Pseudoaneurysm
A pseudoaneurysm, also known as a false aneurysm, is a collection of blood that forms between the two outer layers of an artery, the tunica media and the tunica adventitia. It is usually caused by a penetrating injury to the vessel, which then bleeds, but forms a space between the above two layers, rather than exiting the vessel. It may be pulsatile and can resemble a true aneurysm. A true aneurysm involves all three layers of the blood vessel. A dissecting aneurysm is when blood from the vessel lumen tracks between the two inner layers, the intima and the tunica media. This can cause blockage of the flow. A perivascular hematoma is a collection of blood that is external to the three vessel layers. Due to being close to the vessel, it can also be pulsatile, and can be mistaken for a pseudoaneurysm or aneurysm.
| Pseudoaneurysm | |
|---|---|
| Other names | False aneurysm |
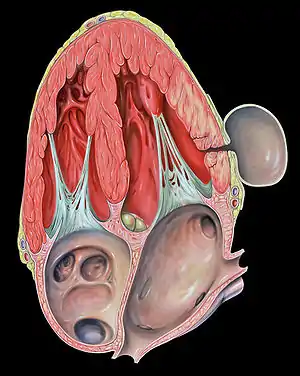 | |
| Pseudoaneurysm of the left ventricle, four-chamber echocardiography view | |
| Specialty | Cardiology |
Femoral pseudoaneurysms may complicate up to 8% of vascular interventional procedures. Small pseudoaneurysms can spontaneously clot, while others need definitive treatment.
A pseudoaneurysm may also occur in a chamber of the heart following myocardial damage due to ischemia or trauma. A pseudoaneurysm of the left ventricle is a potentially lethal complication from a myocardial infarction.
Signs and symptoms
Pseudoaneurysms usually present as a painful, tender, pulsatile mass. The overlying skin is sometimes erythematous (red). They can sometimes be confused with abscesses. The patient may describe a history of catheterization or trauma, and they may note that the pulsatile mass is gradually expanding.
Diagnosis
The diagnosis should be suspected if the patient has a history of arterial trauma. This can include arterial access for catheterization (i.e. the common femoral artery), blunt trauma (i.e. to an extremity), or penetrating trauma (i.e. gunshot or blast injury). Blunt or penetrating trauma can cause a disruption in the arterial wall, leading to a pseudoaneurysm. A patient with such a history who presents with a painful, pulsatile, tender mass at the site of catheterization or trauma should be suspected to have a pseudoaneurysm. The diagnosis should be confirmed using Duplex ultrasonography, which will reveal arterial blood flow into the pseudoaneurysm. A CT angiogram or conventional angiogram can also diagnose a pseudoaneurysm.
It is important that the diagnosis be confirmed before any procedures are performed. Incision and drainage of a suspected abscess, which is instead a pseudoaneurysm, could lead to extensive hemorrhage.
Locations

A pseudoaneurysm can form in communication with essentially any artery in the body. With the high volume of cardiac catheterizations performed today, femoral artery pseudoaneurysms, in addition to pseudoaneurysms of arteriovenous fistulas used for hemodialysis, are the most common. Pseudoaneurysms can form in the legs days, months, or even years after blunt or penetrating trauma.
Although aneurysms and left ventricular aneurysms may involve any wall segment, aneurysms in the posterolateral wall are frequently due to pseudoaneurysms. In contrast, the most common location for a true left ventricular aneurysm involves the apex of the heart.
A pseudoaneurysm can also occur in the aorta as a consequence of traumatic aortic rupture.
Outside of the heart, pseudoaneurysms associated with pancreatitis can occur in several of the abdominal vessels, including the superior mesenteric artery, pancreaticoduodenal artery, and others.
Treatment
Many options exist for the treatment of pseudoaneurysms. While surgery was the gold-standard treatment in the past, several less invasive treatment options are popular today.
Covered stent
Since the pseudoaneurysm communicates with an artery through a hole in the arterial wall, a covered stent may be placed endovascularly across this hole to "exclude it," or to prevent it from receiving blood flow from the artery. The covered stent is composed of metal and is covered with polytetrafluoroethylene (PTFE) or another sterile fabric-like material. The covered stent remains in place permanently, and the pseudoaneurysm, without a continuous flow of arterial blood, then thromboses. Advantages of this technique are that it has a high success rate without the need for an open surgery. Complications include covered stent migration, persistent leakage of blood into the pseudoaneurysm, fracturing (breaking) of the stent, and infection of the stent or of the arterial insertion site.[1][2]
Ultrasound probe compression
Another option for treatment is ultrasound probe compression of the neck of the pseudoaneurysm. The "neck" of the pseudoaneurysm is the narrow path of blood flow between the artery, through the arterial wall, and into the pseudoaneurysm cavity. The artery, neck, and pseudoaneurysm are seen on ultrasound. The ultrasound probe can be pushed firmly against the patient's skin to compress the neck of the pseudoaneurysm for usually about 20 minutes. During this time, the blood within the pseudoaneurysm clots; after the probe is then removed, the pseudoaneurysm will hopefully remain clotted and will not continue to expand. The procedure may be stopped early due to patient discomfort. It is less successful if the patient is obese, since there is more fatty tissue between the skin and the neck of the pseudoaneurysm. It also is less successful if the neck of the pseudoaneurysm is wider, since it is less likely to clot off during the period of compression. Finally, it is also much less successful if the patient is taking aspirin, warfarin (Coumadin), or another anticoagulant, since these would prevent clotting of blood within the pseudoaneurysm. Advantages are that this is the least invasive method of stopping arterial blood flow into a pseudoaneurysm.[3]
Ultrasound-guided thrombin injection
In addition to covered stent placement, another popular, minimally-invasive technique used today is ultrasound-guided thrombin injection. Thrombin (factor IIa in the coagulation cascade) is a clotting factor that converts fibrinogen into fibrin, which then polymerizes to form a blood clot. Under ultrasound guidance, thrombin can be injected directly into a pseudoaneurysm, causing it to clot. Advantages are that the technique is relatively easy to perform, is successful, and is minimally invasive. One contraindication to this procedure is if there is an arteriovenous fistula (communication between an artery and vein), in addition to the pseudoaneurysm. This occurs with about 10% of pseudoaneurysms. If this is present, thrombin injected into the pseudoaneurysm could then enter the venous circulation and possibly lead to distant thrombosis.[4]
Surgical ligation (with or without distal bypass)
Open surgery may also be performed to remove pseudoaneurysms or prevent them from expanding. If the artery is small and "expendable" - the tissues it supplies have adequate collateral blood flow - then the artery supplying the pseudoaneurysm may be ligated both proximally and distally to the pseudoaneurysm. The pseudoaneurysm may or may not be removed. If the tissues supplied by the artery do not have sufficient collateral flow (the artery is not expendable), then a vein or synthetic graft would have to be anastomosed proximally and distally to allow for continued blood flow around the pseudoaneurysm. Advantages are that the technique has been successful in the treatment of pseudoaneurysms for many years. However, it is more invasive (a large skin incision is necessary), and there is more postoperative pain and a risk for wound infection. One of the less invasive options may be preferred in a patient with many comorbidities, who is at high risk for surgery.[3]
See also
References
- Kouvelos, G. N.; Papas, N. K.; Arnaoutoglou, E. M.; Papadopoulos, G. S.; Matsag As, M. I. (2011). "Endovascular repair of profunda femoral artery false aneurysms using covered stents". Vascular. 19 (1): 51–4. doi:10.1258/vasc.2010.cr0224. PMID 21489928.
- Amato, Alexandre Campos Moraes; Kahlberg, Andrea; Bertoglio, Luca; Melissano, Germano; Chiesa, Roberto (2008). "Endovascular treatment of a triple paraanastomotic aneurysm after aortobiiliac reconstruction". Jornal Vascular Brasileiro. 7 (3): 278. doi:10.1590/S1677-54492008000300016.
- Tisi, Paul V.; Callam, Michael J. (2013-11-29). "Treatment for femoral pseudoaneurysms". The Cochrane Database of Systematic Reviews (11): CD004981. doi:10.1002/14651858.CD004981.pub4. ISSN 1469-493X. PMID 24293322.
- Malgor, R. D.; Labropoulos, N.; Gasparis, A. P.; Landau, D. S.; Tassiopoulos, A. K. (2012). "Results of a New Human Recombinant Thrombin for the Treatment of Arterial Pseudoaneurysm". Vascular and Endovascular Surgery. 46 (2): 145–9. doi:10.1177/1538574411431346. PMID 22232329.