slum setting". The American Journal of Clinical Nutrition. 68 (2 Suppl): 414S–417S. doi:10.1093/ajcn/68.2.414S. PMID 9701154.
- Rice AL, West KP, Black RE (2004). "Vitamin A deficiency" (PDF). In Ezzati M, Lopez AD, Rodgers A, Murray CJ (eds.). Comparative quantification of health risks: global and regional burden of disease attributes to selected major risk factors. 1. Geneva: World Health Organization. pp. 211–56, especially 238–240.
- Sommer A, Katz J, Tarwotjo I (November 1984). "Increased risk of respiratory disease and diarrhea in children with preexisting mild vitamin A deficiency". The American Journal of Clinical Nutrition. 40 (5): 1090–5. doi:10.1093/ajcn/40.5.1090. PMID 6496388.
- West KP (September 2002). "Extent of vitamin A deficiency among preschool children and women of reproductive age". The Journal of Nutrition. 132 (9 Suppl): 2857S–2866S. doi:10.1093/jn/132.9.2857S. PMID 12221262.
- Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC (April 2006). "Functional bowel disorders". Gastroenterology. 130 (5): 1480–91. doi:10.1053/j.gastro.2005.11.061. PMID 16678561.
- Wedlake L, A'Hern R, Russell D, Thomas K, Walters JR, Andreyev HJ (October 2009). "Systematic review: the prevalence of idiopathic bile acid malabsorption as diagnosed by SeHCAT scanning in patients with diarrhoea-predominant irritable bowel syndrome". Alimentary Pharmacology & Therapeutics. 30 (7): 707–17. doi:10.1111/j.1365-2036.2009.04081.x. PMID 19570102. S2CID 11327665.
- Kasper DL, Braunwald E, Fauci AS, Hauser SL, Longo DL, Jameson JL (2005). Harrison's Principles of Internal Medicine. New York: McGraw-Hill. ISBN 978-0-07-139140-5.
- Lee KJ (October 2015). "Pharmacologic Agents for Chronic Diarrhea". Intestinal Research. 13 (4): 306–12. doi:10.5217/ir.2015.13.4.306. PMC 4641856. PMID 26576135.
- Vallerand A (2017). Davis's drug guide for nurses. Philadelphia: F.A. Davis Company. pp. 989–994. ISBN 978-0-8036-5705-2.
- Dekel R, Sperber AD. "Diarrhea & Incontinence Caused by Medication". International Foundation for Gastrointestinal Disorders (IFFGD). Archived from the original on 24 February 2017. Retrieved 18 May 2017.
- Das S, Jayaratne R, Barrett KE (2018). "The Role of Ion Transporters in the Pathophysiology of Infectious Diarrhea". Cellular and Molecular Gastroenterology and Hepatology. 6 (1): 33–45. doi:10.1016/j.jcmgh.2018.02.009. PMC 6007821. PMID 29928670.
- Williams G, Nesse RM (1996). Why we get sick: the new science of Darwinian medicine. New York: Vintage Books. pp. 36–38. ISBN 978-0-679-74674-4.
- DuPont HL, Hornick RB (December 1973). "Adverse effect of lomotil therapy in shigellosis". JAMA. 226 (13): 1525–8. doi:10.1001/jama.226.13.1525. PMID 4587313.
- Ruuska T, Vesikari T (1990). "Rotavirus disease in Finnish children: use of numerical scores for clinical severity of diarrhoeal episodes". Scandinavian Journal of Infectious Diseases. 22 (3): 259–67. doi:10.3109/00365549009027046. PMID 2371542.
- Arasaradnam RP, Brown S, Forbes A, Fox MR, Hungin P, Kelman L, et al. (August 2018). "Guidelines for the investigation of chronic diarrhoea in adults: British Society of Gastroenterology, 3rd edition". Gut. 67 (8): 1380–1399. doi:10.1136/gutjnl-2017-315909. PMC 6204957. PMID 29653941.
- Smalley W, Falck-Ytter C, Carrasco-Labra A, Wani S, Lytvyn L, Falck-Ytter Y (September 2019). "AGA Clinical Practice Guidelines on the Laboratory Evaluation of Functional Diarrhea and Diarrhea-Predominant Irritable Bowel Syndrome in Adults (IBS-D)". Gastroenterology. 157 (3): 851–854. doi:10.1053/j.gastro.2019.07.004. PMID 31302098.
- Wolf J, Prüss-Ustün A, Cumming O, Bartram J, Bonjour S, Cairncross S, et al. (August 2014). "Assessing the impact of drinking water and sanitation on diarrhoeal disease in low- and middle-income settings: systematic review and meta-regression" (PDF). Tropical Medicine & International Health. 19 (8): 928–42. doi:10.1111/tmi.12331. PMID 24811732. S2CID 22903164.
- Ejemot-Nwadiaro RI, Ehiri JE, Arikpo D, Meremikwu MM, Critchley JA (September 2015). "Hand washing promotion for preventing diarrhoea". The Cochrane Database of Systematic Reviews (9): CD004265. doi:10.1002/14651858.CD004265.pub3. PMC 4563982. PMID 26346329.
- "Call to action on sanitation" (PDF). United Nations. Archived from the original (PDF) on 19 August 2014. Retrieved 15 August 2014.
- Spears D, Ghosh A, Cumming O (2013). "Open defecation and childhood stunting in India: an ecological analysis of new data from 112 districts". PLOS ONE. 8 (9): e73784. Bibcode:2013PLoSO...873784S. doi:10.1371/journal.pone.0073784. PMC 3774764. PMID 24066070.
- Majorin F, Torondel B, Ka Seen Chan G, Clasen T, et al. (Cochrane Infectious Diseases Group) (September 2019). "Interventions to improve disposal of child faeces for preventing diarrhoea and soil-transmitted helminth infection". The Cochrane Database of Systematic Reviews. 9: CD011055. doi:10.1002/14651858.CD011055.pub2. PMC 6757260. PMID 31549742.
- Clasen TF, Bostoen K, Schmidt WP, Boisson S, Fung IC, Jenkins MW, et al. (Cochrane Infectious Diseases Group) (June 2010). "Interventions to improve disposal of human excreta for preventing diarrhoea". The Cochrane Database of Systematic Reviews (6): CD007180. doi:10.1002/14651858.CD007180.pub2. PMC 6532559. PMID 20556776.
- Curtis V, Cairncross S (May 2003). "Effect of washing hands with soap on diarrhoea risk in the community: a systematic review". The Lancet. Infectious Diseases. 3 (5): 275–81. doi:10.1016/S1473-3099(03)00606-6. PMID 12726975.
- Cairncross S, Hunt C, Boisson S, Bostoen K, Curtis V, Fung IC, Schmidt WP (April 2010). "Water, sanitation and hygiene for the prevention of diarrhoea". International Journal of Epidemiology. 39 Suppl 1 (Suppl 1): i193-205. doi:10.1093/ije/dyq035. PMC 2845874. PMID 20348121.
- "Diarrheal Diseases in Less Developed Countries". CDC. Archived from the original on 4 November 2013. Retrieved 28 October 2013.
- Black RE, Morris SS, Bryce J (June 2003). "Where and why are 10 million children dying every year?". Lancet. 361 (9376): 2226–34. doi:10.1016/S0140-6736(03)13779-8. PMID 12842379. S2CID 14509705.
- Esrey SA, Feachem RG, Hughes JM (1985). "Interventions for the control of diarrhoeal diseases among young children: improving water supplies and excreta disposal facilities". Bulletin of the World Health Organization. 63 (4): 757–72. PMC 2536385. PMID 3878742.
- Arnold BF, Colford JM (February 2007). "Treating water with chlorine at point-of-use to improve water quality and reduce child diarrhea in developing countries: a systematic review and meta-analysis". The American Journal of Tropical Medicine and Hygiene. 76 (2): 354–64. doi:10.4269/ajtmh.2007.76.354. PMID 17297049.
- de Zoysa I, Feachem RG (1985). "Interventions for the control of diarrhoeal diseases among young children: rotavirus and cholera immunization". Bulletin of the World Health Organization. 63 (3): 569–83. PMC 2536413. PMID 3876173.
- Rheingans RD, Antil L, Dreibelbis R, Podewils LJ, Bresee JS, Parashar UD (November 2009). "Economic costs of rotavirus gastroenteritis and cost-effectiveness of vaccination in developing countries". The Journal of Infectious Diseases. 200 Suppl 1: S16-27. doi:10.1086/605026. PMID 19817595.
- Oral cholera vaccines in mass immunization campaigns (PDF). WHO. 2010. pp. 6–8. ISBN 978-92-4-150043-2. Archived (PDF) from the original on 3 September 2014.
- Soares-Weiser K, Goldberg E, Tamimi G, Pitan OC, Leibovici L, et al. (Cochrane Infectious Diseases Group) (26 January 2004). "Rotavirus vaccine for preventing diarrhoea". The Cochrane Database of Systematic Reviews (1): CD002848. doi:10.1002/14651858.CD002848.pub2. PMC 6532746. PMID 14973994.
- Black RE (May 2003). "Zinc deficiency, infectious disease and mortality in the developing world". The Journal of Nutrition. 133 (5 Suppl 1): 1485S–9S. doi:10.1093/jn/133.5.1485S. PMID 12730449.
- Bhutta ZA, Black RE, Brown KH, Gardner JM, Gore S, Hidayat A, et al. (December 1999). "Prevention of diarrhea and pneumonia by zinc supplementation in children in developing countries: pooled analysis of randomized controlled trials. Zinc Investigators' Collaborative Group". The Journal of Pediatrics. 135 (6): 689–97. doi:10.1016/S0022-3476(99)70086-7. PMID 10586170.
- Mayo-Wilson E, Imdad A, Herzer K, Yakoob MY, Bhutta ZA (August 2011). "Vitamin A supplements for preventing mortality, illness, and blindness in children aged under 5: systematic review and meta-analysis". BMJ. 343: d5094. doi:10.1136/bmj.d5094. PMC 3162042. PMID 21868478.
- Chhagan MK, Van den Broeck J, Luabeya KK, Mpontshane N, Bennish ML (September 2014). "Cost of childhood diarrhoea in rural South Africa: exploring cost-effectiveness of universal zinc supplementation". Public Health Nutrition. 17 (9): 2138–45. doi:10.1017/S1368980013002152. PMID 23930984.
- "Effect of breastfeeding on infant and child mortality due to infectious diseases in less developed countries: a pooled analysis. WHO Collaborative Study Team on the Role of Breastfeeding on the Prevention of Infant Mortality". Lancet. 355 (9202): 451–5. February 2000. doi:10.1016/S0140-6736(00)82011-5. PMID 10841125. S2CID 30952224.
- Lawrence R (2016). Breastfeeding : a guide for the medical profession, 8th edition. Philadelphia, PA: Elsevier. p. 28. ISBN 978-0-323-35776-0.
- Sguassero Y. "Optimal duration of exclusive breastfeeding: RHL commentary". WHO. Archived from the original on 3 November 2013. Retrieved 14 October 2013.
- "Infant and young child feeding". World Health Organization. 3 October 2017. Retrieved 5 January 2018.
- Hempel S, Newberry SJ, Maher AR, Wang Z, Miles JN, Shanman R, Johnsen B, Shekelle PG (May 2012). "Probiotics for the prevention and treatment of antibiotic-associated diarrhea: a systematic review and meta-analysis". JAMA: The Journal of the American Medical Association. 307 (18): 1959–69. doi:10.1001/jama.2012.3507. PMID 22570464.
- Das JK, Hadi YB, Salam RA, Hoda M, Lassi ZS, Bhutta ZA, et al. (Cochrane Infectious Diseases Group) (December 2018). "Fly control to prevent diarrhoea in children". The Cochrane Database of Systematic Reviews. 12: CD011654. doi:10.1002/14651858.CD011654.pub2. PMC 6302900. PMID 30556598.
- King CK, Glass R, Bresee JS, Duggan C (November 2003). "Managing acute gastroenteritis among children: oral rehydration, maintenance, and nutritional therapy". MMWR. Recommendations and Reports. 52 (RR-16): 1–16. PMID 14627948. Archived from the original on 28 October 2014.
- "BestBets: Does Withholding milk feeds reduce the duration of diarrhoea in children with acute gastroenteritis?". Archived from the original on 4 May 2009.
- Community Health Worker Training Materials for Cholera Prevention and Control Archived 20 October 2011 at the Wayback Machine, CDC, slides at back are dated 17 November 2010. Page 7 states "... Continue to breastfeed your baby if the baby has watery diarrhea, even when traveling to get treatment. Adults and older children should continue to eat frequently."
- Gregorio GV, Dans LF, Silvestre MA, et al. (Cochrane Infectious Diseases Group) (July 2011). "Early versus Delayed Refeeding for Children with Acute Diarrhoea". The Cochrane Database of Systematic Reviews (7): CD007296. doi:10.1002/14651858.CD007296.pub2. PMC 6532715. PMID 21735409.
- Schiller LR (2007). "Management of diarrhea in clinical practice: strategies for primary care physicians". Reviews in Gastroenterological Disorders. 7 Suppl 3 (Suppl 3): S27-38. PMID 18192963.
- A Guide on Safe Food for Travellers Archived 9 July 2012 at the Wayback Machine, Welcome to South Africa, Host to the 2010 FIFA World Cup (bottom left of page 1).
- Rehydration Project, "Diarrhoea, Diarrhea, Dehydration, Oral Rehydration, Mother and Child Nutrition, Water, Sanitation, Hygiene – Rehydration Project". Archived from the original on 8 June 2015. Retrieved 22 June 2015. Homemade Oral Rehydration Solution Recipe.
- "Management of acute diarrhoea and vomiting due to gastroenteritis in children under 5". National Institute of Clinical Excellence. April 2009. Archived from the original on 2 August 2009.
- Webb A, Starr M (April 2005). "Acute gastroenteritis in children". Australian Family Physician. 34 (4): 227–31. PMID 15861741.
- MacGillivray S, Fahey T, McGuire W (October 2013). "Lactose avoidance for young children with acute diarrhoea". The Cochrane Database of Systematic Reviews. 10 (10): CD005433. doi:10.1002/14651858.CD005433.pub2. PMC 4276385. PMID 24173771.
- "The Facts About Fiber".
- Guarino A, Lo Vecchio A, Pirozzi MR. (2009). "Clinical role of diosmectite in the management of diarrhea". Expert Opin Drug Metab Toxicol. 5 (4): 433–440. doi:10.1517/17425250902865594. PMID 19379128. S2CID 56519371.CS1 maint: uses authors parameter (link)
- Dryden MS, Gabb RJ, Wright SK (June 1996). "Empirical treatment of severe acute community-acquired gastroenteritis with ciprofloxacin". Clinical Infectious Diseases. 22 (6): 1019–25. doi:10.1093/clinids/22.6.1019. PMID 8783703.
- de Bruyn G (March 2008). "Diarrhoea in adults (acute)". BMJ Clinical Evidence. 2008: 0901. PMC 2907942. PMID 19450323.
- Wong CS, Jelacic S, Habeeb RL, Watkins SL, Tarr PI (June 2000). "The risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections". The New England Journal of Medicine. 342 (26): 1930–6. doi:10.1056/NEJM200006293422601. PMC 3659814. PMID 10874060.
- "Diarrhoeal Diseases". World Health Organization. February 2009. Archived from the original on 15 December 2008.
- DuPont HL, Ericsson CD, Farthing MJ, Gorbach S, Pickering LK, Rombo L, Steffen R, Weinke T (2009). "Expert review of the evidence base for self-therapy of travelers' diarrhea". Journal of Travel Medicine. 16 (3): 161–71. doi:10.1111/j.1708-8305.2009.00300.x. PMID 19538576.
- Pawlowski SW, Warren CA, Guerrant R (May 2009). "Diagnosis and treatment of acute or persistent diarrhea". Gastroenterology. 136 (6): 1874–86. doi:10.1053/j.gastro.2009.02.072. PMC 2723735. PMID 19457416.
- Dupont C, Vernisse B (2009). "Anti-diarrheal effects of diosmectite in the treatment of acute diarrhea in children: a review". Paediatric Drugs. 11 (2): 89–99. doi:10.2165/00148581-200911020-00001. PMC 7100234. PMID 19301931.
- Dinnendahl V, Fricke U (eds.). Arzneistoff-Profile (in German). Eschborn, Germany: Govi Pharmazeutischer Verlag. ISBN 978-3-7741-9846-3.
- Liang Y, Zhang L, Zeng L, Gordon M, Wen J, et al. (Cochrane Infectious Diseases Group) (December 2019). "Racecadotril for acute diarrhoea in children". The Cochrane Database of Systematic Reviews. 12: CD009359. doi:10.1002/14651858.CD009359.pub2. PMC 6923519. PMID 31858591.
- Wilcox C, Turner J, Green J (May 2014). "Systematic review: the management of chronic diarrhoea due to bile acid malabsorption". Alimentary Pharmacology & Therapeutics. 39 (9): 923–39. doi:10.1111/apt.12684. PMID 24602022. S2CID 12016216.
- Lazzerini M, Wanzira H (December 2016). "Oral zinc for treating diarrhoea in children". The Cochrane Database of Systematic Reviews. 12 (12): CD005436. doi:10.1002/14651858.CD005436.pub5. PMC 5450879. PMID 27996088.
- Collinson S , Deans A , Padua-Zamora A , Gregorio 3GV, Li 4C, Dans LF , Allen SJ (8 December 2020). "Probiotics for treating acute infectious diarrhoea". Cochrane Database Syst Rev.CS1 maint: multiple names: authors list (link)
- Kale-Pradhan PB, Jassal HK, Wilhelm SM (February 2010). "Role of Lactobacillus in the prevention of antibiotic-associated diarrhea: a meta-analysis". Pharmacotherapy. 30 (2): 119–26. doi:10.1592/phco.30.2.119. PMID 20099986. S2CID 21836205.
- "Mortality and Burden of Disease Estimates for WHO Member States in 2004" (xls). World Health Organization.
- Mandell GL, Bennett JE, Dolin R (2004). Mandell's Principles and Practices of Infection Diseases (6th ed.). Churchill Livingstone. ISBN 978-0-443-06643-6. Archived from the original on 18 October 2013.
- "Diarrhoea: why children are still dying and what can be done" (PDF). World Health Organization. Archived (PDF) from the original on 19 October 2013. Retrieved 12 October 2013.
- Walker CL, Rudan I, Liu L, Nair H, Theodoratou E, Bhutta ZA, O'Brien KL, Campbell H, Black RE (April 2013). "Global burden of childhood pneumonia and diarrhoea". Lancet. 381 (9875): 1405–1416. doi:10.1016/S0140-6736(13)60222-6. PMC 7159282. PMID 23582727.
- Walker CL, Aryee MJ, Boschi-Pinto C, Black RE (2012). "Estimating diarrhea mortality among young children in low and middle income countries". PLOS ONE. 7 (1): e29151. Bibcode:2012PLoSO...729151F. doi:10.1371/journal.pone.0029151. PMC 3250411. PMID 22235266.
- Kosek M, Bern C, Guerrant RL (2003). "The global burden of diarrhoeal disease, as estimated from studies published between 1992 and 2000". Bulletin of the World Health Organization. 81 (3): 197–204. PMC 2572419. PMID 12764516.
-
 The dictionary definition of squits at Wiktionary
The dictionary definition of squits at Wiktionary - The dictionary definition of runs at Wiktionary
- "Definition of Diarrhea by Merriam-Webster". Merriam Webster. Retrieved 11 December 2018.
External links
| Classification | |
|---|---|
| External resources |