Soluble fms-like tyrosine kinase-1
Soluble fms-like tyrosine kinase-1 (sFlt-1 or sVEGFR-1) is a tyrosine kinase protein with antiangiogenic properties. A non-membrane associated splice variant of VEGF receptor 1 (Flt-1), sFlt-1 binds the angiogenic factors VEGF (vascular endothelial growth factor) and PlGF (placental growth factor), reducing blood vessel growth through reduction of free VEGF and PlGF concentrations.[1] In humans, sFlt-1 is important in the regulation of blood vessel formation in diverse tissues, including the kidneys, cornea, and uterus.[2][3] Abnormally high levels of sFlt-1 have been implicated in the pathogenesis of preeclampsia.[4]
Structure
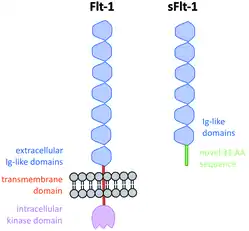
sFlt-1 is a truncated form of the VEGF receptor Flt-1. Though sFlt-1 contains an extracellular domain identical to that of Flt-1, it lacks both the transmembrane and intercellular domains present in Flt-1. Instead, sFlt-1 contains a novel 31 amino acid C-terminal sequence.[5] sFlt-1 is composed of 6 immunoglobulin-like domains, with a binding site for VEGF and PIGF within the second domain from the N-terminus.[6] A sequence of 10 basic amino acids form a binding site for the anticoagulant heparin in the third domain from the N-terminus.[7] sFlt-1 has a pI of 9.51, giving the protein a positive charge at physiological pH.[8]
Biological function

Because sFlt-1 lacks the transmembrane domain that typically embeds tyrosine kinase receptors in the cell membrane, sFlt-1 travels freely in the blood circulation, and thus can travel from the tissue in which it is originally secreted to other areas of the body.[5] As it contains the same extracellular domain as Flt-1, sFlt-1 competes with Flt-1 to bind VEGF and PIGF, effectively reducing serum concentrations of these two angiogenic growth factors.[4] Though sFlt-1 can effectively dimerize, its lack of a kinase domain means that no tyrosine phosphorylation occurs upon ligand binding.[8] As a result, sFIt-1 effectively sequesters agonists of FIt-1, and has been implicated as a regulator of this receptor in the kidney, liver, and brain.[9]
Role in preeclampsia
The placental factor theory of preeclampsia
Preeclampsia is a pregnancy-specific condition characterized by maternal hypertension and proteinuria after the 20th week of gestation.[5] Normally, during early formation of the placenta, extravillous cytotrophoblasts, a type of specialized fetal cell, enter the spiral arteries of the uterus. This invasion spurs remodeling of the epithelial layer of these uterine arteries, increasing their conductance and decreasing their resistance to meet the increase blood flow demands of pregnancy.[10][11] Specifically, invading cytotrophoblasts achieve this change by down-regulating the expression of adhesion molecules characteristic of epithelial cells and up-regulating the expression of adhesion molecules characteristic of endothelial cells in a process known as pseudovasculogenesis.[12][13]
In preeclamptic patients, this arterial transformation is incomplete, as cytotrophoblasts fail to completely switch their adhesion molecule expression pattern to an endothelial form. The balance of pro- and anti-angiogenic factors and their receptors, including VEGF-A, PIGF, Flt1, and sFlt1, is thought to mediate this process.[5]
In women who develop preeclampsia, the sFlt-1 to PlGF ratio is higher than in normal pregnancy.[4][14][6] sFlt-1 produced in the placenta is thought to circulate in the maternal bloodstream to act on distant tissues, explaining the multi-system endothelial dysfunction observed in women with preeclampsia.[5] In-vitro studies have linked sFlt-1 treatment to a pattern of vasoconstriction and endothelial dysfunction identical to the syndrome produced when cells are incubated with serum from preeclamptic patients.[5] Additionally, adenoviral transfer of the sFlt-1 gene to pregnant rats has been shown to produce a syndrome similar to preeclampsia.[5]
Preeclamptic regulation of sFlt-1
Though sFlt-1 is produced in small amounts by endothelial cells and monocytes, the placenta is theorized to be the major source of sFlt-1 during pregnancy.[4] sFlt-1 mRNA shows strong expression in the placenta, and serum concentration of sFlt-1 falls significantly in patients after delivery of the placenta.[15][16]
Expression of sFlt-1 is stimulated by hypoxic conditions. In healthy pregnancies, the placenta develops in a hypoxic environment, leading to a 20-fold increase in sFlt-1 expression.[17] In early-onset preeclamptic patients, this increase is estimated to be up to 43 times more pronounced, and may be spurred by conditions of poor uterine profusion leading to more severe local hypoxia.[18] Inhibition of nitric oxide signaling has also been associated with elevation of serum sFlt-1 in a rat model of preeclampsia; this stimulus may represent a secondary factor contributing to sFlt-1 trends in human preeclampsia as well.[19]
In addition to short-term regulation by oxygen and nitric oxide levels, genetic differences also influence Flt-1 gene splicing and resulting sFlt-1 expression levels. Women with histories of preeclampsia continue to show elevated serum levels of sFlt-1 up to 18 months postpartum, suggesting a genetic basis of sFlt-1 expression independent of pregnancy-related stimuli.[20]
Clinical significance
PlGF and sFlt-1 concentrations measured by immunoassay in maternal blood improve the prognostic possibilities in preeclampsia, which is typically diagnosed solely on the basis of clinical symptoms, proteinuria, and uterine artery Doppler velocimetry.[21][22] Notably, increases in sFlt-1 and decreases in PIGF and VEGF can be detected at least five weeks before the onset of preeclamptic symptoms, potentially facilitating earlier diagnosis and treatment.[23] sFlt-1 changes are most predictive of early-onset preeclampsia; cases of preeclampsia incident late in pregnancy typically are accompanied only by small decreases in PIGF.[18] However, sFlt-1 elevation is also associated with other obstetric conditions such as non-preeclampsic interuterine growth retardation of the fetus, limiting its use as a discriminatory biomarker for preeclampsia.[24] Additionally, sensitivity and specificity of sFlt-1 testing is generally considered too low to enable it to serve as an effective predictor of preeclampsia.[25]
sFlt-1 involvement in the pathogenesis of preeclampsia may explain several demographic trends in incidence of the condition. The human Flt-1/sFlt-1 gene is located at 13q12; the association of fetal trisomy-13 with higher rates of preeclampsia could theoretically be explained by the additional copy of the gene.[5] Additionally, primiparous women have higher baseline levels of sFlt-1, a trend which could potentially explain the higher incidence of preeclampsia among first-time mothers.[5]
Citations
- Khalil A, Muttukrishna S, Harrington K, Jauniaux E (July 2008). "Effect of antihypertensive therapy with alpha methyldopa on levels of angiogenic factors in pregnancies with hypertensive disorders". PLOS One. 3 (7): e2766. doi:10.1371/journal.pone.0002766. PMC 2447877. PMID 18648513.
- Ambati BK, Nozaki M, Singh N, Takeda A, Jani PD, Suthar T, Albuquerque RJ, Richter E, Sakurai E, Newcomb MT, Kleinman ME, Caldwell RB, Lin Q, Ogura Y, Orecchia A, Samuelson DA, Agnew DW, St Leger J, Green WR, Mahasreshti PJ, Curiel DT, Kwan D, Marsh H, Ikeda S, Leiper LJ, Collinson JM, Bogdanovich S, Khurana TS, Shibuya M, Baldwin ME, Ferrara N, Gerber HP, De Falco S, Witta J, Baffi JZ, Raisler BJ, Ambati J (October 2006). "Corneal avascularity is due to soluble VEGF receptor-1". Nature. 443 (7114): 993–7. doi:10.1038/nature05249. PMC 2656128. PMID 17051153.
- Luft FC (February 2014). "Soluble fms-like tyrosine kinase-1 and atherosclerosis in chronic kidney disease". Kidney International. 85 (2): 238–40. doi:10.1038/ki.2013.402. PMID 24487364.
- Maynard SE, Min JY, Merchan J, Lim KH, Li J, Mondal S, Libermann TA, Morgan JP, Sellke FW, Stillman IE, Epstein FH, Sukhatme VP, Karumanchi SA (March 2003). "Excess placental soluble fms-like tyrosine kinase 1 (sFlt1) may contribute to endothelial dysfunction, hypertension, and proteinuria in preeclampsia". The Journal of Clinical Investigation. 111 (5): 649–58. doi:10.1172/JCI200317189. PMC 151901. PMID 12618519.
- Maynard SE, Venkatesha S, Thadhani R, Karumanchi SA (May 2005). "Soluble Fms-like tyrosine kinase 1 and endothelial dysfunction in the pathogenesis of preeclampsia". Pediatric Research. 57 (5 Pt 2): 1R–7R. doi:10.1203/01.PDR.0000159567.85157.B7. PMID 15817508.
- Kendall RL, Thomas KA (November 1993). "Inhibition of vascular endothelial cell growth factor activity by an endogenously encoded soluble receptor". Proceedings of the National Academy of Sciences of the United States of America. 90 (22): 10705–9. doi:10.1073/pnas.90.22.10705. PMC 47846. PMID 8248162.
- Holash J, Davis S, Papadopoulos N, Croll SD, Ho L, Russell M, Boland P, Leidich R, Hylton D, Burova E, Ioffe E, Huang T, Radziejewski C, Bailey K, Fandl JP, Daly T, Wiegand SJ, Yancopoulos GD, Rudge JS (August 2002). "VEGF-Trap: a VEGF blocker with potent antitumor effects". Proceedings of the National Academy of Sciences of the United States of America. 99 (17): 11393–8. doi:10.1073/pnas.172398299. PMC 123267. PMID 12177445.
- Thadhani R, Kisner T, Hagmann H, Bossung V, Noack S, Schaarschmidt W, Jank A, Kribs A, Cornely OA, Kreyssig C, Hemphill L, Rigby AC, Khedkar S, Lindner TH, Mallmann P, Stepan H, Karumanchi SA, Benzing T (August 2011). "Pilot study of extracorporeal removal of soluble fms-like tyrosine kinase 1 in preeclampsia". Circulation. 124 (8): 940–50. doi:10.1161/CIRCULATIONAHA.111.034793. PMID 21810665.
- Maynard S, Epstein FH, Karumanchi SA (2008). "Preeclampsia and angiogenic imbalance". Annual Review of Medicine. 59: 61–78. doi:10.1146/annurev.med.59.110106.214058. PMID 17937587.
- De Wolf, F.; Wolf-Peeters, C. De; Brosens, I.; Robertson, W.B. (1980-05-01). "The human placental bed: Electron microscopic study of trophoblastic invasion of spiral arteries". American Journal of Obstetrics and Gynecology. 137 (1): 58–70. doi:10.1016/0002-9378(80)90387-7. ISSN 0002-9378. PMID 7369289.
- Brosens IA, Robertson WB, Dixon HG (1972). "The role of the spiral arteries in the pathogenesis of preeclampsia". Obstetrics and Gynecology Annual. 1: 177–91. PMID 4669123.
- Zhou Y, Damsky CH, Chiu K, Roberts JM, Fisher SJ (March 1993). "Preeclampsia is associated with abnormal expression of adhesion molecules by invasive cytotrophoblasts". The Journal of Clinical Investigation. 91 (3): 950–60. doi:10.1172/JCI116316. PMC 288047. PMID 7680671.
- Zhou Y, Fisher SJ, Janatpour M, Genbacev O, Dejana E, Wheelock M, Damsky CH (May 1997). "Human cytotrophoblasts adopt a vascular phenotype as they differentiate. A strategy for successful endovascular invasion?". The Journal of Clinical Investigation. 99 (9): 2139–51. doi:10.1172/JCI119387. PMC 508044. PMID 9151786.
- Levine RJ, Thadhani R, Qian C, Lam C, Lim KH, Yu KF, Blink AL, Sachs BP, Epstein FH, Sibai BM, Sukhatme VP, Karumanchi SA (January 2005). "Urinary placental growth factor and risk of preeclampsia". JAMA. 293 (1): 77–85. doi:10.1001/jama.293.1.77. PMID 15632339.
- Hornig C, Barleon B, Ahmad S, Vuorela P, Ahmed A, Weich HA (April 2000). "Release and complex formation of soluble VEGFR-1 from endothelial cells and biological fluids". Laboratory Investigation; A Journal of Technical Methods and Pathology. 80 (4): 443–54. doi:10.1038/labinvest.3780050. PMID 10780661.
- Koga K, Osuga Y, Yoshino O, Hirota Y, Ruimeng X, Hirata T, Takeda S, Yano T, Tsutsumi O, Taketani Y (May 2003). "Elevated serum soluble vascular endothelial growth factor receptor 1 (sVEGFR-1) levels in women with preeclampsia". The Journal of Clinical Endocrinology and Metabolism. 88 (5): 2348–51. doi:10.1210/jc.2002-021942. PMID 12727995.
- Shibata E, Rajakumar A, Powers RW, Larkin RW, Gilmour C, Bodnar LM, Crombleholme WR, Ness RB, Roberts JM, Hubel CA (August 2005). "Soluble fms-like tyrosine kinase 1 is increased in preeclampsia but not in normotensive pregnancies with small-for-gestational-age neonates: relationship to circulating placental growth factor". The Journal of Clinical Endocrinology and Metabolism. 90 (8): 4895–903. doi:10.1210/jc.2004-1955. PMID 15886253.
- Wikström AK, Larsson A, Eriksson UJ, Nash P, Nordén-Lindeberg S, Olovsson M (June 2007). "Placental growth factor and soluble FMS-like tyrosine kinase-1 in early-onset and late-onset preeclampsia". Obstetrics and Gynecology. 109 (6): 1368–74. doi:10.1097/01.AOG.0000264552.85436.a1. PMID 17540809.
- Bahtiyar MO, Buhimschi C, Ravishankar V, Copel J, Norwitz E, Julien S, Guller S, Buhimschi IA (January 2007). "Contrasting effects of chronic hypoxia and nitric oxide synthase inhibition on circulating angiogenic factors in a rat model of growth restriction". American Journal of Obstetrics and Gynecology. 196 (1): 72.e1–6. doi:10.1016/j.ajog.2006.07.048. PMID 17240241.
- Wolf M, Hubel CA, Lam C, Sampson M, Ecker JL, Ness RB, Rajakumar A, Daftary A, Shakir AS, Seely EW, Roberts JM, Sukhatme VP, Karumanchi SA, Thadhani R (December 2004). "Preeclampsia and future cardiovascular disease: potential role of altered angiogenesis and insulin resistance". The Journal of Clinical Endocrinology and Metabolism. 89 (12): 6239–43. doi:10.1210/jc.2004-0548. PMID 15579783.
- Hirashima C, Ohkuchi A, Arai F, Takahashi K, Suzuki H, Watanabe T, Kario K, Matsubara S, Suzuki M (September 2005). "Establishing reference values for both total soluble Fms-like tyrosine kinase 1 and free placental growth factor in pregnant women". Hypertension Research. 28 (9): 727–32. doi:10.1291/hypres.28.727. PMID 16419645.
- Thadhani R, Mutter WP, Wolf M, Levine RJ, Taylor RN, Sukhatme VP, Ecker J, Karumanchi SA (February 2004). "First trimester placental growth factor and soluble fms-like tyrosine kinase 1 and risk for preeclampsia". The Journal of Clinical Endocrinology and Metabolism. 89 (2): 770–5. doi:10.1210/jc.2003-031244. PMID 14764795.
- Levine RJ, Maynard SE, Qian C, Lim KH, England LJ, Yu KF, Schisterman EF, Thadhani R, Sachs BP, Epstein FH, Sibai BM, Sukhatme VP, Karumanchi SA (February 2004). "Circulating angiogenic factors and the risk of preeclampsia". The New England Journal of Medicine. 350 (7): 672–83. doi:10.1056/NEJMoa031884. PMID 14764923.
- Stepan H, Geide A, Faber R (November 2004). "Soluble fms-like tyrosine kinase 1". The New England Journal of Medicine. 351 (21): 2241–2. doi:10.1056/NEJM200411183512123. PMID 15548791.
- Kleinrouweler CE, Wiegerinck MM, Ris-Stalpers C, Bossuyt PM, van der Post JA, von Dadelszen P, Mol BW, Pajkrt E (June 2012). "Accuracy of circulating placental growth factor, vascular endothelial growth factor, soluble fms-like tyrosine kinase 1 and soluble endoglin in the prediction of pre-eclampsia: a systematic review and meta-analysis". BJOG. 119 (7): 778–87. doi:10.1111/j.1471-0528.2012.03311.x. PMID 22433027.