Torsades de pointes
Torsades de pointes, torsade de pointes or torsades des pointes (TdP) (French: [tɔʁsad də pwɑ̃t], translated as "twisting of peaks") is a specific type of abnormal heart rhythm that can lead to sudden cardiac death. It is a polymorphic ventricular tachycardia that exhibits distinct characteristics on the electrocardiogram (ECG). It was described by French physician François Dessertenne in 1966.[1] Prolongation of the QT interval can increase a person's risk of developing this abnormal heart rhythm.
| Torsades de pointes | |
|---|---|
| Other names | Torsade(s) |
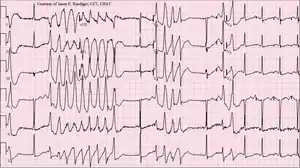 | |
| 12-lead ECG of torsades de pointes (TdP) in a 56-year-old white female with low blood potassium (2.4 mmol/L) and low blood magnesium (1.6 mg/dL) | |
| Specialty | Cardiology |
Signs and symptoms
Most episodes will revert spontaneously to a normal sinus rhythm.[2] Symptoms and consequences include palpitations, dizziness, lightheadedness (during shorter episodes), fainting (during longer episodes), and sudden cardiac death.
Causes
Torsades occurs as both an inherited (linked to at least 17 genes)[3] and as an acquired form caused most often by drugs and/or electrolyte disorders that cause excessive lengthening of the QT interval.[4]
Common causes for torsades de pointes include drug-induced QT prolongation and less often diarrhea, low serum magnesium, and low serum potassium or congenital long QT syndrome. It can be seen in malnourished individuals and chronic alcoholics, due to a deficiency in potassium and/or magnesium. Certain drugs and combinations of drugs resulting in drug interactions are common contributors to torsades de pointes risk. QT-prolonging medications such as clarithromycin, levofloxacin, or haloperidol, when taken concurrently with cytochrome P450 inhibitors, such as fluoxetine, cimetidine, or particular foods including grapefruit, can result in higher-than-normal levels of medications that prolong the QT interval in the bloodstream and therefore increase a person's risk of developing torsades de pointes. At least one mention of the common over-the-counter medication loperamide causing TdP has been made in the literature, although the dose preceding this particular cardiac event was well beyond the therapeutic range of the medication.[5] In addition, patients with inherited long QT syndrome have a very high risk of episodes of TdP and that risk can be further increased by drugs and electrolyte disorders that further prolong QT.
Medications as causes
Knowledge that TdP may occur in patients taking certain prescription drugs has been both a major liability and reason for removal of 14 medications from the marketplace.[6] Forty nine drugs known to cause TdP and another 170 that are known to prolong QTc remain on the market because the drugs provide medical benefit and the risk of TdP can be managed and mitigated by instructions in the drug label.[7][8] Examples of compounds linked to clinical observations of TdP include amiodarone, most fluoroquinolones, methadone, lithium, chloroquine, erythromycin, azithromycin, pimozide, and phenothiazines.[9] The anti-emetic agent ondansetron may also increase the risk of developing TdP.[10] It has also been shown as a side effect of certain anti-arrhythmic medications, such as sotalol, procainamide, quinidine, ibutilide, and dofetilide[11] In one example, the gastrokinetic drug cisapride (Propulsid) was withdrawn from the US market in 2000 after it was linked to deaths caused by long QT syndrome-induced torsades de pointes. This effect can be directly linked to QT prolongation mediated predominantly by inhibition of the hERG channel and, in some cases, augmentation of the late sodium channel.[12]
Risk factors

The following is a partial list of factors associated with an increased tendency towards developing torsades de pointes:[13]
- Medications
- Hypokalemia (low serum potassium)
- Hypomagnesemia (low serum magnesium)
- Hypocalcemia (low serum calcium)
- Bradycardia (slow heartbeat)
- Heart failure
- Left ventricular hypertrophy
- Hypothermia
- Subarachnoid hemorrhage
- Hypothyroidism
Pathophysiology
Action potential of cardiac muscles can be broken down into five phases:
- Phase 0: Sodium channels open, resulting in the entrance of Na+ into the cells; this results in the depolarization of the cardiac muscles.
- Phase 1: Sodium channels close; this stops depolarization. Potassium channels open, leading to an outward current of K+ out of the cells.
- Phase 2: Potassium channels remain open (outward current of K+), and calcium channels now also open (inward current of Ca++), resulting in a plateau state.
- Phase 3: Calcium channels close (inward Ca++ stops), but potassium channels are still open (outward K+ current); this persists until the cells gain back normal polarization (repolarization achieved). Please note that phase 0 leads to a net gain of Na+, while phases 1-3 lead to a net loss of K+. This imbalance is corrected by the Na+/K+-ATPase channel that pumps K+ into the cell and sodium out of the cell; this does not change polarization of the cells, but does restore ionic content to its initial state.
- Phase 4: Exciting triggers (e.g. sinus node) will cause minor depolarization in the cells; this will result in increasing permeability of sodium channels, which trigger the opening of sodium channels.
Repolarization of the cardiomyocytes occurs in phases 1-3, and is caused predominantly by the outward movement of potassium ions. In Torsades de pointes, however, the repolarization is prolonged; this can be due to electrolyte disturbances (hypokalemia, hypomagnesemia, hypocalcemia), bradycardia, certain drugs (disopyramide, sotalol, amiodarone, amitriptyline, chlorpromazine, erythromycin) and/or congenital syndromes.[14]
The prolongation of repolarisation may result in subsequent activation of an inward depolarisation current, known as an early after-depolarisation, which may promote triggered activity.[15] Re-entry, due to a dispersion of refractory periods, is also possible;[16] this is because M Cells (found in the mid myocardial layer) show a more prolonged repolarization phase in response to potassium blockage than other cells. In turn, this produces a zone of functional refractoriness (inability to depolarize) in the mid myocardial layer.[15] When new action potential is generated, the mid myocardial layer will remain in a refractory period, but the surrounding tissue will depolarize. As soon as the mid myocardial layer is no longer in a refractory period, excitation from nearby tissue will cause a retrograde current and a reentry circuit that will result in a positive chronotropic cycle, leading to tachycardia.
Diagnosis
The ECG tracing in torsades demonstrates a polymorphic ventricular tachycardia with a characteristic illusion of a twisting of the QRS complex around the isoelectric baseline (peaks, which are at first pointing up, appear to be pointing down for subsequent "beats" when looking at ECG traces of the "heartbeat"). It is hemodynamically unstable and causes a sudden drop in arterial blood pressure, leading to dizziness and fainting. Depending on their cause, most individual episodes of torsades de pointes revert to normal sinus rhythm within a few seconds; however, episodes may also persist and possibly degenerate into ventricular fibrillation, leading to sudden death in the absence of prompt medical intervention. Torsades de pointes is associated with long QT syndrome, a condition whereby prolonged QT intervals are visible on an ECG. Long QT intervals predispose the patient to an R-on-T phenomenon, wherein the R-wave, representing ventricular depolarization, occurs during the relative refractory period at the end of repolarization (represented by the latter half of the T-wave). An R-on-T can initiate torsades. Sometimes, pathologic T-U waves may be seen in the ECG before the initiation of torsades.[17]
A "short-coupled variant of torsade de pointes", which presents without long QT syndrome, was also described in 1994 as having the following characteristics:[18]
- Drastic rotation of the heart's electrical axis
- Prolonged QT interval (LQTS) - may not be present in the short-coupled variant of torsade de pointes
- Preceded by long and short RR-intervals - not present in the short-coupled variant of torsade de pointes
- Triggered by a premature ventricular contraction (R-on-T PVC)
Treatment
The treatment of torsades de pointes aims to restore a normal rhythm and to prevent the arrhythmia recurring. While torsades may spontaneously revert to a normal sinus rhythm, sustained torsades requires emergency treatment to prevent cardiac arrest.[19] The most effective treatment to terminate torsades is an electrical cardioversion - a procedure in which an electrical current is applied across the heart to temporarily stop and then resynchronise the heart's cells.[19] Treatment to prevent recurrent torsades includes infusion of magnesium sulphate,[20] correction of electrolyte imbalances such as low blood potassium levels (hypokalaemia), and withdrawal of any medications that prolong the QT interval. Treatments used to prevent torsades in specific circumstances include beta blockers or mexiletine in long QT syndrome.[21] Occasionally a pacemaker may be used to accelerate the heart's own sinus rhythm, and those at risk of further torsades may be offered an implantable defibrillator to automatically detect and defibrillate further episodes of the arrhythmia.[21]
History
The phenomenon was originally described in a French medical journal by Dessertenne in 1966, when he observed this cardiac rhythm disorder in an 80-year-old female patient with complete intermittent atrioventricular block. In coining the term, he referred his colleagues to the "Dictionnaire Le Robert", a bilingual French English dictionary, of which his wife had just given him a copy. Here, "torsade" is defined as:
- a bundle of threads, twisted in a helix or spiral, for ornamental purposes (such as in an Aran sweater);
- long hair twisted together;
- an ornamental motif, as seen on architectural columns.
Terminology
The singular and plural forms (torsade de pointes, torsades de pointes and torsades des pointes) have all often been used. The question of whether each one is grammatically "correct" and the others "incorrect" has repeatedly arisen. This is seen among major medical dictionaries, where one enters only the plural form, another enters the plural form as the headword but lists the singular as a variant, and yet another enters the singular form as the headword and gives a usage comment saying that the plural is not preferred. One group of physicians has suggested[22] that it would make the most sense to use the singular form to refer to the arrhythmia entity (where an arrhythmia may involve one or multiple episodes), and that one might best reserve the plural form for describing repeated twisting during a single episode. Other authors have suggested all three words should be plural.[23] Regarding the natural language variation, they concluded, in good nature, "Wasn't it the French who coined the term vive la difference?"[22]
References
- Dessertenne, F. (1966). Prepared by Rahel Farhad. "La tachycardie ventriculaire a deux foyers opposes variables". Archives des maladies du coeur et des vaisseaux (in French). 59 (2): 263–272. ISSN 0003-9683. PMID 4956181.
- Groot, Jan Albert Nicolaas; Ten Bokum, Leonore; Van Den Oever, Hubertus Laurentius Antonius (2018). "Late presentation of Torsades de Pointes related to fluoxetine following a multiple drug overdose". Journal of Intensive Care. 6: 59. doi:10.1186/s40560-018-0329-1. PMC 6131849. PMID 30214811.
- Saprungruang, Ankavipar; Khongphatthanayothin, Apichai; Mauleekoonphairoj, John; Wandee, Pharawee; Kanjanauthai, Supaluck; Bhuiyan, Zahurul A.; Wilde, Arthur A. M.; Poovorawan, Yong (2018). "Genotype and clinical characteristics of congenital long QT syndrome in Thailand". Indian Pacing and Electrophysiology Journal. 18 (5): 165–171. doi:10.1016/j.ipej.2018.07.007. PMC 6198685. PMID 30036649.
- Schwartz, Peter J.; Woosley, Raymond L. (2016). "Predicting the Unpredictable". Journal of the American College of Cardiology. 67 (13): 1639–1650. doi:10.1016/j.jacc.2015.12.063. PMID 27150690.
- Loperamide Induced Torsades de Pointes: A Case Report and Review of the Literature
- Drew, B. J., Ackerman, M. J., Funk, M., et al. Prevention of Torsade de Pointes in Hospital Settings: A Scientific Statement From the American Heart Association and the American College of Cardiology Foundation. Journal of the American College of Cardiology (2010) 55.9:934–947.
- Woosley, R. L., Heise, C. W., Gallo, T., Tate, J., Woosley, D., and K. A. Romero. www.CredibleMeds.org, QTdrugs List, Accessed 9 June 2019, AZCERT, Inc. 1822 Innovation Park Dr., Oro Valley, AZ 85755.
- Prediction of the Risk of Torsade de Pointes Using the Model of Isolated Canine Purkinje Fibres. British Journal of Pharmacology (2005) 144.3:376–385.
- Champeroux, P., Viaud, K., El Amrani, A. I., et al. Prediction of the Risk of Torsade de Pointes Using the Model of Isolated Canine Purkinje Fibres. British Journal of Pharmacology (2005) 144.3:376–385.
- Vallerand, April Hazard (2014-06-05). Davis's drug guide for nurses. Sanoski, Cynthia A.,, Deglin, Judith Hopfer, 1950- (Fourteenth ed.). Philadelphia. ISBN 978-0-8036-4085-6. OCLC 881473728.
- Lenz T. L.; Hilleman D. E. (July 2000). "Dofetilide, a New Class III Antiarrhythmic Agent". Pharmacotherapy. 20 (7): 776–86. doi:10.1592/phco.20.9.776.35208. PMID 10907968. S2CID 19897963.
- Yang, T., Chun, Y. W., Stroud, D. M., et al. Screening for Acute IKr Block is Insufficient to Detect Torsades de Pointes Liability: Role of Late Sodium Current. Circulation (2014) 130:224–234.
- Clinical Factors Associated with Prolonged QTc and/or TdP, CredibleMeds.org, accessed 8 June 2019.
- Davidson, Sir Stanley (2010). Colledge, Nicki; Walker, Brian; Ralston, Stuart (eds.). Davidson's Principles and Practice of Medicine (21st ed.). United Kingdom: Elsevier. p. 568. ISBN 978-0-7020-3084-0.
- Yap, Yee Guan; Camm, A John (2017-01-17). "Drug induced QT prolongation and torsades de pointes". Heart. 89 (11): 1363–1372. doi:10.1136/heart.89.11.1363. ISSN 1355-6037. PMC 1767957. PMID 14594906.
- Napolitano, C.; Priori, S. G.; Schwartz, P. J. (1994-01-01). "Torsade de pointes. Mechanisms and management". Drugs. 47 (1): 51–65. doi:10.2165/00003495-199447010-00004. ISSN 0012-6667. PMID 7510621. S2CID 1153199.
- John, J.; Amley, X.; Bombino, G.; Gitelis, C.; Topi, B.; Hollander, G.; Ghosh, J. (2010). "Torsade de Pointes due to Methadone Use in a Patient with HIV and Hepatitis C Coinfection". Cardiology Research and Practice. 2010: 1–4. doi:10.4061/2010/524764. PMC 3021856. PMID 21253542.
- Leenhardt A, Glaser E, Burguera M, Nürnberg M, Maison-Blanche P, Coumel P (January 1994). "Short-coupled variant of torsade de pointes. A new electrocardiographic entity in the spectrum of idiopathic ventricular tachyarrhythmias". Circulation. 89 (1): 206–15. doi:10.1161/01.CIR.89.1.206. PMID 8281648.
- Thomas, Simon H. L.; Behr, Elijah R. (March 2016). "Pharmacological treatment of acquired QT prolongation and torsades de pointes". British Journal of Clinical Pharmacology. 81 (3): 420–427. doi:10.1111/bcp.12726. ISSN 1365-2125. PMC 4767204. PMID 26183037.
- Hoshino, Kenji; Ogawa, Kiyoshi; Hishitani, Takashi; Isobe, Takeshi; Etoh, Yoshikatsu (2006). "Successful uses of magnesium sulfate for torsades de pointes in children with long QT syndrome". Pediatrics International. 48 (2): 112–117. doi:10.1111/j.1442-200X.2006.02177.x. PMID 16635167. S2CID 24904388.
- Priori, Silvia G.; Blomström-Lundqvist, Carina; Mazzanti, Andrea; Blom, Nico; Borggrefe, Martin; Camm, John; Elliott, Perry Mark; Fitzsimons, Donna; Hatala, Robert; Hindricks, Gerhard; Kirchhof, Paulus (November 2015). "2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC)Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC)". Europace: European Pacing, Arrhythmias, and Cardiac Electrophysiology: Journal of the Working Groups on Cardiac Pacing, Arrhythmias, and Cardiac Cellular Electrophysiology of the European Society of Cardiology. 17 (11): 1601–1687. doi:10.1093/europace/euv319. ISSN 1532-2092. PMID 26318695.
- Moise NS (1999), "As Americans, we should get this right [correspondence and response]", Circulation, 100 (13): 1462, doi:10.1161/01.CIR.100.13.1462, PMID 10500317.
- Mullins ME (2011), "Mon bête noir (my pet peeve)", Journal of Medical Toxicology, 7 (2): 181, doi:10.1007/s13181-011-0153-7, PMC 3724434, PMID 21461788
| Classification | |
|---|---|
| External resources |