Acid–base homeostasis
Acid–base homeostasis is the homeostatic regulation of the pH of the body's extracellular fluid (ECF).[1] The proper balance between the acids and bases (i.e. the pH) in the ECF is crucial for the normal physiology of the body, and cellular metabolism.[1] The pH of the intracellular fluid and the extracellular fluid need to be maintained at a constant level.[2]
Many extracellular proteins such as the plasma proteins and membrane proteins of the body's cells are very sensitive for their three dimensional structures to the extracellular pH.[3][4] Stringent mechanisms therefore exist to maintain the pH within very narrow limits. Outside the acceptable range of pH, proteins are denatured (i.e. their 3-D structure is disrupted), causing enzymes and ion channels (among others) to malfunction.
In humans and many other animals, acid–base homeostasis is maintained by multiple mechanisms involved in three lines of defence:[5][6]
- The first line of defence are the various chemical buffers which minimize pH changes that would otherwise occur in their absence. They do not correct pH deviations, but only serve to reduce the extent of the change that would otherwise occur. These buffers include the bicarbonate buffer system, the phosphate buffer system, and the protein buffer system.[7]
- The second line of defence of the extracellular fluid pH consists in controlling the carbonic acid concentration in the ECF. This is achieved by changes in the rate and depth of breathing (i.e. by hyperventilation or hypoventilation), which blows off or retains carbon dioxide (and thus carbonic acid) in the blood plasma as required.[5][8]
- The third line of defence is the renal system, which can add or remove bicarbonate ions to or from the ECF.[5] The bicarbonate is derived from metabolic carbon dioxide which is enzymatically converted to carbonic acid in the renal tubular cells.[5][9][10] The carbonic acid spontaneously dissociates into hydrogen ions and bicarbonate ions.[5] When the pH in the ECF tends to fall (i.e. become more acidic) the hydrogen ions are excreted into the urine, while the bicarbonate ions are secreted into the blood plasma, causing the plasma pH to rise (correcting the initial fall).[11] The converse happens if the pH in the ECF tends to rise: the bicarbonate ions are then excreted into the urine and the hydrogen ions into the blood plasma.
Physiological corrective measures make up the second and third lines of defence. This is because they operate by making changes to the buffers, each of which consists of two components: a weak acid and its conjugate base.[5][12] It is the ratio concentration of the weak acid to its conjugate base that determines the pH of the solution.[13] Thus, by manipulating firstly the concentration of the weak acid, and secondly that of its conjugate base, the pH of the extracellular fluid (ECF) can be adjusted very accurately to the correct value. The bicarbonate buffer, consisting of a mixture of carbonic acid (H2CO3) and a bicarbonate (HCO−
3) salt in solution, is the most abundant buffer in the extracellular fluid, and it is also the buffer whose acid to base ratio can be changed very easily and rapidly.[14]
An acid–base imbalance is known as acidaemia when the acidity is high, or alkalaemia when the acidity is low.
Acid–base balance
The pH of the extracellular fluid, including the blood plasma, is normally tightly regulated between 7.32 and 7.42,[15] by the chemical buffers, the respiratory system, and the renal system.[12][16][17][18]
Aqueous buffer solutions will react with strong acids or strong bases by absorbing excess hydrogen H+
ions, or hydroxide OH−
ions, replacing the strong acids and bases with weak acids and weak bases.[12] This has the effect of damping the effect of pH changes, or reducing the pH change that would otherwise have occurred. But buffers cannot correct abnormal pH levels in a solution, be that solution in a test tube or in the extracellular fluid. Buffers typically consist of a pair of compounds in solution, one of which is a weak acid and the other a weak base.[12] The most abundant buffer in the ECF consists of a solution of carbonic acid (H2CO3), and the bicarbonate (HCO−
3) salt of, usually, sodium (Na+).[5] Thus, when there is an excess of OH−
ions in the solution carbonic acid partially neutralizes them by forming H2O and bicarbonate (HCO−
3) ions.[5][14] Similarly an excess of H+ ions is partially neutralized by the bicarbonate component of the buffer solution to form carbonic acid (H2CO3), which, because it is a weak acid, remains largely in the undissociated form, releasing far fewer H+ ions into the solution than the original strong acid would have done.[5]
The pH of a buffer solution depends solely on the ratio of the molar concentrations of the weak acid to the weak base. The higher the concentration of the weak acid in the solution (compared to the weak base) the lower the resulting pH of the solution. Similarly, if the weak base predominates the higher the resulting pH.
This principle is exploited to regulate the pH of the extracellular fluids (rather than just buffering the pH). For the carbonic acid-bicarbonate buffer, a molar ratio of weak acid to weak base of 1:20 produces a pH of 7.4; and vice versa - when the pH of the extracellular fluids is 7.4 then the ratio of carbonic acid to bicarbonate ions in that fluid is 1:20.[13]
This relationship is described mathematically by the Henderson–Hasselbalch equation, which, when applied to the carbonic acid-bicarbonate buffer system in the extracellular fluids, states that:[13]
- where:

- pH is the negative logarithm (or cologarithm) of molar concentration of hydrogen ions in the ECF. It indicates the acidity in the ECF in an inverse manner: the lower the pH the greater the acidity of the solution.
- pKa H2CO3 is the cologarithm of the acid dissociation constant of carbonic acid. It is equal to 6.1.
- [HCO−
3] is the molar concentration of bicarbonate in the blood plasma - [H2CO3] is the molar concentration of carbonic acid in the ECF.
- However, since the carbonic acid concentration is directly proportional to the partial pressure of carbon dioxide () in the extracellular fluid, the equation can be rewritten as follows:[5][13]

- where:
- pH is the negative logarithm of molar concentration of hydrogen ions in the ECF, as before.
- [HCO−
3] is the molar concentration of bicarbonate in the plasma - PCO2 is the partial pressure of carbon dioxide in the blood plasma.

The pH of the extracellular fluids can thus be controlled by separately regulating the partial pressure of carbon dioxide (which determines the carbonic acid concentration), and the bicarbonate ion concentration in the extracellular fluids.
There are therefore at least two homeostatic negative feedback systems responsible for the regulation of the plasma pH. The first is the homeostatic control of the blood partial pressure of carbon dioxide, which determines the carbonic acid concentration in the plasma, and can change the pH of the arterial plasma within a few seconds.[5] The partial pressure of carbon dioxide in the arterial blood is monitored by the central chemoreceptors of the medulla oblongata, and so are part of the central nervous system.[5][19] These chemoreceptors are sensitive to the pH and levels of carbon dioxide in the cerebrospinal fluid.[13][11][19] (The peripheral chemoreceptors are located in the aortic bodies and carotid bodies adjacent to the arch of the aorta and to the bifurcation of the carotid arteries, respectively.[19] These chemoreceptors are sensitive primarily to changes in the partial pressure of oxygen in the arterial blood and are therefore not directly involved with pH homeostasis.[19])
The central chemoreceptors send their information to the respiratory centres in the medulla oblongata and pons of the brainstem.[11] The respiratory centres then determine the average rate of ventilation of the alveoli of the lungs, to keep the partial pressure carbon dioxide in the arterial blood constant. The respiratory center does so via motor neurons which activate the muscles of respiration (in particular the diaphragm).[5][20] A rise in the partial pressure of carbon dioxide in the arterial blood plasma above 5.3 kPa (40 mmHg) reflexly causes an increase in the rate and depth of breathing. Normal breathing is resumed when the partial pressure of carbon dioxide has returned to 5.3 kPa.[8] The converse happens if the partial pressure of carbon dioxide falls below the normal range. Breathing may be temporally halted, or slowed down to allow carbon dioxide to accumulate once more in the lungs and arterial blood.
The sensor for the plasma HCO−
3 concentration is not known for certain. It is very probable that the renal tubular cells of the distal convoluted tubules are themselves sensitive to the pH of the plasma. The metabolism of these cells produces CO2, which is rapidly converted to H+ and HCO−
3 through the action of carbonic anhydrase.[5][9][10] When the extracellular fluids tend towards acidity, the renal tubular cells secrete the H+ ions into the tubular fluid from where they exit the body via the urine. The HCO−
3 ions are simultaneously secreted into the blood plasma, thus raising the bicarbonate ion concentration in the plasma, lowering the carbonic acid/bicarbonate ion ratio, and consequently raising the pH of the plasma.[5][11] The converse happens when the plasma pH rises above normal: bicarbonate ions are excreted into the urine, and hydrogen ions into the plasma. These combine with the bicarbonate ions in the plasma to form carbonic acid (H+ + HCO−
3 = H2CO3), thus raising the carbonic acid:bicarbonate ratio in the extracellular fluids, and returning its pH to normal.[5]
In general, metabolism produces more waste acids than bases.[5] The urine is therefore generally acid. This urinary acidity is, to a certain extent, neutralized by the ammonia (NH3) which is excreted into the urine when glutamate and glutamine (carriers of excess, no longer needed, amino groups) are deaminated by the distal renal tubular epithelial cells.[5][10] Thus some of the "acid content" of the urine resides in the resulting ammonium ion (NH4+) content of the urine, though this has no effect on pH homeostasis of the extracellular fluids.[5][21]
Imbalance
Acid–base imbalance occurs when a significant insult causes the blood pH to shift out of the normal range (7.32 to 7.42[15]). An abnormally low pH in the ECF is called an acidaemia and an abnormally high pH is called an alkalaemia.
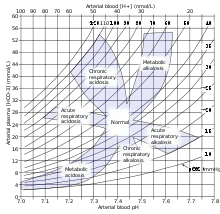
A second pair of terms is used in acid-base pathophysiology: "acidosis" and "alkalosis". They are often used as synonyms for "acidaemia" and "alkalaemia",[22] though this can cause confusion. "Acidaemia" refers unambiguously to the actual change in the pH of the ECF, whereas "acidosis", strictly speaking, refers to either a rise in the amount of carbonic acid in the ECF or to a decrease in the amount of HCO−
3 in the ECF. Either change would on its own (i.e. if left "uncompensated" by an alkalosis) cause an acidaemia.[22] Similarly an alkalosis refers to a rise in the concentration of bicarbonate in the ECF, or to a fall on the partial pressure of carbon dioxide, either of which would on their own raise the pH of the ECF above the normal value.[22] The terms acidosis and alkalosis should always be qualified by an adjective to indicate the cause of the disturbance: "respiratory" (indicating a change in the partial pressure of carbon dioxide),[23] or "metabolic" (indicating a change in the bicarbonate concentration of the ECF).[5][24] There are therefore four different acid-base problems: metabolic acidosis, respiratory acidosis, metabolic alkalosis, and respiratory alkalosis.[5] One or a combination these conditions may occur simultaneously. For instance, a metabolic acidosis (as in uncontrolled diabetes mellitus) is almost always partially compensated by a respiratory alkalosis (hyperventilation), or a respiratory acidosis can be completely or partially corrected by a metabolic alkalosis.
Whether an acidosis causes an acidaemia or not depends on the magnitude of the accompanying alkalosis. If the one cancels the other out (i.e. the ratio of carbonic acid to bicarbonate is returned to 1:20) then there is neither an acidaemia or an alkalaemia.[5] If the accompanying alkalosis overwhelms the acidosis then an alkalaemia results; whereas if the acidosis is greater than the alkalosis then an acidaemia is the inevitable result. The same considerations determine whether an alkalosis results in an alkalaemia or not.
The normal pH in the fetus differs from that in the adult. In the fetus, the pH in the umbilical vein pH is normally 7.25 to 7.45 and that in the umbilical artery is normally 7.18 to 7.38.[25]
See also
References
- Hamm, LL; Nakhoul, N; Hering-Smith, KS (7 December 2015). "Acid-Base Homeostasis". Clinical Journal of the American Society of Nephrology. 10 (12): 2232–42. doi:10.2215/CJN.07400715. PMC 4670772. PMID 26597304.
- J., Tortora, Gerard (2012). Principles of anatomy & physiology. Derrickson, Bryan. (13th ed.). Hoboken, NJ: Wiley. pp. 42–43. ISBN 9780470646083. OCLC 698163931.
- Macefield, Gary; Burke, David (1991). "Paraesthesiae and tetany induced by voluntary hyperventilation: increased excitability of cutaneous and motor axons". Brain. 114 (1): 527–540. doi:10.1093/brain/114.1.527. PMID 2004255.
- Stryer, Lubert (1995). Biochemistry (Fourth ed.). New York: W.H. Freeman and Company. pp. 347, 348. ISBN 0-7167-2009-4.
- Silverthorn, Dee Unglaub (2016). Human physiology. An integrated approach (Seventh, Global ed.). Harlow, England: Pearson. pp. 607–608, 666–673. ISBN 978-1-292-09493-9.
- Adrogué, H. E.; Adrogué, H. J. (April 2001). "Acid-base physiology". Respiratory Care. 46 (4): 328–341. ISSN 0020-1324. PMID 11345941.
- "184 26.4 ACID-BASE BALANCE | Anatomy and Physiology | OpenStax". openstax.org. Retrieved 2020-07-01.
- MedlinePlus Encyclopedia: Metabolic acidosis
- Tortora, Gerard J.; Anagnostakos, Nicholas P. (1987). Principles of anatomy and physiology (Fifth ed.). New York: Harper & Row, Publishers. pp. 581–582, 675–676. ISBN 0-06-350729-3.
- Stryer, Lubert (1995). Biochemistry (Fourth ed.). New York: W.H. Freeman and Company. pp. 39, 164, 630–631, 716–717. ISBN 0-7167-2009-4.
- Tortora, Gerard J.; Anagnostakos, Nicholas P. (1987). Principles of anatomy and physiology (Fifth ed.). New York: Harper & Row, Publishers. pp. 494, 556–582. ISBN 0-06-350729-3.
- Tortora, Gerard J.; Anagnostakos, Nicholas P. (1987). Principles of anatomy and physiology (Fifth ed.). New York: Harper & Row, Publishers. pp. 698–700. ISBN 0-06-350729-3.
- Bray, John J. (1999). Lecture notes on human physiology. Malden, Mass.: Blackwell Science. p. 556. ISBN 978-0-86542-775-4.
- Garrett, Reginald H.; Grisham, Charles M (2010). Biochemistry. Cengage Learning. p. 43. ISBN 978-0-495-10935-8.
- Diem, K.; Lentner, C. (1970). "Blood – Inorganic substances". in: Scientific Tables (Seventh ed.). Basle, Switzerland: CIBA-GEIGY Ltd. p. 527.
- MedlinePlus Encyclopedia: Blood gases
- Caroline, Nancy (2013). Nancy Caroline's Emergency care in the streets (7th ed.). Buffer systems: Jones & Bartlett Learning. pp. 347–349. ISBN 978-1449645861.
- Hamm, L. Lee; Nakhoul, Nazih; Hering-Smith, Kathleen S. (2015-12-07). "Acid-Base Homeostasis". Clinical Journal of the American Society of Nephrology. 10 (12): 2232–2242. doi:10.2215/CJN.07400715. ISSN 1555-905X. PMC 4670772. PMID 26597304.
- J., Tortora, Gerard (2010). Principles of anatomy and physiology. Derrickson, Bryan. (12th ed.). Hoboken, NJ: John Wiley & Sons. p. 907. ISBN 9780470233474. OCLC 192027371.
- Levitzky, Michael G. (2013). Pulmonary physiology (Eighth ed.). New York: McGraw-Hill Medical. p. Chapter 9. Control of Breathing. ISBN 978-0-07-179313-1.
- Rose, Burton; Helmut Rennke (1994). Renal Pathophysiology. Baltimore: Williams & Wilkins. ISBN 0-683-07354-0.
- Andertson, Douglas M. (2003). Dorland's illustrated medical dictionary (30th ed.). Philadelphia PA: Saunders. pp. 17, 49. ISBN 0-7216-0146-4.
- Brandis, Kerry. Acid-base physiology Respiratory acidosis: definition. http://www.anaesthesiamcq.com/AcidBaseBook/ab4_1.php
- Brandis, Kerry. Acid-base physiology Metabolic acidosis: definition. http://www.anaesthesiamcq.com/AcidBaseBook/ab5_1.php
- Yeomans, ER; Hauth, JC; Gilstrap, LC III; Strickland DM (1985). "Umbilical cord pH, PCO2, and bicarbonate following uncomplicated term vaginal deliveries (146 infants)". Am J Obstet Gynecol. 151 (6): 798–800. doi:10.1016/0002-9378(85)90523-x. PMID 3919587.