Herpes labialis
Herpes labialis, commonly known as cold sores, is a type of infection by the herpes simplex virus that affects primarily the lip.[1] Symptoms typically include a burning pain followed by small blisters or sores.[1] The first attack may also be accompanied by fever, sore throat, and enlarged lymph nodes.[1][9] The rash usually heals within ten days, but the virus remains dormant in the trigeminal ganglion.[1] The virus may periodically reactivate to create another outbreak of sores in the mouth or lip.[1]
| Herpes labialis | |
|---|---|
| Other names | Cold sores,[1] fever blisters,[1] herpes simplex labialis,[2] recurrent herpes labialis,[3] orolabial herpes[4] |
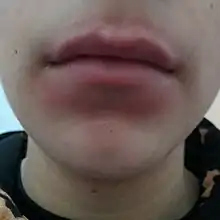
.jpg.webp) | |
| Herpes labialis of the lower lip. Note the blisters in a group marked by an arrow. | |
| Specialty | Infectious disease |
| Symptoms | Burning pain followed by small blisters or sores[1] |
| Complications | Herpes encephalitis, herpetic whitlow[5] |
| Usual onset | < 20 years old[1] |
| Duration | Heals within 10 days[1] |
| Causes | Typically herpes simplex virus type 1 (direct contact)[1][6] |
| Diagnostic method | Usually based on symptoms[1] |
| Differential diagnosis | Herpangina, aphthous stomatitis, impetigo, mononucleosis[7] |
| Prevention | Avoiding exposure, antiviral medication[3][8] |
| Treatment | Zinc oxide, anesthetic, or antiviral cream,[1] antivirals by mouth[3] |
| Prognosis | Good[1] |
| Frequency | 2.5 per 1,000 affected per year[1] |
The cause is usually herpes simplex virus type 1 (HSV-1) and occasionally herpes simplex virus type 2 (HSV-2).[1] The infection is typically spread between people by direct non-sexual contact.[6] Attacks can be triggered by sunlight, fever, psychological stress, or a menstrual period.[1][9] Direct contact with the genitals can result in genital herpes.[1] Diagnosis is usually based on symptoms but can be confirmed with specific testing.[1][9]
Prevention includes avoiding kissing or using the personal items of a person who is infected.[8] A zinc oxide, anesthetic, or antiviral cream appears to decrease the duration of symptoms by a small amount.[1] Antiviral medications may also decrease the frequency of outbreaks.[1][3]
About 2.5 per 1000 people are affected with outbreaks in any given year.[1] After one episode about 33% of people develop subsequent episodes.[1] Onset often occurs in those less than 20 years old and 80% develop antibodies for the virus by this age.[1] In those with recurrent outbreaks, these typically happen less than three times a year.[10] The frequency of outbreaks generally decreases over time.[1]
Terminology
The term labia means "lip". Herpes labialis does not refer to the labia of the genitals, though the origin of the word is the same. When the viral infection affects both face and mouth, the broader term orofacial herpes is used, whereas herpetic stomatitis describes infection of the mouth specifically; stomatitis is derived from the Greek word stoma, which means "mouth".
Signs and symptoms
Herpes infections usually show no symptoms;[1] when symptoms do appear they typically resolve within two weeks.[11] The main symptom of oral infection is inflammation of the mucosa of the cheek and gums—known as acute herpetic gingivostomatitis—which occurs within 5–10 days of infection. Other symptoms may also develop, including headache, nausea, dizziness and painful ulcers—sometimes confused with canker sores—fever, and sore throat.[11]
Primary HSV infection in adolescents frequently manifests as severe pharyngitis with lesions developing on the cheek and gums. Some individuals develop difficulty in swallowing (dysphagia) and swollen lymph nodes (lymphadenopathy).[11] Primary HSV infections in adults often results in pharyngitis similar to that observed in glandular fever (infectious mononucleosis), but gingivostomatitis is less likely.
Recurrent oral infection is more common with HSV-1 infections than with HSV-2. Symptoms typically progress in a series of eight stages:
- Latent (weeks to months incident-free): The remission period; After initial infection, the viruses move to sensory nerve ganglia (trigeminal ganglion),[12] where they reside as lifelong, latent viruses. Asymptomatic shedding of contagious virus particles can occur during this stage.
- Prodromal (day 0–1): Symptoms often precede a recurrence. Symptoms typically begin with tingling (itching) and reddening of the skin around the infected site. This stage can last from a few days to a few hours preceding the physical manifestation of an infection and is the best time to start treatment.
- Inflammation (day 1): Virus begins reproducing and infecting cells at the end of the nerve. The healthy cells react to the invasion with swelling and redness displayed as symptoms of infection.
- Pre-sore (day 2–3): This stage is defined by the appearance of tiny, hard, inflamed papules and vesicles that may itch and are painfully sensitive to touch. In time, these fluid-filled blisters form a cluster on the lip (labial) tissue, the area between the lip and skin (vermilion border), and can occur on the nose, chin, and cheeks.
- Open lesion (day 4): This is the most painful and contagious of the stages. All the tiny vesicles break open and merge to create one big, open, weeping ulcer. Fluids are slowly discharged from blood vessels and inflamed tissue. This watery discharge is teeming with active viral particles and is highly contagious. Depending on the severity, one may develop a fever and swollen lymph glands under the jaw.[13]
- Crusting (day 5–8): A honey/golden crust starts to form from the syrupy exudate. This yellowish or brown crust or scab is not made of active virus but from blood serum containing useful proteins such as immunoglobulins. This appears as the healing process begins. The sore is still painful at this stage, but, more painful, however, is the constant cracking of the scab as one moves or stretches their lips, as in smiling or eating. Virus-filled fluid will still ooze out of the sore through any cracks.
- Healing (day 9–14): New skin begins to form underneath the scab as the virus retreats into latency. A series of scabs will form over the sore (called Meier Complex), each one smaller than the last. During this phase irritation, itching, and some pain are common.
- Post-scab (12–14 days): A reddish area may linger at the site of viral infection as the destroyed cells are regenerated. Virus shedding can still occur during this stage.
The recurrent infection is thus often called herpes simplex labialis. Rare reinfections occur inside the mouth (intraoral HSV stomatitis) affecting the gums, alveolar ridge, hard palate, and the back of the tongue, possibly accompanied by herpes labialis.[11]
A lesion caused by herpes simplex can occur in the corner of the mouth and be mistaken for angular cheilitis of another cause. Sometimes termed "angular herpes simplex".[14] A cold sore at the corner of the mouth behaves similarly to elsewhere on the lips. Rather than utilizing antifungal creams, angular herpes simplex is treated in the same way as a cold sore, with topical antiviral drugs.
Causes
Herpes labialis infection occurs when the herpes simplex virus comes into contact with oral mucosal tissue or abraded skin of the mouth. Infection by the type 1 strain of herpes simplex virus (HSV-1) is most common; however, cases of oral infection by the type 2 strain are increasing.[11] Specifically, type 2 has been implicated as causing 10–15% of oral infections.
Cold sores are the result of the virus reactivating in the body. Once HSV-1 has entered the body, it never leaves. The virus moves from the mouth to remain latent in the central nervous system. In approximately one-third of people, the virus can "wake up" or reactivate to cause disease. When reactivation occurs, the virus travels down the nerves to the skin where it may cause blisters (cold sores) around the lips, in the mouth or, in about 10% of cases, on the nose, chin, or cheeks.
Cold sore outbreaks may be influenced by stress, menstruation, sunlight, sunburn, fever, dehydration, or local skin trauma. Surgical procedures such as dental or neural surgery, lip tattooing, or dermabrasion are also common triggers. HSV-1 can in rare cases be transmitted to newborn babies by family members or hospital staff who have cold sores; this can cause a severe disease called neonatal herpes simplex.
The colloquial term for this condition, "cold sore" comes from the fact that herpes labialis is often triggered by fever, for example, as may occur during an upper respiratory tract infection (i.e. a cold).[15]
People can transfer the virus from their cold sores to other areas of the body, such as the eye, skin, or fingers; this is called autoinoculation. Eye infection, in the form of conjunctivitis or keratitis, can happen when the eyes are rubbed after touching the lesion. Finger infection (herpetic whitlow) can occur when a child with cold sores or primary HSV-1 infection sucks their fingers.
Blood tests for herpes may differentiate between type 1 and type 2. When a person is not experiencing any symptoms, a blood test alone does not reveal the site of infection. Genital herpes infections occurred with almost equal frequency as type 1 or 2 in younger adults when samples were taken from genital lesions. Herpes in the mouth is more likely to be caused by type 1, but (see above) also can be type 2. The only way to know for certain if a positive blood test for herpes is due to infection of the mouth, genitals, or elsewhere, is to sample from lesions. This is not possible if the afflicted individual is asymptomatic. The body's immune system typically fight the virus.[16]
Prevention
The likelihood of the infection being spread can be reduced through behaviors such as avoiding touching an active outbreak site, washing hands frequently while the outbreak is occurring, not sharing items that come in contact with the mouth, and not coming into close contact with others (by avoiding kissing, oral sex, or contact sports).
Because the onset of an infection is difficult to predict, lasts a short period of time and heals rapidly, it is difficult to conduct research on cold sores. Though famciclovir improves lesion healing time, it is not effective in preventing lesions; valaciclovir and a mixture of acyclovir and hydrocortisone are similarly useful in treating outbreaks but may also help prevent them.[17]
Acyclovir and valacyclovir by mouth are effective in preventing recurrent herpes labialis if taken prior to the onset of any symptoms or exposure to any triggers.[3][18] Evidence does not support L-lysine.[19]
Treatment
Despite no cure or vaccine for the virus, a human body's immune system and specialty antigens typically fight the virus.[16] Docosanol, a saturated fatty alcohol, is a safe and effective topical application that has been approved by the United States Food and Drug Administration for herpes labialis in adults with properly functioning immune systems. It is comparable in effectiveness to prescription topical antiviral agents. Due to its mechanism of action, there is little risk of drug resistance.[20] The duration of symptoms can be shortened a bit if an antiviral, anesthetic, zinc oxide or zinc sulfate cream is applied soon after it starts.[12]
Effective antiviral medications include acyclovir and penciclovir, which can speed healing by as much as 10%.[17] Famciclovir or valacyclovir, taken in pill form, can be effective using a single day, high-dose application and is more cost effective and convenient than the traditional treatment of lower doses for 5–7 days.[21]
Epidemiology
Herpes labialis is common throughout the world. A large survey of young adults on six continents reported that 33% of males and 28% of females had herpes labialis on two or more occasions during the year before the study. The lifetime prevalence in the United States of America is estimated at 20–45% of the adult population. Lifetime prevalence in France was reported by one study as 32% in males and 42% in females. In Germany, the prevalence was reported at 32% in people aged between 35 and 44 years, and 20% in those aged 65–74. In Jordan, another study reported a lifetime prevalence of 26%.[22]
Research
Research has gone into vaccines for both prevention and treatment of herpes infections.
References
- Opstelten W, Neven AK, Eekhof J (December 2008). "Treatment and prevention of herpes labialis". Can Fam Physician. 54 (12): 1683–1687. PMC 2602638. PMID 19074705. Archived from the original on 2010-10-28.
- "Oral Herpes – National Library of Medicine". PubMed Health. Archived from the original on 10 September 2017. Retrieved 29 May 2017.
- Rahimi H, Mara T, Costella J, Speechley M, Bohay R (May 2012). "Effectiveness of antiviral agents for the prevention of recurrent herpes labialis: a systematic review and meta-analysis". Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology. 113 (5): 618–627. doi:10.1016/j.oooo.2011.10.010. PMID 22668620.
- James, William D.; Berger, Timothy G.; et al. (2006). Andrews' Diseases of the Skin: Clinical Dermatology. Saunders Elsevier. p. 368. ISBN 978-0-7216-2921-6.
- Kennedy, PG; Rovnak, J; Badani, H; Cohrs, RJ (July 2015). "A comparison of herpes simplex virus type 1 and varicella-zoster virus latency and reactivation". The Journal of General Virology. 96 (Pt 7): 1581–1602. doi:10.1099/vir.0.000128. PMC 4635449. PMID 25794504.
- "STD Facts – Genital Herpes". www.cdc.gov. Archived from the original on 28 May 2017. Retrieved 29 May 2017.
- Buttaro, Terry Mahan (2013). Primary Care: A Collaborative Practice. Elsevier Health Sciences. p. 257. ISBN 978-0323075015. Archived from the original on 2017-09-10.
- "Cold Sores / Herpes". www.bccdc.ca. Archived from the original on 6 June 2017. Retrieved 29 May 2017.
- Stoopler, ET; Sollecito, TP (November 2014). "Oral mucosal diseases: evaluation and management". The Medical Clinics of North America. 98 (6): 1323–1352. doi:10.1016/j.mcna.2014.08.006. PMID 25443679.
- Craft, Noah; Fox, Lindy P.; Goldsmith, Lowell A.; Papier, Art; Birnbaum, Ron; Mercurio, Mary Gail (2011). VisualDx: Essential Adult Dermatology. Lippincott Williams & Wilkins. p. 349. ISBN 9781451148282. Archived from the original on 2017-09-10.
- Bruce AJ, Rogers RS (2004). "Oral manifestations of sexually transmitted diseases". Clin. Dermatol. 22 (6): 520–527. doi:10.1016/j.clindermatol.2004.07.005. PMID 15596324.
- Opstelten W, Neven AK, Eekhof J (December 2008). "Treatment and prevention of herpes labialis". Canadian Family Physician. 54 (12): 1683–7. PMC 2602638. PMID 19074705.
- Emmert DH (Mar 15, 2000). "Treatment of common cutaneous herpes simplex virus infections". American Family Physician. 61 (6): 1697–706, 1708. PMID 10750877. Archived from the original on 2013-05-26.
- Park KK, Brodell RT, Helms SE (June 2011). "Angular cheilitis, part 1: local etiologies". Cutis; Cutaneous Medicine for the Practitioner. 87 (6): 289–95. PMID 21838086.
- Scully C (2013). Oral and maxillofacial medicine : the basis of diagnosis and treatment (3rd ed.). Edinburgh: Churchill Livingstone. pp. 277–281. ISBN 9780702049484.
- "Prevalence of Herpes Simplex Virus Type 1 and Type 2 in Persons Aged 14–49: United States, 2015–2016". www.cdc.gov. July 2, 1018. Retrieved December 1, 2018.
- Harmenberg J, Oberg B, Spruance S (2010). "Prevention of ulcerative lesions by episodic treatment of recurrent herpes labialis: A literature review". Acta Derm. Venereol. 90 (2): 122–30. doi:10.2340/00015555-0806. PMID 20169294.
- "Valtrex (Valacyclovir Hydrochloride): Side Effects, Interactions, Warning, Dosage & Uses". RxList. Retrieved 2018-11-28.
- Chi, CC; Wang, SH; Delamere, FM; Wojnarowska, F; Peters, MC; Kanjirath, PP (7 August 2015). "Interventions for prevention of herpes simplex labialis (cold sores on the lips)". The Cochrane Database of Systematic Reviews. 8 (8): CD010095. doi:10.1002/14651858.CD010095.pub2. PMC 6461191. PMID 26252373.
- Treister NS, Woo SB (2010). "Topical n-docosanol for management of recurrent herpes labialis". Expert Opin Pharmacother. 11 (5): 853–60. doi:10.1517/14656561003691847. PMID 20210688. S2CID 26237384.
- Gilbert SC (2007). "Management and prevention of recurrent herpes labialis in immunocompetent patients". Herpes. 14 (3): 56–61. PMID 18371287.
- Lee C, Chi CC, Hsieh SC, Chang CJ, Delamere FM, Peters MC, Kanjirath PP, Anderson PF (2011). "Interventions for treatment of herpes simplex labialis (cold sores on the lips) (Protocol)". Cochrane Database of Systematic Reviews (10). doi:10.1002/14651858.CD009375.