Right bundle branch block
A right bundle branch block (RBBB) is a heart block in the right bundle branch of the electrical conduction system.[1]
| Right bundle branch block | |
|---|---|
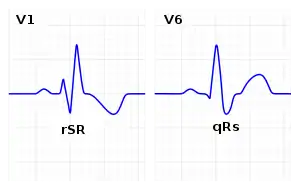 | |
| ECG characteristics of a typical RBBB showing wide QRS complexes with a terminal R wave in lead V1 and a prolonged S wave in lead V6. | |
| Specialty | Cardiology |
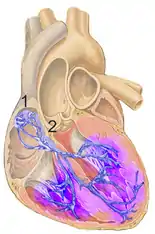
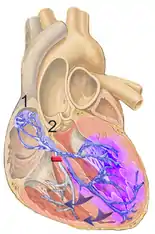
During a right bundle branch block, the right ventricle is not directly activated by impulses travelling through the right bundle branch. The left ventricle however, is still normally activated by the left bundle branch. These impulses are then able to travel through the myocardium of the left ventricle to the right ventricle and depolarize the right ventricle this way. As conduction through the myocardium is slower than conduction through the Bundle of His-Purkinje fibres, the QRS complex is seen to be widened. The QRS complex often shows an extra deflection that reflects the rapid depolarisation of the left ventricle followed by the slower depolarisation of the right ventricle.
Causes
Common causes are Normal variant, Right ventricular hypertrophy or strain, Congenital heart disease such as atrial septal defect and Ischemic heart disease. [2] In addition, a right bundle branch block may also result from Brugada syndrome, pulmonary embolism, rheumatic heart disease, myocarditis, cardiomyopathy, or hypertension.
Diagnosis
The criteria to diagnose a right bundle branch block on the electrocardiogram:
- The heart rhythm must originate above the ventricles (i.e., sinoatrial node, atria or atrioventricular node) to activate the conduction system at the correct point.
- The QRS duration must be more than 100 ms (incomplete block) or more than 120 ms (complete block).[3]
- There should be a terminal R wave in lead V1 (often called "R prime," and denoted by R, rR', rsR', rSR', or qR).
- There must be a prolonged S wave in leads I and V6 (sometimes referred to as a "slurred" S wave).
The T wave should be deflected opposite the terminal deflection of the QRS complex. This is known as appropriate T wave discordance with bundle branch block. A concordant T wave may suggest ischemia or myocardial infarction.
 RBBB with associated first degree AV block
RBBB with associated first degree AV block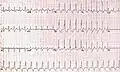 RBBB with associated tachycardia
RBBB with associated tachycardia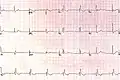 RBBB
RBBB
Treatment
The underlying condition may be treated by medications to control hypertension or diabetes, if they are the primary underlying cause. If coronary arteries are blocked, an invasive coronary angioplasty may relieve the impending RBBB.[4]
Epidemiology
Prevalence of RBBB increases with age.
References
- "Conduction Blocks 2006 KCUMB". Retrieved 2009-01-20.
- Goldman, Lee (2011). Goldman's Cecil Medicine (24th ed.). Philadelphia: Elsevier Saunders. pp. 400–401. ISBN 978-1437727883.
- "Lesson VI - ECG Conduction Abnormalities". Retrieved 2009-01-07.
- "Right Bundle Branch Block". www.symptoma.com. Retrieved 2015-08-13.
External links
| Classification | |
|---|---|
| External resources |
