Delirium tremens
Delirium tremens (DTs) is a rapid onset of confusion usually caused by withdrawal from alcohol.[2] When it occurs, it is often three days into the withdrawal symptoms and lasts for two to three days.[2] Physical effects may include shaking, shivering, irregular heart rate, and sweating.[1] People may also hallucinate.[2] Occasionally, a very high body temperature or seizures may result in death.[2] Alcohol is one of the most dangerous drugs from which to withdraw.[5]
| Delirium tremens | |
|---|---|
.jpg.webp) | |
| An alcoholic man with delirium tremens on his deathbed, surrounded by his terrified family. The text "L'Alcool Tue" means "Alcohol Kills" in French. | |
| Specialty | Psychiatry, critical care medicine |
| Symptoms | Confusion, hallucination, shaking, shivering, irregular heart rate, sweating[1][2] |
| Complications | Very high body temperature, seizures[2] |
| Usual onset | Rapid[2] |
| Duration | 2–3 days[2] |
| Causes | Withdrawal from alcohol[2] |
| Differential diagnosis | Benzodiazepine withdrawal syndrome, barbiturate withdrawal[3] |
| Treatment | Intensive care unit, benzodiazepines, thiamine[2] |
| Prognosis | Risk of death ~2% (treatment), 25% (no treatment)[4] |
| Frequency | ~4% of those withdrawing from alcohol[2] |
Delirium tremens typically only occurs in people with a high intake of alcohol for more than a month.[6] A similar syndrome may occur with benzodiazepine and barbiturate withdrawal.[3] Withdrawal from stimulants such as cocaine do not have major medical complications.[7] In a person with delirium tremens it is important to rule out other associated problems such as electrolyte abnormalities, pancreatitis, and alcoholic hepatitis.[2]
Prevention is by treating withdrawal symptoms.[2] If delirium tremens occurs, aggressive treatment improves outcomes.[2] Treatment in a quiet intensive care unit with sufficient light is often recommended.[2] Benzodiazepines are the medication of choice with diazepam, lorazepam, chlordiazepoxide, and oxazepam all commonly used.[6] They should be given until a person is lightly sleeping.[2] The antipsychotic haloperidol may also be used.[2] The vitamin thiamine is recommended.[2] Mortality without treatment is between 15% and 40%.[4] Currently death occurs in about 1% to 4% of cases.[2]
About half of people with alcoholism will develop withdrawal symptoms upon reducing their use.[2] Of these, 3% to 5% develop DTs or have seizures.[2] The name delirium tremens was first used in 1813; however, the symptoms were well described since the 1700s.[6] The word "delirium" is Latin for "going off the furrow," a plowing metaphor.[4] It is also called shaking frenzy and Saunders-Sutton syndrome.[4] Nicknames include the shakes, barrel-fever, blue horrors, bottleache, bats, drunken horrors, elephants, gallon distemper, quart mania, heebie jeebies, pink spiders and riding the ghost train.[8]
Signs and symptoms
The main symptoms of delirium tremens are nightmares, agitation, global confusion, disorientation, visual and[9] auditory hallucinations, tactile hallucinations, fever, high blood pressure, heavy sweating, and other signs of autonomic hyperactivity (fast heart rate and high blood pressure). These symptoms may appear suddenly, but typically develop two to three days after the stopping of heavy drinking, being worst on the fourth or fifth day.[10] Also, these symptoms are characteristically worse at night.[11] In general, DT is considered the most severe manifestation of alcohol withdrawal and occurs 3–10 days following the last drink.[9] Other common symptoms include intense perceptual disturbance such as visions of insects, snakes, or rats. These may be hallucinations or illusions related to the environment, e.g., patterns on the wallpaper or in the peripheral vision that the patient falsely perceives as a resemblance to the morphology of an insect, and are also associated with tactile hallucinations such as sensations of something crawling on the subject—a phenomenon known as formication. Delirium tremens usually includes extremely intense feelings of "impending doom". Severe anxiety and feelings of imminent death are common DT symptoms.
DT can sometimes be associated with severe, uncontrollable tremors of the extremities and secondary symptoms such as anxiety, panic attacks and paranoia. Confusion is often noticeable to onlookers as those with DT will have trouble forming simple sentences or making basic logical calculations.
DT should be distinguished from alcoholic hallucinosis, the latter of which occurs in approximately 20% of hospitalized alcoholics and does not carry a significant mortality. In contrast, DT occurs in 5–10% of alcoholics and carries up to 15% mortality with treatment and up to 35% mortality without treatment.[12] DT is characterized by the presence of altered sensorium; that is, a complete hallucination without any recognition of the real world. DT has extreme autonomic hyperactivity (high pulse, blood pressure, and rate of breathing), and 35-60% of patients have a fever. Some patients experience seizures.
Causes
Delirium tremens is mainly caused by a long period of drinking being stopped abruptly. Withdrawal leads to a biochemical regulation cascade.
Another cause of delirium tremens is abrupt stopping of tranquilizer drugs of the barbiturate or benzodiazepine classes in a person with a relatively strong addiction to them. Because these tranquilizers' primary pharmacological and physiological effects stem from their manipulation of the GABA chemical and transmitter somatic system, the same neurotransmitter system affected by alcohol, delirium tremens can occur upon abrupt decrease of dosage in those who are heavily dependent. These DTs are much the same as those caused by alcohol and so is the attendant withdrawal syndrome of which they are a manifestation. That is the primary reason benzodiazepines are such an effective treatment for DTs, despite also being the cause of them in many cases. Because ethanol and tranquilizers such as barbiturates and benzodiazepines function as positive allosteric modulators at GABAA receptors, the brain, in its desire to equalize an unbalanced chemical system, triggers the abrupt stopping of the production of endogenous GABA. This decrease becomes more and more marked as the addiction becomes stronger and as higher doses are needed to cause intoxication. In addition to having sedative properties, GABA is an immensely important regulatory neurotransmitter that controls the heart rate, blood pressure, and seizure threshold among myriad other important autonomic nervous subsystems.
Delirium tremens is most common in people who have a history of alcohol withdrawal, especially in those who drink the equivalent of 7 to 8 US pints (3 to 4 l) of beer or 1 US pint (0.5 l) of distilled beverage daily. Delirium tremens also commonly affects those with a history of habitual alcohol use or alcoholism that has existed for more than 10 years.[13]
Pathophysiology
Delirium tremens is a component of alcohol withdrawal hypothesized to be the result of compensatory changes in response to chronic alcohol abuse. Alcohol positively allosterically modulates the binding of GABA, enhancing its effect and resulting in inhibition of neurons projecting into the nucleus accumbens, as well as inhibiting NMDA receptors. This combined with desensitization of alpha-2 adrenergic receptors, results in a homeostatic upregulation of these systems in chronic alcohol use. When alcohol use ceases, the unregulated mechanisms result in hyperexcitability of neurons as natural GABAergic systems are down-regulated and excitatory glutamatergic systems are unregulated. This combined with increased noradrenergic activity results in the symptoms of delirium tremens.[14]
Diagnosis
Diagnosis is mainly based on symptoms. In a person with delirium tremens it is important to rule out other associated problems such as electrolyte abnormalities, pancreatitis, and alcoholic hepatitis.[2]
Treatment
Delirium tremens due to alcohol withdrawal can be treated with benzodiazepines. High doses may be necessary to prevent death.[15] Amounts given are based on the symptoms. Typically the person is kept sedated with benzodiazepines, such as diazepam, lorazepam, chlordiazepoxide, or oxazepam.
In some cases antipsychotics, such as haloperidol may also be used. Older drugs such as paraldehyde and clomethiazole were formerly the traditional treatment but have now largely been superseded by the benzodiazepines.
Acamprosate is occasionally used in addition to other treatments, and is then carried on into long-term use to reduce the risk of relapse. If status epilepticus occurs it is treated in the usual way.
It can also be helpful to provide a well lit room as people often have hallucinations.[16]
Alcoholic beverages can also be prescribed as a treatment for delirium tremens,[17] but this practice is not universally supported.[18]
High doses of thiamine often by the intravenous route is also recommended.[2]
Society and culture

Nicknames include "the horrors", "the shakes", "the bottleache", "quart mania", "ork orks", "gallon distemper", "the zoots", "barrel fever", "the 750 itch", "pint paralysis", “seeing pink elephants”. Another nickname is "the Brooklyn Boys" found in Eugene O'Neill's one-act play Hughie set in Times Square in the 1920s.[19]
Writer Jack Kerouac details his experiences with delirium tremens in his book Big Sur.[20]
One of the characters in Joseph Conrad's novel Lord Jim experiences "DTs of the worst kind" with symptoms that include seeing millions of pink frogs.
In the 1995 film Leaving Las Vegas, Nicolas Cage plays a suicidal alcoholic who rids himself of all his possessions and travels to Las Vegas to drink himself to death. During his travels he experiences delirium tremens on a couch after waking up from a binge and crawls in pain to the refrigerator for more vodka. Cage's performance as Ben Sanderson in the film won the Academy Award for Best Actor in 1995.
In the 1945 film The Lost Weekend, Ray Milland won the Academy Award for Best Actor for his depiction of a character who experiences delirium tremens after being hospitalized, hallucinating that he saw a bat fly in and eat a mouse poking through a wall.[21][22][23]
English author George Eliot provides a case involving delirium tremens in her novel Middlemarch (1871–72). Alcoholic scoundrel John Raffles, both an abusive stepfather of Joshua Riggs and blackmailing nemesis of financier Nicholas Bulstrode, dies, whose "death was due to delirium tremens" while at Peter Featherstone's Stone Court property. Housekeeper Mrs Abel provides Raffles’ final night of care per Bulstrode's instruction whose directions given to Abel stand adverse to Dr Tertius Lydgate's orders.
Pages 700–710, Chapters 69-70: "‘Remember, if he calls for liquors of any sort, not to give it to him.’" (Lydgate to Bulstrode). "...he gave directions to Bulstrode as to the doses, and the point at which they should cease. He insisted on the risk of not ceasing, and repeated his order that no alcohol should be given.’ (Bulstrode reflecting): "The thought was, that he had not told Mrs Abel when the dose of opium must cease. ... He walked up-stairs, candle in hand, not knowing whether he should straitaway enter his own room and go to bed, or turn to the patient’s room and rectify his omission. ... He turned to his own room. Before he had quite undressed, Mrs Abel rapped at his door ...‘If you please sir, should I have no brandy nor nothing to give the poor creetur? ...When I nursed my poor master, Mr Robisson, I had to give him port-wine and brandy constant, and a big glass at a time,’ added Mrs Abel with a touch of remonstrance in her tone. ...a key was thrust through the inch of doorway, and Mr Bulstrode said huskily, ‘That is the key of the wine-cooler. You will find plenty of brandy there.’"
American writer Mark Twain describes an episode of delirium tremens in his book The Adventures of Huckleberry Finn (1884). In Chapter 6, Huck states about his father, "After supper pap took the jug, and said he had enough whisky there for two drunks and one delirium tremens. That was always his word." Subsequently, Pap Finn runs around with hallucinations of snakes and chases Huck around their cabin with a knife in an attempt to kill him, thinking Huck is the "Angel of Death".
French writer Émile Zola's novel The Drinking Den (L'Assommoir) includes a character who suffers delirium tremens by the end of the book. It is Coupeau, the main character Gervaise's husband.
The M*A*S*H (TV series) episode "Bottoms Up" (Season 9, Episode 15) featured a side story about a nurse (Cpt. Helen Whitfield) who was found to be drinking heavily off-duty. By the culmination of the episode, after a confrontation by Maj. Margaret Houlihan, the character swears off her alcoholism and presumably quits immediately. At mealtime, an unspecified time later (roughly 48 hours, according to Maj. Houlihan), Whitfield becomes hysterical upon being served food in the Mess tent, claiming that there are things crawling onto her from it. Margaret and Col. Sherman Potter subdue her. Potter, having recognized the symptoms of delirium tremens (which he abbreviates "the DTs"), orders 5 ml of paraldehyde from a witnessing nurse.
Russian composer Modest Mussorgsky died of delirium tremens.[24]
The Belgian beer "Delirium Tremens" is named after delirium tremens and is also using a pink elephant as its logo to highlight one of the symptoms of delirium tremens.[25]
See also
References
- Healy, David (3 December 2008). Psychiatric Drugs Explained. Elsevier Health Sciences. p. 237. ISBN 978-0-7020-2997-4. Archived from the original on 8 September 2017.
- Schuckit, MA (27 November 2014). "Recognition and management of withdrawal delirium (delirium tremens)". The New England Journal of Medicine. 371 (22): 2109–13. doi:10.1056/NEJMra1407298. PMID 25427113.
- Posner, Jerome B. (2007). Plum and Posner's Diagnosis of Stupor and Coma (4 ed.). Oxford: Oxford University Press, USA. p. 283. ISBN 9780198043362. Archived from the original on 2016-03-04.
- Blom, Jan Dirk (2010). A dictionary of hallucinations (. ed.). New York: Springer. p. 136. ISBN 9781441912237. Archived from the original on 2016-03-04.
- Fisher, Gary L. (2009). Encyclopedia of substance abuse prevention, treatment, & recovery. Los Angeles: SAGE. p. 1005. ISBN 9781452266015. Archived from the original on 2015-12-22.
- Stern, TA; Gross, AF; Stern, TW; Nejad, SH; Maldonado, JR (2010). "Current approaches to the recognition and treatment of alcohol withdrawal and delirium tremens: "old wine in new bottles" or "new wine in old bottles"". Primary Care Companion to the Journal of Clinical Psychiatry. 12 (3). doi:10.4088/PCC.10r00991ecr. PMC 2947546. PMID 20944765.
- Galanter, Marc; Kleber, Herbert D (1 July 2008). The American Psychiatric Publishing Textbook of Substance Abuse Treatment (4th ed.). United States of America: American Psychiatric Publishing Inc. p. 58. ISBN 978-1-58562-276-4. Archived from the original on 4 March 2016.
- Baldwin, Dan (2002). Just the FAQ's, Please, About Alcohol and Drug Abuse: Frequently Asked Questions from Families. America Star Books. pp. Chapter four. ISBN 9781611028706. Archived from the original on 2016-03-04.
- Delirium Tremens (DTs)~clinical at eMedicine
- Hales, R.; Yudofsky, S.; Talbott, J. (1999). Textbook of Psychiatry (3rd ed.). London: The American Psychiatric Press.
- Gelder et al, 2005 p188 Psychiatry 3rd Ed. oxford: New York.
- Delirium Tremens (DTs): Prognosis at eMedicine
- MedlinePlus Encyclopedia: Delirium Tremens
- Stern, Theodore A.; Gross, Anne F.; Stern, Thomas W.; Nejad, Shamim H.; Maldonado, Jose R. (1 January 2010). "Current Approaches to the Recognition and Treatment of Alcohol Withdrawal and Delirium Tremens: "Old Wine in New Bottles" or "New Wine in Old Bottles"". Primary Care Companion to the Journal of Clinical Psychiatry. 12 (3). doi:10.4088/PCC.10r00991ecr. ISSN 1523-5998. PMC 2947546. PMID 20944765.
- Wolf KM, Shaughnessy AF, Middleton DB (1993). "Prolonged delirium tremens requiring massive doses of medication". J Am Board Fam Pract. 6 (5): 502–4. PMID 8213241.
- NCLEX-RN in a Flash. Jones & Bartlett Learning. 2009. ISBN 9780763761974.
- Rosenbaum M, McCarty T (2002). "Alcohol prescription by surgeons in the prevention and treatment of delirium tremens: Historic and current practice". General Hospital Psychiatry. 24 (4): 257–259. doi:10.1016/S0163-8343(02)00188-3. PMID 12100836.
- Sattar SP, Qadri SF, Warsi MK, Okoye C, Din AU, Padala PR, Bhatia SC (2006). "Use of alcoholic beverages in VA medical centers". Substance Abuse Treatment, Prevention, and Policy. 1: 30. doi:10.1186/1747-597X-1-30. PMC 1624810. PMID 17052353.
- Paulson, Michael, "Gambling on O’Neill: Forest Whitaker Makes His Broadway Debut in ‘Hughie’" Archived 2016-02-29 at the Wayback Machine, New York Times, February 3, 2016. Retrieved 2016-02-03.
- Summary and analysis of novel Archived 2011-06-28 at the Wayback Machine
- Bailey, Blake. "Weekend in the Sun; Hollywood went wild over Charles Jackson and his 1944 best-seller, The Lost Weekend. Jackson reciprocated, thrilled that the celebrated Billy Wilder wanted to direct his dark, autobiographical novel of addiction. But would the result—a cinematic classic—destroy his literary achievement?" Archived 2016-04-13 at the Wayback Machine, Vanity Fair (magazine), February 28, 2013. Accessed February 15, 2017. "That summer, Hollywood columns had buzzed with rumors about who would play Don Birnam, the genteel alcoholic who ends up howling with delirium tremens. The role had been turned down by everyone from Cary Grant to Gary Cooper before the Welshman Ray Milland took it, refusing to heed an all but universal warning that he was committing 'career suicide.'"
- Cameron, Kate. "The Lost Weekend effectively portrays the damage caused by alcoholism on screen" Archived 2017-02-16 at the Wayback Machine, New York Daily News, January 2, 1945, reprinted February 17, 2015. Accessed February 15, 2017. "If you read the book, which was a best-seller last year, you know that Jackson did a remarkable job of recording the actions of Birnam, during a weekend binge of monumental proportions, and in setting down in graphic prose the effects produced on him by liquor. In adapting the book to the screen, Brackett and Wilder have accomplished an equally remarkable feat of projecting a case of delirium tremens on screen."
- Armstrong, Richard. Billy Wilder, American Film Realist Archived 2017-02-17 at the Wayback Machine, p. 41. McFarland & Company, 2004. ISBN 9780786421190. Accessed February 15, 2017. "Finally, Don's hallucination in which a wheeling bat devours a mouse places The Lost Weekend in a direct line of descent from the Gothicism of the '30s Universal horror cycle."
- Алкогольная трагедия легендарного композитора Мусоргского
- Belgian, Beers (2020-05-29). "The Pink Elephant beer: Delirium Tremens". Belgian Beers. Retrieved 2020-05-29.
External links
| Classification | |
|---|---|
| External resources |
| General | 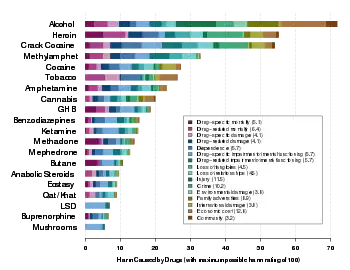 | ||||
|---|---|---|---|---|---|
| Combined substance use |
| ||||
| Alcohol |
| ||||
| Caffeine | |||||
| Cannabis |
| ||||
| Cocaine |
| ||||
| Hallucinogen | |||||
| Nicotine | |||||
| Opioids |
| ||||
| Sedative / hypnotic | |||||
| Stimulants | |||||
| Volatile solvent |
| ||||
| Alcohol use |
| ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Alcohol control |
| ||||||||||||||||
| Related | |||||||||||||||||
| |||||||||||||||||