Substance abuse
Substance abuse, also known as drug abuse, is use of a drug in amounts or by methods which are harmful to the individual or others. It is a form of substance-related disorder. Differing definitions of drug abuse are used in public health, medical and criminal justice contexts. In some cases criminal or anti-social behaviour occurs when the person is under the influence of a drug, and long term personality changes in individuals may occur as well.[4] In addition to possible physical, social, and psychological harm, use of some drugs may also lead to criminal penalties, although these vary widely depending on the local jurisdiction.[5]
| Substance abuse | |
|---|---|
| Other names | Drug abuse, substance use disorder, substance misuse disorder |
 | |
| A tin containing drugs and drug paraphernalia | |
| Specialty | Psychiatry |
| Complications | Drug overdose |
| Frequency | 27 million[1][2] |
| Deaths | 307,400 (2015)[3] |

Drugs most often associated with this term include: alcohol, amphetamines, barbiturates, benzodiazepines, cannabis, cocaine, hallucinogens, methaqualone, and opioids. The exact cause of substance abuse is not clear, with the two predominant theories being: either a genetic disposition which is learned from others, or a habit which if addiction develops, manifests itself as a chronic debilitating disease.[6]
In 2010 about 5% of people (230 million) used an illicit substance.[1] Of these 27 million have high-risk drug use otherwise known as recurrent drug use causing harm to their health, psychological problems, or social problems that put them at risk of those dangers.[1][2] In 2015 substance use disorders resulted in 307,400 deaths, up from 165,000 deaths in 1990.[3][7] Of these, the highest numbers are from alcohol use disorders at 137,500, opioid use disorders at 122,100 deaths, amphetamine use disorders at 12,200 deaths, and cocaine use disorders at 11,100.[3]
Classification
Public health definitions

Public health practitioners have attempted to look at substance use from a broader perspective than the individual, emphasizing the role of society, culture, and availability. Some health professionals choose to avoid the terms alcohol or drug "abuse" in favor of language they consider more objective, such as "substance and alcohol type problems" or "harmful/problematic use" of drugs. The Health Officers Council of British Columbia — in their 2005 policy discussion paper, A Public Health Approach to Drug Control in Canada — has adopted a public health model of psychoactive substance use that challenges the simplistic black-and-white construction of the binary (or complementary) antonyms "use" vs. "abuse".[8] This model explicitly recognizes a spectrum of use, ranging from beneficial use to chronic dependence.
Medical definitions
'Drug abuse' is no longer a current medical diagnosis in either of the most used diagnostic tools in the world, the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (DSM), and the World Health Organization's International Statistical Classification of Diseases (ICD).
Value judgment
Philip Jenkins suggests that there are two issues with the term "drug abuse". First, what constitutes a "drug" is debatable. For instance, GHB, a naturally occurring substance in the central nervous system is considered a drug, and is illegal in many countries, while nicotine is not officially considered a drug in most countries.
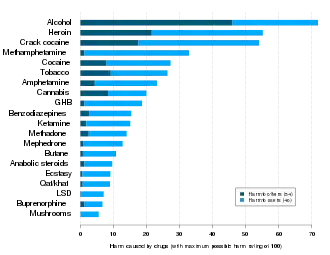
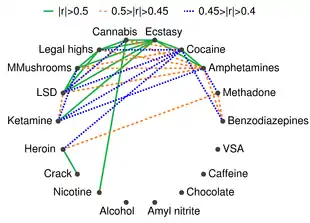
Second, the word "abuse" implies a recognized standard of use for any substance. Drinking an occasional glass of wine is considered acceptable in most Western countries, while drinking several bottles is seen as an abuse. Strict temperance advocates, who may or may not be religiously motivated, would see drinking even one glass as an abuse. Some groups even condemn caffeine use in any quantity. Similarly, adopting the view that any (recreational) use of cannabis or substituted amphetamines constitutes drug abuse implies a decision made that the substance is harmful, even in minute quantities.[11] In the U.S., drugs have been legally classified into five categories, schedule I, II, III, IV, or V in the Controlled Substances Act. The drugs are classified on their deemed potential for abuse. Usage of some drugs is strongly correlated.[12] For example, the consumption of seven illicit drugs (amphetamines, cannabis, cocaine, ecstasy, legal highs, LSD, and magic mushrooms) is correlated and the Pearson correlation coefficient r>0.4 in every pair of them; consumption of cannabis is strongly correlated (r>0.5) with usage of nicotine (tobacco), heroin is correlated with cocaine (r>0.4) and methadone (r>0.45), and is strongly correlated with crack (r>0.5)[12]
Drug misuse
Drug misuse is a term used commonly when prescription medication with sedative, anxiolytic, analgesic, or stimulant properties are used for mood alteration or intoxication ignoring the fact that overdose of such medicines can sometimes have serious adverse effects. It sometimes involves drug diversion from the individual for whom it was prescribed.
Prescription misuse has been defined differently and rather inconsistently based on status of drug prescription, the uses without a prescription, intentional use to achieve intoxicating effects, route of administration, co-ingestion with alcohol, and the presence or absence of dependence symptoms.[13][14] Chronic use of certain substances leads to a change in the central nervous system known as a 'tolerance' to the medicine such that more of the substance is needed in order to produce desired effects. With some substances, stopping or reducing use can cause withdrawal symptoms to occur,[15] but this is highly dependent on the specific substance in question.
The rate of prescription drug use is fast overtaking illegal drug use in the United States. According to the National Institute of Drug Abuse, 7 million people were taking prescription drugs for nonmedical use in 2010. Among 12th graders, nonmedical prescription drug use is now second only to cannabis.[16] In 2011, "Nearly 1 in 12 high school seniors reported nonmedical use of Vicodin; 1 in 20 reported such use of OxyContin."[17] Both of these drugs contain opioids. A 2017 survey of 12th graders in the United States, found misuse of OxyContin of 2.7 percent, compared to 5.5 percent at its peak in 2005.[18] Misuse of the combination hydrocodone/paracetamol was at its lowest since a peak of 10.5 percent in 2003.[18] This decrease may be related to public health initiatives and decreased availability.[18]
Avenues of obtaining prescription drugs for misuse are varied: sharing between family and friends, illegally buying medications at school or work, and often "doctor shopping" to find multiple physicians to prescribe the same medication, without knowledge of other prescribers.
Increasingly, law enforcement is holding physicians responsible for prescribing controlled substances without fully establishing patient controls, such as a patient "drug contract". Concerned physicians are educating themselves on how to identify medication-seeking behavior in their patients, and are becoming familiar with "red flags" that would alert them to potential prescription drug abuse.[19]
Signs and symptoms
| Drug | Drug class | Physical harm |
Dependence liability |
Social harm |
Avg. harm |
|---|---|---|---|---|---|
| Methamphetamine | CNS stimulant | 3.00 | 2.80 | 2.72 | 2.92 |
| Heroin | Opioid | 2.78 | 3.00 | 2.54 | 2.77 |
| Cocaine | CNS stimulant | 2.33 | 2.39 | 2.17 | 2.30 |
| Barbiturates | CNS depressant | 2.23 | 2.01 | 2.00 | 2.08 |
| Methadone | Opioid | 1.86 | 2.08 | 1.87 | 1.94 |
| Alcohol | CNS depressant | 1.40 | 1.93 | 2.21 | 1.85 |
| Ketamine | Dissociative anesthetic | 2.00 | 1.54 | 1.69 | 1.74 |
| Benzodiazepines | Benzodiazepine | 1.63 | 1.83 | 1.65 | 1.70 |
| Amphetamine | CNS stimulant | 1.81 | 1.67 | 1.50 | 1.66 |
| Tobacco | Tobacco | 1.24 | 2.21 | 1.42 | 1.62 |
| Buprenorphine | Opioid | 1.60 | 1.64 | 1.49 | 1.58 |
| Cannabis | Cannabinoid | 0.99 | 1.51 | 1.50 | 1.33 |
| Solvent drugs | Inhalant | 1.28 | 1.01 | 1.52 | 1.27 |
| 4-MTA | Designer SSRA | 1.44 | 1.30 | 1.06 | 1.27 |
| LSD | Psychedelic | 1.13 | 1.23 | 1.32 | 1.23 |
| Methylphenidate | CNS stimulant | 1.32 | 1.25 | 0.97 | 1.18 |
| Anabolic steroids | Anabolic steroid | 1.45 | 0.88 | 1.13 | 1.15 |
| GHB | Neurotransmitter | 0.86 | 1.19 | 1.30 | 1.12 |
| Ecstasy | Empathogenic stimulant | 1.05 | 1.13 | 1.09 | 1.09 |
| Alkyl nitrites | Inhalant | 0.93 | 0.87 | 0.97 | 0.92 |
| Khat | CNS stimulant | 0.50 | 1.04 | 0.85 | 0.80 |
Notes about the harm ratings
The Physical harm, Dependence liability, and Social harm scores were each computed from the average of three distinct ratings.[20] The highest possible harm rating for each rating scale is 3.0.[20] Physical harm is the average rating of the scores for acute binge use, chronic use, and intravenous use.[20] Dependence liability is the average rating of the scores for intensity of pleasure, psychological dependence, and physical dependence.[20] Social harm is the average rating of the scores for drug intoxication, health-care costs, and other social harms.[20] Average harm was computed as the average of the Physical harm, Dependence liability, and Social harm scores. | |||||
Depending on the actual compound, drug abuse including alcohol may lead to health problems, social problems, morbidity, injuries, unprotected sex, violence, deaths, motor vehicle accidents, homicides, suicides, physical dependence or psychological addiction.[21]
There is a high rate of suicide in alcoholics and other drug abusers. The reasons believed to cause the increased risk of suicide include the long-term abuse of alcohol and other drugs causing physiological distortion of brain chemistry as well as the social isolation.[22] Another factor is the acute intoxicating effects of the drugs may make suicide more likely to occur. Suicide is also very common in adolescent alcohol abusers, with 1 in 4 suicides in adolescents being related to alcohol abuse.[23] In the US, approximately 30% of suicides are related to alcohol abuse. Alcohol abuse is also associated with increased risks of committing criminal offences including child abuse, domestic violence, rapes, burglaries and assaults.[24]
Drug abuse, including alcohol and prescription drugs, can induce symptomatology which resembles mental illness. This can occur both in the intoxicated state and also during the withdrawal state. In some cases these substance induced psychiatric disorders can persist long after detoxification, such as prolonged psychosis or depression after amphetamine or cocaine abuse. A protracted withdrawal syndrome can also occur with symptoms persisting for months after cessation of use. Benzodiazepines are the most notable drug for inducing prolonged withdrawal effects with symptoms sometimes persisting for years after cessation of use. Both alcohol, barbiturate as well as benzodiazepine withdrawal can potentially be fatal. Abuse of hallucinogens can trigger delusional and other psychotic phenomena long after cessation of use.
Cannabis may trigger panic attacks during intoxication and with continued use, it may cause a state similar to dysthymia.[25] Researchers have found that daily cannabis use and the use of high-potency cannabis are independently associated with a higher chance of developing schizophrenia and other psychotic disorders.[26][27][28]
Severe anxiety and depression are commonly induced by sustained alcohol abuse, which in most cases abates with prolonged abstinence. Even sustained moderate alcohol use may increase anxiety and depression levels in some individuals. In most cases these drug induced psychiatric disorders fade away with prolonged abstinence.[29] Similarly, although substance abuse induces many changes to the brain, there is evidence that many of these alterations are reversed following periods of prolonged abstinence.[30]
Impulsivity
Impulsivity is characterized by actions based on sudden desires, whims, or inclinations rather than careful thought.[31] Individuals with substance abuse have higher levels of impulsivity,[32] and individuals who use multiple drugs tend to be more impulsive.[32] A number of studies using the Iowa gambling task as a measure for impulsive behavior found that drug using populations made more risky choices compared to healthy controls.[33] There is a hypothesis that the loss of impulse control may be due to impaired inhibitory control resulting from drug induced changes that take place in the frontal cortex.[34] The neurodevelopmental and hormonal changes that happen during adolescence may modulate impulse control that could possibly lead to the experimentation with drugs and may lead to the road of addiction.[35] Impulsivity is thought to be a facet trait in the neuroticism personality domain (overindulgence/negative urgency) which is prospectively associated with the development of substance abuse.[36]
Screening and assessment
There are several different screening tools that have been validated for use with adolescents such as the CRAFFT Screening Test[37] and in adults the CAGE questionnaire.[38]
Some recommendations for screening tools for substance misuse in pregnancy include that they take less than 10 minutes, should be used routinely, include an educational component. Tools suitable for pregnant women include i.a. 4Ps, T-ACE, TWEAK, TQDH (Ten-Question Drinking History), and AUDIT.[39]
Given that addiction manifests in structural changes to the brain, it is possible that non-invasive neuroimaging scans obtained via MRI could be used to help diagnose addiction in the future.[30]
Treatment
Psychological
From the applied behavior analysis literature, behavioral psychology, and from randomized clinical trials, several evidenced based interventions have emerged: behavioral marital therapy, motivational Interviewing, community reinforcement approach, exposure therapy, contingency management[40][41] They help suppress cravings and mental anxiety, improve focus on treatment and new learning behavioral skills, ease withdrawal symptoms and reduce the chances of relapse.[42]
In children and adolescents, cognitive behavioral therapy (CBT)[43] and family therapy[44] currently has the most research evidence for the treatment of substance abuse problems. Well-established studies also include ecological family-based treatment and group CBT.[45] These treatments can be administered in a variety of different formats, each of which has varying levels of research support[46] Research has shown that what makes group CBT most effective is that it promotes the development of social skills, developmentally appropriate emotional regulatory skills and other interpersonal skills.[47] A few integrated[48] treatment models, which combines parts from various types of treatment, have also been seen as both well-established or probably effective.[45] A study on maternal alcohol and other drug use has shown that integrated treatment programs have produced significant results, resulting in higher negative results on toxicology screens.[48] Additionally, brief school-based interventions have been found to be effective in reducing adolescent alcohol and cannabis use and abuse.[49] Motivational interviewing can also be effective in treating substance use disorder in adolescents.[50][51]
Alcoholics Anonymous and Narcotics Anonymous are one of the most widely known self-help organizations in which members support each other not to use alcohol.[52] Social skills are significantly impaired in people suffering from alcoholism due to the neurotoxic effects of alcohol on the brain, especially the prefrontal cortex area of the brain.[53] It has been suggested that social skills training adjunctive to inpatient treatment of alcohol dependence is probably efficacious,[54] including managing the social environment.
Medication
A number of medications have been approved for the treatment of substance abuse.[55] These include replacement therapies such as buprenorphine and methadone as well as antagonist medications like disulfiram and naltrexone in either short acting, or the newer long acting form. Several other medications, often ones originally used in other contexts, have also been shown to be effective including bupropion and modafinil. Methadone and buprenorphine are sometimes used to treat opiate addiction.[56] These drugs are used as substitutes for other opioids and still cause withdrawal symptoms but they facilitate the tapering off process in a controlled fashion.
Antipsychotic medications have not been found to be useful.[57] Acamprostate[58] is a glutamatergic NMDA antagonist, which helps with alcohol withdrawal symptoms because alcohol withdrawal is associated with a hyperglutamatergic system.
Heroin-assisted treatment
Three countries in Europe have active HAT programs, namely England, the Netherlands and Switzerland. Despite critical voices by conservative think-tanks with regard to these liberal approaches, significant progress in the reduction of drug-related deaths has been achieved in those countries. For example the US, devoid of such measures, have seen large increases in drug-related deaths since 2000 (mostly related to heroin use), while Switzerland has seen large decreases. In 2018, approximately 60,000 people have died of drug overdoses in America, while in the same time period, Switzerland's drug deaths were at 260. Relative to the population of these countries, the US has 10-times more drug-related deaths compared to the Swiss Confederation, which in effect illustrates the efficacy of HAT to reduce fatal outcomes in opiate/opioid addiction.[59][60]
Dual diagnosis
It is common for individuals with drugs use disorder to have other psychological problems.[61] The terms “dual diagnosis” or “co-occurring disorders,” refer to having a mental health and substance use disorder at the same time. According to the British Association for Psychopharmacology (BAP), “symptoms of psychiatric disorders such as depression, anxiety and psychosis are the rule rather than the exception in patients misusing drugs and/or alcohol.”[62]
Individuals who have a comorbid psychological disorder often have a poor prognosis if either disorder is untreated.[61] Historically most individuals with dual diagnosis either received treatment only for one of their disorders or they didn't receive any treatment all. However, since the 1980s, there has been a push towards integrating mental health and addiction treatment. In this method, neither condition is considered primary and both are treated simultaneously by the same provider.[62]
Epidemiology

The initiation of drug use including alcohol is most likely to occur during adolescence, and some experimentation with substances by older adolescents is common. For example, results from 2010 Monitoring the Future survey, a nationwide study on rates of substance use in the United States, show that 48.2% of 12th graders report having used an illicit drug at some point in their lives.[63] In the 30 days prior to the survey, 41.2% of 12th graders had consumed alcohol and 19.2% of 12th graders had smoked tobacco cigarettes.[63] In 2009 in the United States about 21% of high school students have taken prescription drugs without a prescription.[64] And earlier in 2002, the World Health Organization estimated that around 140 million people were alcohol dependent and another 400 million with alcohol-related problems.[65]
Studies have shown that the large majority of adolescents will phase out of drug use before it becomes problematic. Thus, although rates of overall use are high, the percentage of adolescents who meet criteria for substance abuse is significantly lower (close to 5%).[66] According to BBC, "Worldwide, the UN estimates there are more than 50 million regular users of morphine diacetate (heroin), cocaine and synthetic drugs."[67]
More than 70,200 Americans died from drug overdoses in 2017.[68] Among these, the sharpest increase occurred among deaths related to fentanyl and synthetic opioids (28,466 deaths).[68] See charts below.
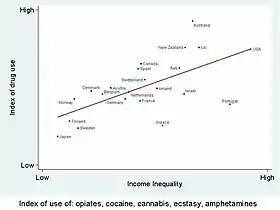 Drug use is higher in countries with high economic inequality
Drug use is higher in countries with high economic inequality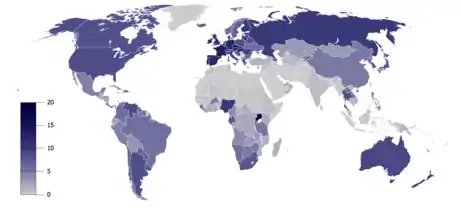 Total recorded alcohol per capita consumption (15+), in litres of pure alcohol[69]
Total recorded alcohol per capita consumption (15+), in litres of pure alcohol[69]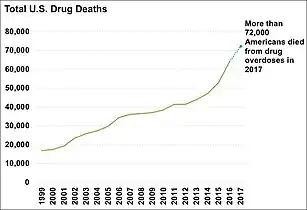 Total yearly U.S. drug deaths.[68]
Total yearly U.S. drug deaths.[68]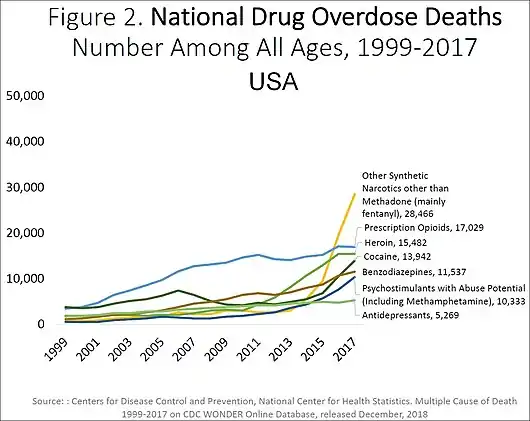 US yearly overdose deaths, and the drugs involved.[68]
US yearly overdose deaths, and the drugs involved.[68]
History
APA, AMA, and NCDA
In 1932, the American Psychiatric Association created a definition that used legality, social acceptability, and cultural familiarity as qualifying factors:
…as a general rule, we reserve the term drug abuse to apply to the illegal, nonmedical use of a limited number of substances, most of them drugs, which have properties of altering the mental state in ways that are considered by social norms and defined by statute to be inappropriate, undesirable, harmful, threatening, or, at minimum, culture-alien.[70]
In 1966, the American Medical Association's Committee on Alcoholism and Addiction defined abuse of stimulants (amphetamines, primarily) in terms of 'medical supervision':
…'use' refers to the proper place of stimulants in medical practice; 'misuse' applies to the physician's role in initiating a potentially dangerous course of therapy; and 'abuse' refers to self-administration of these drugs without medical supervision and particularly in large doses that may lead to psychological dependency, tolerance and abnormal behavior.
In 1973, the National Commission on Marijuana and Drug Abuse stated:
...drug abuse may refer to any type of drug or chemical without regard to its pharmacologic actions. It is an eclectic concept having only one uniform connotation: societal disapproval. ... The Commission believes that the term drug abuse must be deleted from official pronouncements and public policy dialogue. The term has no functional utility and has become no more than an arbitrary codeword for that drug use which is presently considered wrong.[71]
DSM
The first edition of the American Psychiatric Association's Diagnostic and Statistical Manual of Mental Disorders (published in 1952) grouped alcohol and other drug abuse under Sociopathic Personality Disturbances, which were thought to be symptoms of deeper psychological disorders or moral weakness.[72] The third edition, published in 1980, was the first to recognize substance abuse (including drug abuse) and substance dependence as conditions separate from substance abuse alone, bringing in social and cultural factors. The definition of dependence emphasised tolerance to drugs, and withdrawal from them as key components to diagnosis, whereas abuse was defined as "problematic use with social or occupational impairment" but without withdrawal or tolerance.
In 1987, the DSM-IIIR category "psychoactive substance abuse," which includes former concepts of drug abuse is defined as "a maladaptive pattern of use indicated by...continued use despite knowledge of having a persistent or recurrent social, occupational, psychological or physical problem that is caused or exacerbated by the use (or by) recurrent use in situations in which it is physically hazardous." It is a residual category, with dependence taking precedence when applicable. It was the first definition to give equal weight to behavioural and physiological factors in diagnosis. By 1988, the DSM-IV defines substance dependence as "a syndrome involving compulsive use, with or without tolerance and withdrawal"; whereas substance abuse is "problematic use without compulsive use, significant tolerance, or withdrawal." Substance abuse can be harmful to your health and may even be deadly in certain scenarios. By 1994, The fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) issued by the American Psychiatric Association, the DSM-IV-TR, defines substance dependence as "when an individual persists in use of alcohol or other drugs despite problems related to use of the substance, substance dependence may be diagnosed." followed by criteria for the diagnose[73]
DSM-IV-TR defines substance abuse as:[74]
- A. A maladaptive pattern of substance use leading to clinically significant impairment or distress, as manifested by one (or more) of the following, occurring within a 12-month period:
- Recurrent substance use resulting in a failure to fulfill major role obligations at work, school, or home (e.g., repeated absences or poor work performance related to substance use; substance-related absences, suspensions or expulsions from school; neglect of children or household)
- Recurrent substance use in situations in which it is physically hazardous (e.g., driving an automobile or operating a machine when impaired by substance use)
- Recurrent substance-related legal problems (e.g., arrests for substance-related disorderly conduct)
- Continued substance use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of the substance (e.g., arguments with spouse about consequences of intoxication, physical fights)
- B. The symptoms have never met the criteria for Substance Dependence for this class of substance.
The fifth edition of the DSM (DSM-5), was released in 2013, and it revisited this terminology. The principal change was a transition from the abuse/dependence terminology. In the DSM-IV era, abuse was seen as an early form or less hazardous form of the disease characterized with the dependence criteria. However, the APA's 'dependence' term, as noted above, does not mean that physiologic dependence is present but rather means that a disease state is present, one that most would likely refer to as an addicted state. Many involved recognize that the terminology has often led to confusion, both within the medical community and with the general public. The American Psychiatric Association requested input as to how the terminology of this illness should be altered as it moves forward with DSM-5 discussion.[75] In the DSM-5, substance abuse and substance dependence have been merged into the category of substance use disorders and they now longer exist as individual concepts. While substance abuse and dependence were either present or not, substance use disorder has three levels of severity: mild, moderate and severe.[76]
Society and culture
Legal approaches
- Related articles: Drug control law, Prohibition (drugs), Arguments for and against drug prohibition, Harm reduction
Most governments have designed legislation to criminalize certain types of drug use. These drugs are often called "illegal drugs" but generally what is illegal is their unlicensed production, distribution, and possession. These drugs are also called "controlled substances". Even for simple possession, legal punishment can be quite severe (including the death penalty in some countries). Laws vary across countries, and even within them, and have fluctuated widely throughout history.
Attempts by government-sponsored drug control policy to interdict drug supply and eliminate drug abuse have been largely unsuccessful. In spite of the huge efforts by the U.S., drug supply and purity has reached an all-time high, with the vast majority of resources spent on interdiction and law enforcement instead of public health.[77][78] In the United States, the number of nonviolent drug offenders in prison exceeds by 100,000 the total incarcerated population in the EU, despite the fact that the EU has 100 million more citizens.[79]
Despite drug legislation (or perhaps because of it), large, organized criminal drug cartels operate worldwide. Advocates of decriminalization argue that drug prohibition makes drug dealing a lucrative business, leading to much of the associated criminal activity.
Cost
Policymakers try to understand the relative costs of drug-related interventions. An appropriate drug policy relies on the assessment of drug-related public expenditure based on a classification system where costs are properly identified.
Labelled drug-related expenditures are defined as the direct planned spending that reflects the voluntary engagement of the state in the field of illicit drugs. Direct public expenditures explicitly labeled as drug-related can be easily traced back by exhaustively reviewing official accountancy documents such as national budgets and year-end reports. Unlabelled expenditure refers to unplanned spending and is estimated through modeling techniques, based on a top-down budgetary procedure. Starting from overall aggregated expenditures, this procedure estimates the proportion causally attributable to substance abuse (Unlabelled Drug-related Expenditure = Overall Expenditure × Attributable Proportion). For example, to estimate the prison drug-related expenditures in a given country, two elements would be necessary: the overall prison expenditures in the country for a given period, and the attributable proportion of inmates due to drug-related issues. The product of the two will give a rough estimate that can be compared across different countries.[80]
Europe
As part of the reporting exercise corresponding to 2005, the European Monitoring Centre for Drugs and Drug Addiction's network of national focal points set up in the 27 European Union (EU) Member States, Norway, and the candidates countries to the EU, were requested to identify labeled drug-related public expenditure, at the country level.[80]
This was reported by 10 countries categorized according to the functions of government, amounting to a total of EUR 2.17 billion. Overall, the highest proportion of this total came within the government functions of Health (66%) (e.g. medical services), and Public Order and Safety (POS) (20%) (e.g. police services, law courts, prisons). By country, the average share of GDP was 0.023% for Health, and 0.013% for POS. However, these shares varied considerably across countries, ranging from 0.00033% in Slovakia, up to 0.053% of GDP in Ireland in the case of Health, and from 0.003% in Portugal, to 0.02% in the UK, in the case of POS; almost a 161-fold difference between the highest and the lowest countries for Health, and a 6-fold difference for POS. Why do Ireland and the UK spend so much in Health and POS, or Slovakia and Portugal so little, in GDP terms?
To respond to this question and to make a comprehensive assessment of drug-related public expenditure across countries, this study compared Health and POS spending and GDP in the 10 reporting countries. Results found suggest GDP to be a major determinant of the Health and POS drug-related public expenditures of a country. Labelled drug-related public expenditure showed a positive association with the GDP across the countries considered: r = 0.81 in the case of Health, and r = 0.91 for POS. The percentage change in Health and POS expenditures due to a one percent increase in GDP (the income elasticity of demand) was estimated to be 1.78% and 1.23% respectively.
Being highly income elastic, Health and POS expenditures can be considered luxury goods; as a nation becomes wealthier it openly spends proportionately more on drug-related health and public order and safety interventions.[80]
United Kingdom
The UK Home Office estimated that the social and economic cost of drug abuse[81] to the UK economy in terms of crime, absenteeism and sickness is in excess of £20 billion a year.[82] However, the UK Home Office does not estimate what portion of those crimes are unintended consequences of drug prohibition (crimes to sustain expensive drug consumption, risky production and dangerous distribution), nor what is the cost of enforcement. Those aspects are necessary for a full analysis of the economics of prohibition.[83]
United States
| Year | Cost (billions of dollars)[84] |
|---|---|
| 1992 | 107 |
| 1993 | 111 |
| 1994 | 117 |
| 1995 | 125 |
| 1996 | 130 |
| 1997 | 134 |
| 1998 | 140 |
| 1999 | 151 |
| 2000 | 161 |
| 2001 | 170 |
| 2002 | 181 |
These figures represent overall economic costs, which can be divided in three major components: health costs, productivity losses and non-health direct expenditures.
- Health-related costs were projected to total $16 billion in 2002.
- Productivity losses were estimated at $128.6 billion. In contrast to the other costs of drug abuse (which involve direct expenditures for goods and services), this value reflects a loss of potential resources: work in the labor market and in household production that was never performed, but could reasonably be expected to have been performed absent the impact of drug abuse.
- Included are estimated productivity losses due to premature death ($24.6 billion), drug abuse-related illness ($33.4 billion), incarceration ($39.0 billion), crime careers ($27.6 billion) and productivity losses of victims of crime ($1.8 billion).
- The non-health direct expenditures primarily concern costs associated with the criminal justice system and crime victim costs, but also include a modest level of expenses for administration of the social welfare system. The total for 2002 was estimated at $36.4 billion. The largest detailed component of these costs is for state and federal corrections at $14.2 billion, which is primarily for the operation of prisons. Another $9.8 billion was spent on state and local police protection, followed by $6.2 billion for federal supply reduction initiatives.
According to a report from the Agency for Healthcare Research and Quality (AHRQ), Medicaid was billed for a significantly higher number of hospitals stays for Opioid drug overuse than Medicare or private insurance in 1993. By 2012, the differences were diminished. Over the same time, Medicare had the most rapid growth in number of hospital stays.[85]
Special populations
Immigrants and refugees
Immigrant and refugees have often been under great stress,[86] physical trauma and depression and anxiety due to separation from loved ones often characterize the pre-migration and transit phases, followed by "cultural dissonance," language barriers, racism, discrimination, economic adversity, overcrowding, social isolation, and loss of status and difficulty obtaining work and fears of deportation are common. Refugees frequently experience concerns about the health and safety of loved ones left behind and uncertainty regarding the possibility of returning to their country of origin.[87][88] For some, substance abuse functions as a coping mechanism to attempt to deal with these stressors.[88]
Immigrants and refugees may bring the substance use and abuse patterns and behaviors of their country of origin,[88] or adopt the attitudes, behaviors, and norms regarding substance use and abuse that exist within the dominant culture into which they are entering.[88][89]
Street children
Street children in many developing countries are a high risk group for substance misuse, in particular solvent abuse.[90] Drawing on research in Kenya, Cottrell-Boyce argues that "drug use amongst street children is primarily functional – dulling the senses against the hardships of life on the street – but can also provide a link to the support structure of the ‘street family’ peer group as a potent symbol of shared experience."[91]
Musicians
In order to maintain high-quality performance, some musicians take chemical substances.[92] Some musicians take drugs such as alcohol to deal with the stress of performing. As a group they have a higher rate of substance abuse.[92] The most common chemical substance which is abused by pop musicians is cocaine,[92] because of its neurological effects. Stimulants like cocaine increase alertness and cause feelings of euphoria, and can therefore make the performer feel as though they in some ways ‘own the stage’. One way in which substance abuse is harmful for a performer (musicians especially) is if the substance being abused is aspirated. The lungs are an important organ used by singers, and addiction to cigarettes may seriously harm the quality of their performance.[92] Smoking causes harm to alveoli, which are responsible for absorbing oxygen.
Veterans
Substance abuse can be another contributing factor that affects physical and mental health of veterans. Substance abuse may also damage personal relationships families and lead to financial difficulty. There is evidence to suggest that substance abuse disproportionately affects the homeless veteran population. A 2015 Florida study compared causes of homelessness between veterans and non veteran populations in a self reporting questionnaire. The results from the study found that 17.8% of the homeless veteran participants attributed their homelessness to alcohol and other drug related problems compared to just 3.7% of the non-veteran homeless group.[93]
A 2003 study found that homelessness was associated with access to support from family/friends and services. However, this relationship was not true when comparing homeless participants who had a current substance-use disorders.[94] The U.S. Department of Veterans Affairs provide a summary of treatment options for veterans with substance use disorder. For treatments that do not involve medication, they offer a therapeutic options that focused on finding outside support groups and “looking at how substance use problems may relate to other problems such as PTSD and depression”.[95]
Sex and gender
There are many sex differences in substance abuse.[96][97][98] Men and Women express differences in the short and long-term effects of substance abuse. These differences can be credited to sexual dimorphisms in brain, endocrine and metabolic systems. Social and environmental factors that tend to disproportionately effect women; such as child and elder care and the risk of exposure to violence are also factors in the gender differences in substance abuse.[96] Women report having greater impairment in areas such as employment, family and social functioning when abusing substances but have a similar response to treatment. Co-occurring psychiatric disorders are more common among women than men who abuse substances; women more frequently use substances to reduce the negative effects of these co-occurring disorders. Substance abuse puts both men and women at higher risk for perpetration and victimization of sexual violence.[96] Men tend to take drugs for the first time to be part of a group and fit in more so than women. At first interaction, women may experience more pleasure from drugs than men do. Women tend to progress more rapidly from first experience to addiction than men.[97] Physicians, psychiatrists and social workers have believed for decades that women escalate alcohol use more rapidly once they start. Once the addictive behavior is established for women they stabilize at higher doses of drugs than males do. When withdrawing from smoking women experience greater stress response. Males experience greater symptoms when withdrawing from alcohol.[97] There are even gender differences when it comes to rehabilitation and relapse rates. For alcohol, relapse rates were very similar for men and women. For women, marriage and marital stress were risk factors for alcohol relapse. For men, being married lowered the risk of relapse.[98] This difference may be a result of gendered differences in excessive drinking. Alcoholic women are much more likely to be married to partners that drink excessively than are alcoholic men. As a result of this, men may be protected from relapse by marriage while women are out at higher risk when married. However, women are less likely than men to experience relapse to substance use. When men experience a relapse to substance use, they more than likely had a positive experience prior to the relapse. On the other hand, when women relapse to substance use, they were more than likely affected by negative circumstances or interpersonal problems.[98]
See also
- ΔFosB
- Addictive personality
- Alcohol abuse
- Combined drug intoxication
- Controlled Substances Act
- Drug addiction
- Drug overdose
- List of controlled drugs in the United Kingdom
- List of deaths from drug overdose and intoxication
- Harm reduction
- Low-threshold treatment programs
- Needle-exchange programme
- Poly drug use
- Polysubstance abuse
- Responsible drug use
- Supervised injection site
References
- "World Drug Report 2012" (PDF). UNITED NATIONS. Retrieved 27 September 2016.
- "EMCDDA | Information on the high-risk drug use (HRDU) (formerly 'problem drug use' (PDU)) key indicator". emcdda.europa.eu. Retrieved 2016-09-27.
- GBD 2015 Mortality and Causes of Death, Collaborators. (8 October 2016). "Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015". Lancet. 388 (10053): 1459–1544. doi:10.1016/S0140-6736(16)31012-1. PMC 5388903. PMID 27733281.
- Ksir, Oakley Ray; Charles (2002). Drugs, society, and human behavior (9th ed.). Boston [u.a.]: McGraw-Hill. ISBN 978-0072319637.
- (2002). Mosby's Medical, Nursing & Allied Health Dictionary. Sixth Edition. Drug abuse definition, p. 552. Nursing diagnoses, p. 2109. ISBN 0-323-01430-5.
- "Addiction is a Chronic Disease". Archived from the original on 24 June 2014. Retrieved 2 July 2014.
- GBD 2013 Mortality and Causes of Death, Collaborators (17 December 2014). "Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013". Lancet. 385 (9963): 117–71. doi:10.1016/S0140-6736(14)61682-2. PMC 4340604. PMID 25530442.
- "A Public Health Approach" (PDF). Retrieved 1 April 2017.
- Nutt, David J; King, Leslie A; Phillips, Lawrence D (November 2010). "Drug harms in the UK: a multicriteria decision analysis". The Lancet. 376 (9752): 1558–1565. CiteSeerX 10.1.1.690.1283. doi:10.1016/S0140-6736(10)61462-6. PMID 21036393. S2CID 5667719.
- E. Fehrman, A. K. Muhammad, E. M. Mirkes, V. Egan, A. N. Gorban,The Five Factor Model of personality and evaluation of drug consumption risk, arXiv:1506.06297 [stat.AP], 2015
- Philip Jenkins, Synthetic panics: the symbolic politics of designer drugs, NYU Press, 1999, ISBN 0-8147-4244-0, pp. ix–x
- Fehrman, Elaine; Egan, Vincent; Gorban, Alexander N.; Levesley, Jeremy; Mirkes, Evgeny M.; Muhammad, Awaz K. (2019). Personality Traits and Drug Consumption. A Story Told by Data. Springer, Cham. arXiv:2001.06520. doi:10.1007/978-3-030-10442-9. ISBN 978-3-030-10441-2. S2CID 151160405.
- Barrett SP, Meisner JR, Stewart SH (November 2008). "What constitutes prescription drug misuse? Problems and pitfalls of current conceptualizations" (PDF). Curr Drug Abuse Rev. 1 (3): 255–62. doi:10.2174/1874473710801030255. PMID 19630724. Archived from the original (PDF) on 2010-06-15.
- McCabe SE, Boyd CJ, Teter CJ (June 2009). "Subtypes of nonmedical prescription drug misuse". Drug Alcohol Depend. 102 (1–3): 63–70. doi:10.1016/j.drugalcdep.2009.01.007. PMC 2975029. PMID 19278795.
- Antai-Otong, D. 2008. Psychiatric Nursing: Biological and Behavioral Concepts. 2nd edition. Canada: Thompson Delmar Learning
- "The Prescription Drug Abuse Epidemic". PDMP Center of Excellence. 2010–2013.
- "Topics in Brief: Prescription Drug Abuse" NIDA, December 2011.
- "Vaping popular among teens; opioid misuse at historic lows". National Institute on Drug Abuse. 14 December 2017. Retrieved 10 April 2019.
- "Combating Prescription Drug Abuse in Your Practice" Archived 2012-06-18 at the Wayback Machine Aubrey Westgate, Physicians Practice, June 2012.
- Nutt, D.; King, L. A.; Saulsbury, W.; Blakemore, C. (2007). "Development of a rational scale to assess the harm of drugs of potential misuse". The Lancet. 369 (9566): 1047–1053. doi:10.1016/S0140-6736(07)60464-4. PMID 17382831. S2CID 5903121.
- Burke PJ, O'Sullivan J, Vaughan BL (November 2005). "Adolescent substance use: brief interventions by emergency care providers". Pediatr Emerg Care. 21 (11): 770–6. doi:10.1097/01.pec.0000186435.66838.b3. PMID 16280955. S2CID 36410538.
- Serafini G, Innamorati M, Dominici G, Ferracuti S, Kotzalidis GD, Serra G (April 2010). "Suicidal Behavior and Alcohol Abuse". International Journal of Environmental Research and Public Health. International Journal Environmental Research and Public Health. 7 (4): 1392–1431. doi:10.3390/ijerph7041392. PMC 2872355. PMID 20617037.
- O'Connor, Rory; Sheehy, Noel (29 January 2000). Understanding suicidal behaviour. Leicester: BPS Books. pp. 33–36. ISBN 978-1-85433-290-5.
- Isralowitz, Richard (2004). Drug use: a reference handbook. Santa Barbara, Calif.: ABC-CLIO. pp. 122–123. ISBN 978-1-57607-708-5.
- University of Miami: Substance Abuse, Substance Abuse and Health Risks
- "High-strength skunk 'now dominates' UK cannabis market". nhs.uk. 28 February 2018.
- Di Forti M, Marconi A, Carra E, Fraietta S, Trotta A, Bonomo M, Bianconi F, Gardner-Sood P, O'Connor J, Russo M, Stilo SA, Marques TR, Mondelli V, Dazzan P, Pariante C, David AS, Gaughran F, Atakan Z, Iyegbe C, Powell J, Morgan C, Lynskey M, Murray RM (2015). "Proportion of patients in south London with first-episode psychosis attributable to use of high potency cannabis: a case-control study" (PDF). Lancet Psychiatry. 2 (3): 233–8. doi:10.1016/S2215-0366(14)00117-5. PMID 26359901.
- Marta Di Forti (17 December 2013). "Daily Use, Especially of High-Potency Cannabis, Drives the Earlier Onset of Psychosis in Cannabis Users". Schizophrenia Bulletin. 40 (6): 1509–1517. doi:10.1093/schbul/sbt181. PMC 4193693. PMID 24345517.
- Evans, Katie; Sullivan, Michael J. (1 March 2001). Dual Diagnosis: Counseling the Mentally Ill Substance Abuser (2nd ed.). Guilford Press. pp. 75–76. ISBN 978-1-57230-446-8.
- Hampton WH, Hanik I, Olson IR (2019). "[Substance Abuse and White Matter: Findings, Limitations, and Future of Diffusion Tensor Imaging Research]". Drug and Alcohol Dependence. 197 (4): 288–298. doi:10.1016/j.drugalcdep.2019.02.005. PMC 6440853. PMID 30875650.
Given that our the central nervous system is an intricately balanced, complex network of billions of neurons and supporting cells, some might imagine that extrinsic substances could cause irreversible brain damage. Our review paints a less gloomy picture of the substances reviewed, however. Following prolonged abstinence, abusers of alcohol (Pfefferbaum et al., 2014) or opiates (Wang et al., 2011) have white matter microstructure that is not significantly different from non-users. There was also no evidence that the white matter microstructural changes observed in longitudinal studies of cannabis, nicotine, or cocaine were completely irreparable. It is therefore possible that, at least to some degree, abstinence can reverse effects of substance abuse on white matter. The ability of white matter to “bounce back” very likely depends on the level and duration of abuse, as well as the substance being abused.
- "Impulsivity". The Free Dictionary.
- Gerard Moeller M.D., Barratt Ernest S., Ph, Dougherty Donald M., Ph, Schmitz Joy M., Ph, Swann Alan C. (2001). "Psychiatric Aspects of Impulsivity". The American Journal of Psychiatry. 158 (11): 1783–93. doi:10.1176/appi.ajp.158.11.1783. PMID 11691682. Archived from the original on April 15, 2013.CS1 maint: multiple names: authors list (link)
- Bishara AJ, Pleskac TJ, Fridberg DJ, Yechiam E, Lucas J, Busemeyer JR, Finn PR, Stout JC (2009). "Similar Processes Despite Divergent Behavior in Two Commonly Used Measures of Risky Decision Making". J Behav Decis Mak. 22 (4): 435–454. doi:10.1002/bdm.641. PMC 3152830. PMID 21836771.
- Kreek, Mary Jeanne; Nielsen, David A; Butelman, Eduardo R; LaForge, K Steven (26 October 2005). "Genetic influences on impulsivity, risk taking, stress responsivity and vulnerability to drug abuse and addiction". Nature Neuroscience. 8 (11): 1450–1457. doi:10.1038/nn1583. PMID 16251987. S2CID 12589277.
- Chambers RA, Taylor JR, Potenza MN (2003). "Developmental neurocircuitry of motivation in adolescence: a critical period of addiction vulnerability". Am J Psychiatry. 160 (6): 1041–52. doi:10.1176/appi.ajp.160.6.1041. PMC 2919168. PMID 12777258.
- Jeronimus B.F.; Kotov, R.; Riese, H.; Ormel, J. (2016). "Neuroticism's prospective association with mental disorders halves after adjustment for baseline symptoms and psychiatric history, but the adjusted association hardly decays with time: a meta-analysis on 59 longitudinal/prospective studies with 443 313 participants". Psychological Medicine. 46 (14): 2883–2906. doi:10.1017/S0033291716001653. PMID 27523506.
- Knight JR, Shrier LA, Harris SK, Chang G (2002). "Validity of the CRAFFT substance abuse screening test among adolescent clinic patients". JAMA Pediatrics. 156 (6): 607–614. doi:10.1001/archpedi.156.6.607.
- Dhalla S, Kopec JA (2007). "The CAGE questionnaire for alcohol misuse: a review of reliability and validity studies". Clinical and Investigative Medicine: 33–41. doi:10.25011/cim.v30i1.447.
- Morse, Barbara (1997). Screening for Substance Abuse During Pregnancy: Improving Care, Improving Health (PDF). pp. 4–5. ISBN 978-1-57285-042-2.
- O'Donohue, W; K.E. Ferguson (2006). "Evidence-Based Practice in Psychology and Behavior Analysis". The Behavior Analyst Today. 7 (3): 335–350. doi:10.1037/h0100155. Retrieved 2008-03-24.
- Chambless, D.L.; et al. (1998). "An update on empirically validated therapies" (PDF). Clinical Psychology. 49: 5–14. Retrieved 2008-03-24.
- "NIH Senior Health "Build With You in Mind": Survey". nihseniorhealth.gov. Archived from the original on 2015-08-11. Retrieved 29 July 2015.
- "Association for Behavioral and Cognitive Therapies – What is CBT?". Archived from the original on 2010-04-21.
- "Association for Behavioral and Cognitive Therapies – What is Family Therapy?". Archived from the original on 2010-06-13.
- Hogue, A; Henderson, CE; Ozechowski, TJ; Robbins, MS (2014). "Evidence base on outpatient behavioral treatments for adolescent substance use: updates and recommendations 2007–2013". Journal of Clinical Child and Adolescent Psychology. 43 (5): 695–720. doi:10.1080/15374416.2014.915550. PMID 24926870. S2CID 10036629.
- "Association for Behavioral and Cognitive Therapies – Treatment for Substance Use Disorders". Archived from the original on 2010-04-21.
- Engle, Bretton; Macgowan, Mark J. (2009-08-05). "A Critical Review of Adolescent Substance Abuse Group Treatments". Journal of Evidence-Based Social Work. 6 (3): 217–243. doi:10.1080/15433710802686971. ISSN 1543-3714. PMID 20183675. S2CID 3293758.
- "Maternal substance use and integrated treatment programs for women with substance abuse issues and their children: a meta-analysis". crd.york.ac.uk. Retrieved 2016-03-09.
- Carney, Tara; Myers, Bronwyn J; Louw, Johann; Okwundu, Charles I (2016-01-20). "Brief school-based interventions and behavioural outcomes for substance-using adolescents". Cochrane Database of Systematic Reviews (1): CD008969. doi:10.1002/14651858.cd008969.pub3. hdl:10019.1/104381. PMC 7119449. PMID 26787125.
- Jensen, Chad D.; Cushing, Christopher C.; Aylward, Brandon S.; Craig, James T.; Sorell, Danielle M.; Steele, Ric G. (2011). "Effectiveness of motivational interviewing interventions for adolescent substance use behavior change: A meta-analytic review". Journal of Consulting and Clinical Psychology. 79 (4): 433–440. doi:10.1037/a0023992. PMID 21728400. S2CID 19892519.
- Barnett, Elizabeth; Sussman, Steve; Smith, Caitlin; Rohrbach, Louise A.; Spruijt-Metz, Donna (2012). "Motivational Interviewing for adolescent substance use: A review of the literature". Addictive Behaviors. 37 (12): 1325–1334. doi:10.1016/j.addbeh.2012.07.001. PMC 3496394. PMID 22958865.
- "Self-Help Groups Article". Retrieved May 27, 2015.
- Uekermann J, Daum I (May 2008). "Social cognition in alcoholism: a link to prefrontal cortex dysfunction?". Addiction. 103 (5): 726–35. doi:10.1111/j.1360-0443.2008.02157.x. PMID 18412750.
- Purvis G.; MacInnis D. M. (2009). "Implementation of the Community Reinforcement Approach (CRA) in a Long-Standing Addictions Outpatient Clinic" (PDF). Journal of Behavior Analysis of Sports, Health, Fitness and Behavioral Medicine. 2: 133–44. Archived from the original (PDF) on 2010-12-29.
- "Current Pharmacological Treatment Available for Alchhol Abuse". The California Evidence-Based Clearinghouse. 2006–2013.
- James W. Kalat Biological psychology 11th edition pg.78
- Maglione, M; Maher, AR; Hu, J; Wang, Z; Shanman, R; Shekelle, PG; Roth, B; Hilton, L; Suttorp, MJ; Ewing, BA; Motala, A; Perry, T (September 2011). "Off-Label Use of Atypical Antipsychotics: An Update [Internet]". Agency for Healthcare Research and Quality (US). PMID 22132426. Report No.: 11-EHC087-EF.
- Lingford-Hughes AR, Welch S, Peters L, Nutt DJ, British Association for Psychopharmacology, Expert Reviewers Group (2012-07-01). "BAP updated guidelines: evidence-based guidelines for the pharmacological management of substance abuse, harmful use, addiction and comorbidity: recommendations from BAP". Journal of Psychopharmacology. 26 (7): 899–952. doi:10.1177/0269881112444324. ISSN 0269-8811. PMID 22628390.
- "Drogentote" Swiss Health Observatory. obsan.admin.ch. Retrieved 23 December 2020.
- "Overdose Death Rates". drugabuse.gov. Retrieved 23 December 2020.
- Lingford-Hughes A. R.; Welch S.; Peters L.; Nutt D. J. (2012). "BAP updated guidelines: evidence-based guidelines for the pharmacological management of substance abuse, harmful use, addiction and comorbidity: recommendations from BAP" (PDF). Journal of Psychopharmacology. 26 (7): 899–952. doi:10.1177/0269881112444324. PMID 22628390. S2CID 30030790. Archived from the original (PDF) on 2012-12-03.
- Peterson Ashley L (2013). "Integrating Mental Health and Addictions Services to Improve Client Outcomes". Issues in Mental Health Nursing. 34 (10): 752–756. doi:10.3109/01612840.2013.809830. PMID 24066651. S2CID 11537206.
- Johnston, L. D., O’Malley, P. M., Bachman, J. G., & Schulenberg, J. E. (2011). Monitoring the Future national results on adolescent drug use: Overview of key findings, 2010. Ann Arbor: Institute for Social Research, The University of Michigan.
- "CDC Newsroom Press Release June 3, 2010".
- Barker, P. ed. 2003. Psychiatric and mental health nursing: the craft and caring. London: Arnold. pp297
- Effective Child Therapy: Substance Abuse and Dependence. Copyright 2012 Archived 2013-05-03 at the Wayback Machine
- "Drug Trade". BBC News.
- Overdose Death Rates. By National Institute on Drug Abuse (NIDA).
- Global Status Report on Alcohol 2004
- Glasscote, R.M., Sussex, J.N., Jaffe, J.H., Ball, J., Brill, L. (1932). The Treatment of Drug Abuse for people like you...: Programs, Problems, Prospects. Washington, D.C.: Joint Information Service of the American Psychiatric Association and the National Association for Mental Health.
- Second Report of the National Commission on Marihuana and Drug Abuse; Drug Use In America: Problem In Perspective (March 1973), p.13
- Transformations: Substance Drug Abuse
- DSM-IV & DSM-IV-TR:Substance Dependence Archived 2011-09-27 at the Wayback Machine
- American Psychiatric Association (1994). Diagnostic and statistical manual of mental disorders (4th edition). Washington, DC.
- Hasin, Deborah S.; O’Brien, Charles P.; Auriacombe, Marc; Borges, Guilherme; Bucholz, Kathleen; Budney, Alan; Compton, Wilson M.; Crowley, Thomas; Ling, Walter (2013-08-01). "DSM-5 Criteria for Substance Use Disorders: Recommendations and Rationale". American Journal of Psychiatry. 170 (8): 834–851. doi:10.1176/appi.ajp.2013.12060782. ISSN 0002-953X. PMC 3767415. PMID 23903334.
- "Diagnostic and Statistical Manual of Mental Disorders: DSM-5 (5th edition)2014 102 Washington, DC American Psychiatric Association 2013 xliv+947 pp. 9780890425541(hbck);9780890425558(pbck) £175 $199 (hbcchvk); £45 $69 (pbck)". Reference Reviews. 28 (3): 36–37. 11 March 2014. doi:10.1108/rr-10-2013-0256.
- Copeman M (April 2003). "Drug supply and drug abuse". CMAJ. 168 (9): 1113, author reply 1113. PMC 153673. PMID 12719309. Archived from the original on 2009-09-06.
- Wood E, Tyndall MW, Spittal PM, et al. (January 2003). "Impact of supply-side policies for control of illicit drugs in the face of the AIDS and overdose epidemics: investigation of a massive heroin seizure". CMAJ. 168 (2): 165–9. PMC 140425. PMID 12538544.
- Bewley-Taylor, Dave, Hallam, Chris, Allen Rob. The Beckley Foundation Drug Policy Programme: The Incarceration of Drug Offenders: An Overview. March 2009.
- Prieto L (2010). "Labelled drug-related public expenditure in relation to gross domestic product (gdp) in Europe: A luxury good?". Substance Abuse Treatment, Prevention, and Policy. 5: 9. doi:10.1186/1747-597x-5-9. PMC 2881082. PMID 20478069.
- "NHS and Drug Abuse". National Health Service (NHS). March 22, 2010. Retrieved March 22, 2010.
- "Home Office | Tackling Drugs Changing Lives | Drugs in the workplace". 2007-06-09. Archived from the original on 2007-06-09. Retrieved 2016-09-19.
- Thornton, Mark. "The Economics of Prohibition".
- The economic costs of drug abuse in the United States
- Owens PL, Barrett ML, Weiss AJ, Washington RE, Kronick R (August 2014). "Hospital Inpatient Utilization Related to Opioid Overuse Among Adults, 1993–2012". HCUP Statistical Brief #177. Rockville, MD: Agency for Healthcare Research and Quality.
- Drachman, D. (1992). "A stage-of-migration framework for service to immigrant populations". Social Work. 37 (1): 68–72. doi:10.1093/sw/37.1.68.
- Pumariega A. J.; Rothe E.; Pumariega J. B. (2005). "Mental health of immigrants and refugees". Community Mental Health Journal. 41 (5): 581–597. CiteSeerX 10.1.1.468.6034. doi:10.1007/s10597-005-6363-1. PMID 16142540. S2CID 7326036.
- National Institute on Alcohol Abuse and Alcoholism. (2005). Module 10F: Immigrants, refugees, and alcohol. In NIAAA: Social work education for the prevention and treatment of alcohol use disorders (NIH publication). Washington, D.C.
- Caetano R.; Clark C. L.; Tam T. (1998). "Alcohol consumption among racial/ethnic minorities: Theory and research". Journal of Alcohol, Health, and Research. 22 (4): 233–241.
- UNODC. "Understanding Substance Use Among Street Children" (PDF). Retrieved 30 January 2014.
- Cottrell-Boyce, Joe (2010). "The role of solvents in the lives of Kenyan street children: An ethnographic perspective" (PDF). African Journal of Drug & Alcohol Studies. 9 (2): 93–102. doi:10.4314/ajdas.v9i2.64142. Retrieved 28 January 2014.
- Breitenfeld D.; Thaller V.; Perić B.; Jagetic N.; Hadžić D.; Breitenfeld T. (2008). "Substance abuse in performing musicians". Alcoholism: Journal on Alcoholism and Related Addictions. 44 (1): 37–42. ProQuest 622145760.
- Dunne, E. M., Burrell, L. I., Diggins, A. D., Whitehead, N. E., & Latimer, W. W. (2015). "Increased risk for substance use and health‐related problems among homeless veterans". The American Journal on Addictions. 24 (7): 676–680. doi:10.1111/ajad.12289. PMC 6941432. PMID 26359444.CS1 maint: multiple names: authors list (link)
- Zlotnick, C., Tam, T., & Robertson, M. J. (2003). "Disaffiliation, substance use, and exiting homelessness". Substance Use & Misuse. 38 (3–6): 577–599. doi:10.1081/ja-120017386. PMID 12747398. S2CID 31815225.CS1 maint: multiple names: authors list (link)
- "Treatment Programs for Substance Use Problems – Mental Health". mentalhealth.va.gov. Retrieved 2016-12-17.
- McHugh, R. Kathryn; Votaw, Victoria R.; Sugarman, Dawn E.; Greenfield, Shelly F. (2018-12-01). "Sex and gender differences in substance use disorders". Clinical Psychology Review. Gender and Mental Health. 66: 12–23. doi:10.1016/j.cpr.2017.10.012. ISSN 0272-7358. PMC 5945349. PMID 29174306.
- Becker, Jill B.; McClellan, Michele L.; Reed, Beth Glover (2016-11-07). "Sex differences, gender and addiction". Journal of Neuroscience Research. 95 (1–2): 136–147. doi:10.1002/jnr.23963. ISSN 0360-4012. PMC 5120656. PMID 27870394.
- Walitzer, Kimberly S.; Dearing, Ronda L. (2006-03-01). "Gender differences in alcohol and substance use relapse". Clinical Psychology Review. Relapse in the addictive behaviors. 26 (2): 128–148. doi:10.1016/j.cpr.2005.11.003. ISSN 0272-7358. PMID 16412541.
External links
| Classification | |
|---|---|
| External resources |
| Wikimedia Commons has media related to Substance abuse. |
- Substance abuse at Curlie
- Adverse Childhood Experiences: Risk Factors for Substance Misuse and Mental Health Dr. Robert Anda of the U.S. Centers for Disease Control describes the relation between childhood adversity and later ill-health, including substance abuse (video)
- The National Institute on Drug Abuse
| General | 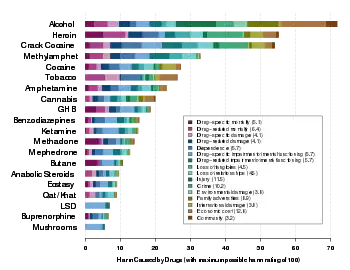 | ||||
|---|---|---|---|---|---|
| Combined substance use |
| ||||
| Alcohol |
| ||||
| Caffeine | |||||
| Cannabis |
| ||||
| Cocaine |
| ||||
| Hallucinogen | |||||
| Nicotine | |||||
| Opioids |
| ||||
| Sedative / hypnotic | |||||
| Stimulants | |||||
| Volatile solvent |
| ||||