Vein
Veins are blood vessels that carry blood towards the heart. Most veins carry deoxygenated blood from the tissues back to the heart; exceptions are the pulmonary and umbilical veins, both of which carry oxygenated blood to the heart. In contrast to veins, arteries carry blood away from the heart.
| Vein | |
|---|---|
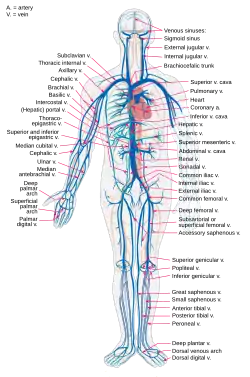 The main veins in the human body | |
.svg.png.webp) Structure of a vein, which consists of three main layers. The outer layer is connective tissue, called tunica adventitia or tunica externa; a middle layer of smooth muscle called the tunica media, and the inner layer lined with endothelial cells called the tunica intima. | |
| Details | |
| System | Circulatory system |
| Identifiers | |
| Latin | vena |
| MeSH | D014680 |
| TA98 | A12.0.00.030 A12.3.00.001 |
| TA2 | 3904 |
| FMA | 50723 |
| Anatomical terminology | |
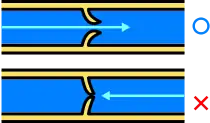
Veins are less muscular than arteries and are often closer to the skin. There are valves in most veins to prevent backflow.
Structure
Veins are present throughout the body as tubes that carry blood back to the heart. Veins are classified in a number of ways, including superficial vs. deep, pulmonary vs. systemic, and large vs. small.
- Superficial veins are those closer to the surface of the body, and have no corresponding arteries.
- Deep veins are deeper in the body and have corresponding arteries.
- Perforator veins drain from the superficial to the deep veins.[1] These are usually referred to in the lower limbs and feet.
- Communicating veins are veins that directly connect superficial veins to deep veins.
- Pulmonary veins are a set of veins that deliver oxygenated blood from the lungs to the heart.
- Systemic veins drain the tissues of the body and deliver deoxygenated blood to the heart.
Most veins are equipped with one-way valves, similar to a Duckbill valve, to prevent blood flowing in the reverse direction.
Veins are translucent, so the color a vein appears from an organism's exterior is determined in large part by the color of venous blood, which is usually dark red as a result of its low oxygen content. Veins appear blue because the of the low oxygen level in the vein. The color of a vein can be affected by the characteristics of a person's skin, how much oxygen is being carried in the blood, and how big and deep the vessels are.[2] When a vein is drained of blood and removed from an organism, it appears grey-white.
Venous system
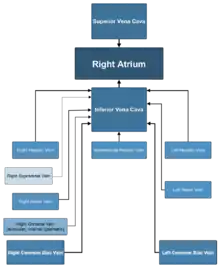
The largest veins in the human body are the venae cavae. These are two large veins which enter the right atrium of the heart from above and below. The superior vena cava carries blood from the arms and head to the right atrium of the heart, while the inferior vena cava carries blood from the legs and abdomen to the heart. The inferior vena cava is retroperitoneal and runs to the right and roughly parallel to the abdominal aorta along the spine. Large veins feed into these two veins, and smaller veins into these. Together this forms the venous system.
Whilst the main veins hold a relatively constant position, the position of veins person to person can display quite a lot of variation.
The pulmonary veins carry relatively oxygenated blood from the lungs to the heart. The superior and inferior venae cavae carry relatively deoxygenated blood from the upper and lower systemic circulations, respectively.
The portal venous system is a series of veins or venules that directly connect two capillary beds. Examples of such systems include the hepatic portal vein and hypophyseal portal system.
The peripheral veins carry blood from the limbs and hands and feet.
Microanatomy
Microscopically, veins have a thick outer layer made of connective tissue, called the tunica externa or tunica adventitia. During procedures requiring venous access such as venipuncture, one may notice a subtle "pop" as the needle penetrates this layer. The middle layer of bands of smooth muscle are called tunica media and are, in general, much thinner than those of arteries, as veins do not function primarily in a contractile manner and are not subject to the high pressures of systole, as arteries are. The interior is lined with endothelial cells called tunica intima. The precise location of veins varies much more from person to person than that of arteries.[3]
Function
Veins serve to return blood from organs to the heart. Veins are also called "capacitance vessels" because most of the blood volume (60%) is contained within veins. In systemic circulation oxygenated blood is pumped by the left ventricle through the arteries to the muscles and organs of the body, where its nutrients and gases are exchanged at capillaries. After taking up cellular waste and carbon dioxide in capillaries, blood is channeled through vessels that converge with one another to form venules, which continue to converge and form the larger veins. The de-oxygenated blood is taken by veins to the right atrium of the heart, which transfers the blood to the right ventricle, where it is then pumped through the pulmonary arteries to the lungs. In pulmonary circulation the pulmonary veins return oxygenated blood from the lungs to the left atrium, which empties into the left ventricle, completing the cycle of blood circulation.
The return of blood to the heart is assisted by the action of the muscle pump, and by the thoracic pump action of breathing during respiration. Standing or sitting for a prolonged period of time can cause low venous return from venous pooling (vascular) shock. Fainting can occur but usually baroreceptors within the aortic sinuses initiate a baroreflex such that angiotensin II and norepinephrine stimulate vasoconstriction and heart rate increases to return blood flow. Neurogenic and hypovolaemic shock can also cause fainting. In these cases, the smooth muscles surrounding the veins become slack and the veins fill with the majority of the blood in the body, keeping blood away from the brain and causing unconsciousness. Jet pilots wear pressurized suits to help maintain their venous return and blood pressure.
The arteries are perceived as carrying oxygenated blood to the tissues, while veins carry deoxygenated blood back to the heart. This is true of the systemic circulation, by far the larger of the two circuits of blood in the body, which transports oxygen from the heart to the tissues of the body. However, in pulmonary circulation, the arteries carry deoxygenated blood from the heart to the lungs, and veins return blood from the lungs to the heart. The difference between veins and arteries is their direction of flow (out of the heart by arteries, returning to the heart for veins), not their oxygen content. In addition, deoxygenated blood that is carried from the tissues back to the heart for reoxygenation in the systemic circulation still carries some oxygen, though it is considerably less than that carried by the systemic arteries or pulmonary veins.
Although most veins take blood back to the heart, there is an exception. Portal veins carry blood between capillary beds. For example, the hepatic portal vein takes blood from the capillary beds in the digestive tract and transports it to the capillary beds in the liver. The blood is then drained in the gastrointestinal tract and spleen, where it is taken up by the hepatic veins, and blood is taken back into the heart. Since this is an important function in mammals, damage to the hepatic portal vein can be dangerous. Blood clotting in the hepatic portal vein can cause portal hypertension, which results in a decrease of blood fluid to the liver.
Cardiac veins
The vessels that remove the deoxygenated blood from the heart muscle are known as cardiac veins. These include the great cardiac vein, the middle cardiac vein, the small cardiac vein, the smallest cardiac veins, and the anterior cardiac veins. Coronary veins carry blood with a poor level of oxygen, from the myocardium to the right atrium. Most of the blood of the coronary veins returns through the coronary sinus. The anatomy of the veins of the heart is very variable, but generally it is formed by the following veins: heart veins that go into the coronary sinus: the great cardiac vein, the middle cardiac vein, the small cardiac vein, the posterior vein of the left ventricle, and the vein of Marshall. Heart veins that go directly to the right atrium: the anterior cardiac veins, the smallest cardiac veins (Thebesian veins).[4]
Clinical significance
Venous insufficiency
Venous insufficiency is the most common disorder of the venous system, and is usually manifested as spider veins or varicose veins. Several varieties of treatments are used, depending on the patient's particular type and pattern of veins and on the physician's preferences. Treatment can include Endovenous Thermal Ablation using radiofrequency or laser energy, vein stripping, ambulatory phlebectomy, foam sclerotherapy, lasers, or compression.
Postphlebitic syndrome is venous insufficiency that develops following deep vein thrombosis.[5]
Deep vein thrombosis
Deep vein thrombosis is a condition in which a blood clot forms in a deep vein. This is usually the veins of the legs, although it can also occur in the veins of the arms. Immobility, active cancer, obesity, traumatic damage and congenital disorders that make clots more likely are all risk factors for deep vein thrombosis. It can cause the affected limb to swell, and cause pain and an overlying skin rash. In the worst case, a deep vein thrombosis can extend, or a part of a clot can break off and land in the lungs, called pulmonary embolism.
The decision to treat deep vein thrombosis depends on its size, a person's symptoms, and their risk factors. It generally involves anticoagulation to prevents clots or to reduce the size of the clot.
Portal hypertension
The portal veins are found within the abdomen and carry blood through to the liver. Portal hypertension is associated with cirrhosis or disease of the liver, or other conditions such as an obstructing clot (Budd Chiari syndrome) or compression from tumours or tuberculosis lesions. When the pressure increases in the portal veins, a collateral circulation develops, causing visible veins such as oesophageal varices.
Other
Thrombophlebitis is an inflammatory condition of the veins related to blood clots.
Imaging
Ultrasound, particularly duplex ultrasound, is a common way that veins can be seen.
Veins of clinical significance
The Batson Venous plexus, or simply Batson's Plexus, runs through the inner vertebral column connecting the thoracic and pelvic veins. These veins get their notoriety from the fact that they are valveless, which is believed to be the reason for metastasis of certain cancers.
The great saphenous vein is the most important superficial vein of the lower limb. First described by the Persian physician Avicenna, this vein derives its name from the word safina, meaning "hidden". This vein is "hidden" in its own fascial compartment in the thigh and exits the fascia only near the knee. Incompetence of this vein is an important cause of varicose veins of lower limbs.
The Thebesian veins within the myocardium of the heart are valveless veins that drain directly into the chambers of the heart. The coronary veins all empty into the coronary sinus which empties into the right atrium.
The dural venous sinuses within the dura mater surrounding the brain receive blood from the brain and also are a point of entry of cerebrospinal fluid from arachnoid villi absorption. Blood eventually enters the internal jugular vein.
Phlebology
| Look up phlebology in Wiktionary, the free dictionary. |
Phlebology is the medical specialty devoted to the diagnosis and treatment of venous disorders. A medical specialist in phlebology is termed a phlebologist. A related image is called a phlebograph.
The American Medical Association added phlebology to their list of self-designated practice specialties in 2005. In 2007 the American Board of Phlebology (ABPh), subsequently known as the American Board of Venous & Lymphatic Medicine (ABVLM), was established to improve the standards of phlebologists and the quality of their patient care by establishing a certification examination, as well as requiring maintenance of certification. Although As of 2017 not a Member Board of the American Board of Medical Specialties (ABMS), the American Board of Venous & Lymphatic Medicine uses a certification exam based on ABMS standards.
The American Vein and Lymphatic Society (AVLS), formerly the American College of Phlebology (ACP) one of the largest medical societies in the world for physicians and allied health professionals working in the field of phlebology, has 2000 members. The AVLS encourages education and training to improve the standards of medical practitioners and the quality of patient care.
The American Venous Forum (AVF) is a medical society for physicians and allied health professionals dedicated to improving the care of patients with venous and lymphatic disease. The majority of its members manage the entire spectrum of venous and lymphatic diseases – from varicose veins to congenital abnormalities to deep vein thrombosis to chronic venous diseases. Founded in 1987, the AVF encourages research, clinical innovation, hands-on education, data collection and patient outreach.
History
The earliest known writings on the circulatory system are found in the Ebers Papyrus (16th century BCE), an ancient Egyptian medical papyrus containing over 700 prescriptions and remedies, both physical and spiritual. In the papyrus, it acknowledges the connection of the heart to the arteries. The Egyptians thought air came in through the mouth and into the lungs and heart. From the heart, the air travelled to every member through the arteries. Although this concept of the circulatory system is only partially correct, it represents one of the earliest accounts of scientific thought.
In the 6th century BCE, the knowledge of circulation of vital fluids through the body was known to the Ayurvedic physician Sushruta in ancient India.[6] He also seems to have possessed knowledge of the arteries, described as 'channels' by Dwivedi & Dwivedi (2007).[6] The valves of the heart were discovered by a physician of the Hippocratean school around the 4th century BCE. However their function was not properly understood then. Because blood pools in the veins after death, arteries look empty. Ancient anatomists assumed they were filled with air and that they were for transport of air.
The Greek physician Herophilus distinguished veins from arteries but thought that the pulse was a property of arteries themselves. Greek anatomist Erasistratus observed that arteries that were cut during life bleed. He ascribed the fact to the phenomenon that air escaping from an artery is replaced with blood that entered by very small vessels between veins and arteries. Thus he apparently postulated capillaries but with reversed flow of blood.[7]
In 2nd century AD Rome, the Greek physician Galen knew that blood vessels carried blood and identified venous (dark red) and arterial (brighter and thinner) blood, each with distinct and separate functions. Growth and energy were derived from venous blood created in the liver from chyle, while arterial blood gave vitality by containing pneuma (air) and originated in the heart. Blood flowed from both creating organs to all parts of the body where it was consumed and there was no return of blood to the heart or liver. The heart did not pump blood around, the heart's motion sucked blood in during diastole and the blood moved by the pulsation of the arteries themselves.
Galen believed that the arterial blood was created by venous blood passing from the left ventricle to the right by passing through 'pores' in the interventricular septum, air passed from the lungs via the pulmonary artery to the left side of the heart. As the arterial blood was created 'sooty' vapors were created and passed to the lungs also via the pulmonary artery to be exhaled.
In 1025, The Canon of Medicine by the Persian physician Avicenna "erroneously accepted the Greek notion regarding the existence of a hole in the ventricular septum by which the blood traveled between the ventricles." While also refining Galen's erroneous theory of the pulse, Avicenna provided the first correct explanation of pulsation: "Every beat of the pulse comprises two movements and two pauses. Thus, expansion : pause : contraction : pause. [...] The pulse is a movement in the heart and arteries ... which takes the form of alternate expansion and contraction."[8]
In 1242, the Arabian physician Ibn al-Nafis became the first person to accurately describe the process of pulmonary circulation,[9] for which he has been described as the Arab Father of Circulation.[10] Ibn al-Nafis stated in his Commentary on Anatomy in Avicenna's Canon:
"...the blood from the right chamber of the heart must arrive at the left chamber but there is no direct pathway between them. The thick septum of the heart is not perforated and does not have visible pores as some people thought or invisible pores as Galen thought. The blood from the right chamber must flow through the vena arteriosa (pulmonary artery) to the lungs, spread through its substances, be mingled there with air, pass through the arteria venosa (pulmonary vein) to reach the left chamber of the heart and there form the vital spirit..."
In addition, Ibn al-Nafis had an insight into what would become a larger theory of the capillary circulation. He stated that "there must be small communications or pores (manafidh in Arabic) between the pulmonary artery and vein," a prediction that preceded the discovery of the capillary system by more than 400 years.[11] Ibn al-Nafis' theory, however, was confined to blood transit in the lungs and did not extend to the entire body.
Michael Servetus was the first European to describe the function of pulmonary circulation, although his achievement was not widely recognized at the time, for a few reasons. He firstly described it in the "Manuscript of Paris"[12][13] (near 1546), but this work was never published. And later he published this description, but in a theological treatise, Christianismi Restitutio, not in a book on medicine. Only three copies of the book survived but these remained hidden for decades, the rest were burned shortly after its publication in 1553 because of persecution of Servetus by religious authorities.
Better known discovery of pulmonary circulation was by Vesalius's successor at Padua, Realdo Colombo, in 1559.
_Venenbild.jpg.webp)
Finally, William Harvey, a pupil of Hieronymus Fabricius (who had earlier described the valves of the veins without recognizing their function), performed a sequence of experiments, and published Exercitatio Anatomica de Motu Cordis et Sanguinis in Animalibus in 1628, which "demonstrated that there had to be a direct connection between the venous and arterial systems throughout the body, and not just the lungs. Most importantly, he argued that the beat of the heart produced a continuous circulation of blood through minute connections at the extremities of the body. This is a conceptual leap that was quite different from Ibn al-Nafis' refinement of the anatomy and bloodflow in the heart and lungs."[14] This work, with its essentially correct exposition, slowly convinced the medical world. However, Harvey was not able to identify the capillary system connecting arteries and veins; these were later discovered by Marcello Malpighi in 1661.
In 1956, André Frédéric Cournand, Werner Forssmann and Dickinson W. Richards were awarded the Nobel Prize in Medicine "for their discoveries concerning heart catheterization and pathological changes in the circulatory system."[15] In his Nobel lecture, Forssmann credits Harvey as birthing cardiology with the publication of his book in 1628.[16]
In the 1970s, Diana McSherry developed computer-based systems to create images of the circulatory system and heart without the need for surgery.[17]
References
- Albert, consultants Daniel (2012). Dorland's illustrated medical dictionary (32nd ed.). Philadelphia, PA: Saunders/Elsevier. p. 2042. ISBN 978-1-4160-6257-8.
- Kienle, Alwin; Lilge, Lothar; Vitkin, I. Alex; Patterson, Michael S.; Wilson, Brian C.; Hibst, Raimund; Steiner, Rudolf (1 March 1996). "Why do veins appear blue? A new look at an old question". Applied Optics. 35 (7): 1151. Bibcode:1996ApOpt..35.1151K. doi:10.1364/AO.35.001151. PMID 21085227.
- Maton, Anthea; Jean Hopkins; Charles William McLaughlin; Alexandra Senckowski; Susan Johnson; Maryanna Quon Warner; David LaHart; Jill D. Wright (1993). Human Biology and Health. Englewood Cliffs, New Jersey: Prentice Hall. ISBN 978-0-13-981176-0.
- Adams, Matt; Morgan, Matt A.; et al. "Coronary veins". Radiopaedia.org.
- Kahn SR (August 2006). "The post-thrombotic syndrome: progress and pitfalls". British Journal of Haematology. 134 (4): 357–65. doi:10.1111/j.1365-2141.2006.06200.x. PMID 16822286. S2CID 19715556.
- Dwivedi, Girish & Dwivedi, Shridhar (2007). "History of Medicine: Sushruta – the Clinician – Teacher par Excellence" Archived October 10, 2008, at the Wayback Machine, Indian J Chest Dis Allied Sci Vol.49 pp.243-4, National Informatics Centre (Government of India).
- Anatomy – History of anatomy. Scienceclarified.com. Retrieved 2013-09-15.
- Hajar, Rachel (1999). "The Greco-Islamic Pulse". Heart Views. 1 (4): 136–140 [138]. Archived from the original on 9 January 2014.
- Loukas, M; Lam, R; Tubbs, RS; Shoja, MM; Apaydin, N (May 2008). "Ibn al-Nafis (1210-1288): the first description of the pulmonary circulation". The American Surgeon. 74 (5): 440–2. doi:10.1177/000313480807400517. PMID 18481505. S2CID 44410468.
- Reflections, Chairman's (2004). "Traditional Medicine Among Gulf Arabs, Part II: Blood-letting". Heart Views. 5 (2): 74–85 [80]. Archived from the original on 11 September 2007.
- West, J. B. (2008). "Ibn al-Nafis, the pulmonary circulation, and the Islamic Golden Age". Journal of Applied Physiology. 105 (6): 1877–1880. doi:10.1152/japplphysiol.91171.2008. PMC 2612469. PMID 18845773.
- Gonzalez Etxeberria, Patxi (2011) Amor a la verdad, el – vida y obra de Miguel servet [The love for truth. Life and work of Michael Servetus]. Navarro y Navarro, Zaragoza, collaboration with the Government of Navarra, Department of Institutional Relations and Education of the Government of Navarra. ISBN 8423532666 pp. 215–228 & 62nd illustration (XLVII)
- Michael Servetus Research Study with graphical proof on the Manuscript of Paris and many other manuscripts and new works by Servetus
- Pormann, Peter E. and Smith, E. Savage (2007) Medieval Islamic medicine Georgetown University, Washington DC, p. 48, ISBN 1589011619.
- "The Nobel Prize in Physiology or Medicine 1956". Nobel Foundation. Retrieved 28 July 2007.
- "The Role of Heart Catheterization and Angiocardiography in the Development of Modern Medicine". Retrieved 8 October 2017.
- Wayne, Tiffany K. (2011). American women of science since 1900. Santa Barbara, Calif.: ABC-CLIO. pp. 677–678. ISBN 9781598841589.
Further reading
- Shoja, M. M.; Tubbs, R. S.; Loukas, M.; Khalili, M.; Alakbarli, F.; Cohen-Gadol, A. A. (2009). "Vasovagal syncope in the Canon of Avicenna: The first mention of carotid artery hypersensitivity". International Journal of Cardiology. 134 (3): 297–301. doi:10.1016/j.ijcard.2009.02.035. PMID 19332359.
External links
| Look up vein in Wiktionary, the free dictionary. |
- Merck Manual article on veins
- A lecture on YouTube on the veins' and lymphatic systems of the upper limb