Ketamine
Ketamine is a medication primarily used for starting and maintaining anesthesia. It induces dissociative anesthesia, a trance-like state providing pain relief, sedation, and amnesia.[19] The distinguishing features of ketamine anesthesia are preserved breathing and airway reflexes, stimulated heart function with increased blood pressure, and moderate bronchodilation.[19] At lower, sub-anesthetic doses, ketamine is a promising agent for pain and treatment-resistant depression.[20] However, the antidepressant action of a single administration of ketamine wanes with time, and the effects of repeated use have not been sufficiently studied.[21][22][23]
Psychiatric side effects are frequent as well as raised blood pressure and nausea. Liver and urinary toxicity are common among regular users of high doses of ketamine for recreational purposes. Ketamine is an NMDA receptor antagonist, and that accounts for most of its actions except the antidepressive effect, the mechanism of which is a matter of much research and debate.
Ketamine was discovered in 1956 and approved for use in the United States in 1970. It was extensively used for surgical anesthesia in the Vietnam War due to its safety.[24] Ketamine is also used as a recreational drug for its hallucinogenic and dissociative effects.[25] Ketamine is on the World Health Organization's List of Essential Medicines.[26] and is available as a generic medication.[27]
Medical uses
Anesthesia
The use of ketamine in anesthesia reflects its characteristics. It is a drug of choice for short-term procedures when the muscle relaxation is not required.[28] The effect of ketamine on the respiratory and circulatory systems is different from that of other anesthetics. It suppresses breathing much less than most other available anesthetics.[29] When used at anesthetic doses, ketamine usually stimulates rather than depresses the circulatory system.[30] Protective airway reflexes are preserved,[31] and it is sometimes possible to administer ketamine anesthesia without protective measures to the airways.[28] Psychotomimetic effects limit the acceptance of ketamine; however, they can be counteracted by administering benzodiazepines or propofol.[32]
Ketamine is frequently used in severely injured people and appears to be safe in this group.[33] It has been widely used for emergency surgery in field conditions in war zones,[34] for example, during the Vietnam War.[35] A 2011 clinical practice guideline supports the use of ketamine as a sedative in emergency medicine, including during physically painful procedures.[19] It is the drug of choice for people in traumatic shock who are at risk of hypotension.[36] Low blood pressure is harmful in people with severe head injury,[37] and ketamine is least likely to cause low blood pressure and often even able to prevent it.[38][39]
Ketamine is an option in children, as the sole anesthetic for minor procedures or as an induction agent followed by neuromuscular blocker and tracheal intubation[34] In particular, children with cyanotic heart disease and neuromuscular disorders are good candidates for ketamine anesthesia.[32]
Due to the bronchodilating properties of ketamine, it can be used for anesthesia in people with asthma, chronic obstructive airway disease, and with severe reactive airway disease including active bronchospasm.[34][32][40]
Pain
Ketamine infusions are used for the acute pain treatment in emergency departments and in the perioperative period in individuals with refractory pain. The doses are lower than those used for anesthesia; they are usually referred to as sub-anesthetic doses. Adjunctive to morphine or on its own, ketamine reduces morphine use, pain level, nausea, and vomiting after surgery. Ketamine is likely to be most beneficial for surgical patients when severe post-operative pain is expected and for opioid-tolerant patients.[41][42]
Ketamine is especially useful in the prehospital setting, due to its effectiveness and low risk of respiratory depression.[43] Ketamine has similar efficacy to opioids in a hospital emergency department setting for management of acute pain and for control of procedural pain.[44] It may also prevent opioid-induced hyperalgesia [45][46] and postanesthetic shivering.[47]
For chronic pain, ketamine is used as an intravenous analgesic, particularly, if the pain is neuropathic.[48] It has the added benefit of counteracting spinal sensitization or wind-up phenomena experienced with chronic pain.[49] In multiple clinical trials, ketamine infusions delivered short-term pain relief in neuropathic pain diagnoses, pain after traumatic spine injury, fibromyalgia, and complex regional pain syndrome (CRPS).[48] However, the 2018 consensus guidelines on chronic pain concluded that, overall, there is only weak evidence in favor of ketamine use in spinal injury pain, moderate evidence in favor of ketamine for CRPS, and weak or no evidence for ketamine in mixed neuropathic pain, fibromyalgia, and cancer pain. In particular, only for CRPS there is evidence of medium to longer term pain relief.[48]
Depression
Ketamine is a robust and rapid-acting antidepressant, albeit its effect is transient.[50] Intravenous ketamine infusion in treatment resistant depression results in improved mood within 4 hours reaching the peak at 24 hours.[20][21] The effect is diminished at 7 days, and most patients relapse within 10 days, although for a significant minority the improvement may last 30 days and longer.[21][22][51][52] The main challenge with ketamine treatment is what to do when the anti-depressive action expires. The maintenance therapy with ketamine (from twice a week to once in two weeks) appears to be a promising option, although the evidence to firmly recommend it is insufficient.[21][22][23] Ketamine may also decrease suicidal thoughts for up to three days after the injection.[53]
Ketamine has not been approved for use as an antidepressant, but the Canadian Network for Mood and Anxiety Treatments recommends it as a third line treatment for depression.[22] One of the enantiomers of ketamine, esketamine, has been approved as a nasal spray for treatment-resistant depression in the United States and elsewhere (see Esketamine#Depression). Intravenous infusion of ketamine has never been directly compared with intranasal esketamine, but a comparative meta-analysis of clinical trials indicates the superiority of intravenous ketamine, which has greater overall response and remission rates, and lower number of dropouts.[54]
Seizures
Ketamine is sometimes used in the treatment of status epilepticus that has failed to adequately respond to standard treatments, although only limited evidence (case studies and no randomized controlled trials) exists in its favor.[55][56]
Contraindications
Main contraindications for ketamine:[48][41]
- Severe cardiovascular disease such as unstable angina or poorly controlled hypertension.
- Increased intracranial or intraocular pressure. Both of these contraindications are controversial.[41]
- Poorly controlled psychosis.
- Severe liver disease such as cirrhosis.
- Pregnancy.
- Active substance use (for serial ketamine injections).
- Age less than 3 months.[10]
Side effects
At anesthetic doses, 10–20% of adults (1–2% of children)[10] experience adverse psychiatric reactions that occur during emergence from anesthesia, ranging from dreams and dysphoria to hallucinations and emergence delirium.[57] These can be counteracted by pretreating with a benzodiazepine or propofol.[57][32] Ketamine anesthesia commonly causes tonic-clonic movements (greater than 10% of people) and rarely hypertonia.[16][57] Vomiting can be expected in 5–15% of the patients; pre-treatment with propofol mitigates it as well.[10][57] Laryngospasm occurs only rarely with ketamine. Ketamine, generally, stimulates breathing; however, in the first 2–3 minutes of a high-dose rapid intravenous injection it may cause a transient respiratory depression.[57]
At lower sub-anesthetic doses, psychiatric side effects are prominent. A majority of patients feel strange, spacey, woozy or floating, or have visual distortions or numbness. Also very frequent (20–50%) are difficulty speaking, confusion, euphoria, drowsiness, and difficulty concentrating. The symptoms of psychosis such as going into a hole, disappearing, feeling melting, experiencing colors and hallucinations are described by 6–10% of people. Dizziness, blurred vision, dry mouth, hypertension, nausea, increased/decreased body temperature, or feeling flushed are the common (>10%) non-psychiatric side effects. All these adverse effects are most pronounced by the end of the injection, dramatically reduced 40 min after, and completely disappear within 4 hours after the injection.[58]
Urinary and liver toxicity
Urinary toxicity occurs primarily in people who use large amounts of ketamine routinely, with 20–30% of frequent users having bladder complaints.[48][59] It includes a range of disorders from cystitis to hydronephrosis to kidney failure.[60] The typical symptoms of ketamine-induced cystitis are frequent urination, dysuria, and urinary urgency sometimes accompanied by pain during urination and blood in urine.[61] The damage to the bladder wall has similarities to both interstitial and eosinophilic cystitis. The wall is thickened, and the functional bladder capacity is as low as 10–150 mL.[60]
Management of ketamine-induced cystitis involves ketamine cessation as the first step. This is followed by NSAIDs and anticholinergics and, if the response is insufficient, by tramadol. The second line treatments are epithelium-protective agents such as oral pentosan polysulfate or intravesical (intra-bladder) instillation of hyaluronic acid. Intravesical botulinum toxin is also useful.[60]
Liver toxicity of ketamine also involves higher doses and repeated administration. In a group of chronic high dose ketamine users, the frequency of liver injury was reported to be about 10%. There are case reports of increased liver enzymes involving ketamine treatment of chronic pain.[60]
Dependence
Some people who regularly use ketamine develop ketamine dependence. Increased subjective feelings of 'high' have been reported in healthy human volunteers exposed to ketamine. Animal experiments also confirm the risk of misuse.[25] Additionally, the rapid onset of effects following insufflation may increase the drug's recreational use potential. The short duration of effects promotes bingeing. Ketamine tolerance rapidly develops, even with repeated medical use, prompting the use of higher doses. Some daily users reported withdrawal symptoms, primarily anxiety, shaking, sweating, and palpitations following the attempts to stop.[25] Cognitive deficits as well as increased dissociation and delusion symptoms were observed in frequent recreational users of ketamine.[62]
Interactions
Ketamine potentiates the sedative effects of propofol[63] and midazolam.[64] Naltrexone potentiates psychotomimetic effects of a low dose of ketamine,[65] while lamotrigine[66] and nimodipine[67] decrease them. Clonidine reduces the salivation, heart rate and blood pressure increases during ketamine anesthesia and decreases the incidence of nightmares.[68]
Clinical observations suggest that benzodiazepines may diminish the antidepressant effects of ketamine.[69] Ketamine is frequently used to treat resistant depression as an add-on to a variety of antidepressants. Hence, it appears most conventional antidepressants can be safely combined with ketamine.[69]
Pharmacology
Mechanism of action
Antagonism of the NMDA receptor is responsible for the anesthetic, analgesic, and psychotomimetic effects of ketamine.[70][71] NMDA receptor antagonism results in analgesia by preventing central sensitization in dorsal horn neurons; in other words, ketamine's actions interfere with pain transmission in the spinal cord.[16]
The mechanism of antidepressant action of ketamine is uncertain. It is not clear whether NMDA receptor is solely responsible for this action or interactions with other receptors are also necessary. It is not clear whether ketamine alone is sufficient for the antidepressive action or its metabolites are also important.[70][72][73] In any case, it has been elucidated that acute blockade of NMDA receptors in the brain results in an activation of α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptors (AMPA receptors), which in turn modulate a variety of downstream signaling pathways to influence neurotransmission in the limbic system and mediate antidepressant effects of NMDA receptor antagonists like ketamine.[51][72] Such downstream actions of this activation of AMPA receptors include upregulation of brain-derived neurotrophic factor (BDNF) and activation of its signaling receptor tropomyosin receptor kinase B (TrkB), activation of the mammalian target of rapamycin (mTOR) pathway, deactivation of glycogen synthase kinase 3 (GSK-3), and inhibition of the phosphorylation of the eukaryotic elongation factor 2 (eEF2) kinase.[51][72][74][75] In addition to blockade of the NMDA receptor, the active metabolite of ketamine hydroxynorketamine, which does not interact importantly with the NMDA receptor but nonetheless indirectly activates AMPA receptors similarly, may also or alternatively be involved in the rapid-onset antidepressant effects of ketamine.[72][73] Recent research has elucidated that an acute inhibition of the lateral habenula, a part of the brain in the limbic system that has been referred to as the "anti-reward center" (projecting to and inhibiting the mesolimbic reward pathway and modulating other limbic areas), may be involved in the antidepressant effects of ketamine.[72][76][77]
Ketamine is a mixture of equal amounts of two enantiomers: esketamine and arketamine. Esketamine is a more potent NMDA receptor antagonist and dissociative hallucinogen than arketamine.[11] Because of the hypothesis that NMDA receptor antagonism underlies the antidepressant effects of ketamine, esketamine was developed as an antidepressant.[11] However, multiple other NMDA receptor antagonists, including memantine, lanicemine, rislenemdaz, rapastinel, and 4-chlorokynurenine, have thus far failed to demonstrate sufficient effectiveness for depression.[11][78] Furthermore, animal research indicates that arketamine, the enantiomer with a weaker NMDA receptor antagonism, as well as (2R,6R)-hydroxynorketamine, the metabolite with negligible affinity for the NMDA receptor but a potent alpha-7 nicotinic receptor antagonist may have antidepressive action.[11][79] It is now argued that NMDA receptor antagonism may not be responsible for the antidepressant effects of ketamine.[11][80][78]
Molecular targets
| Site | Value (μM) | Type | Action | Species | Ref |
|---|---|---|---|---|---|
| NMDA | 0.25–0.66 | Ki | Antagonist | Human | [81][82] |
| MOR | 42 | Ki | Antagonist | Human | [83] |
| MOR2 | 12.1 | Ki | Antagonist | Human | [84] |
| KOR | 28 25 |
Ki Ki |
Antagonist Agonist | Human | [83] [85] |
| σ2 | 26 | Ki | ND | Rat | [86] |
| D2 | 0.5 10 | Ki Ki | Agonist ND | Human | [87] [82][88][89] |
| M1 | 45 | Ki | ND | Human | [90] |
| α2β2 | 92 | IC50 | Antagonist | Human | [91] |
| α2β4 | 29 | IC50 | Antagonist | Human | [91] |
| α3β2 | 50 | IC50 | Antagonist | Human | [91] |
| α3β4 | 9.5 | IC50 | Antagonist | Human | [91] |
| α4β2 | 72 | IC50 | Antagonist | Human | [91] |
| α4β4 | 18 | IC50 | Antagonist | Human | [91] |
| α7 | 3.1 | IC50 | Antagonist | Rat | [79] |
| ERα | 0.34 | Ki | ND | Human | [92] |
| NET | 82–291 | IC50 | Inhibitor | Human | [93][94] |
| DAT | 63 | Ki | Inhibitor | Rat | [93] |
| HCN1 | 8–16 | EC50 | Inhibitor | Mouse | [95] |
| The smaller the value, the stronger the interaction with the site. | |||||
Ketamine principally acts as an antagonist of the NMDA receptor, an ionotropic glutamate receptor.[96] The S(+) and R(–) stereoisomers of ketamine bind to the dizocilpine site of the NMDA receptor with different affinities, the former showing approximately 2- to 3-fold greater affinity for the receptor than the latter.[97] Ketamine may also interact with and inhibit the NMDAR via another allosteric site on the receptor.[98]
With a couple of exceptions ketamine actions at other receptors are far weaker than ketamine's antagonism of the NMDA receptor (see the activity table to the right).[6][99]
Although ketamine is a very weak ligand of the monoamine transporters (Ki > 60 μM), it has been suggested that it may interact with allosteric sites on the monoamine transporters to produce monoamine reuptake inhibition.[82] However, no functional inhibition (IC50) of the human monoamine transporters has been observed with ketamine or its metabolites at concentrations of up to 10,000 nM.[88][96] Moreover, animal studies and at least three human case reports have found no interaction between ketamine and the monoamine oxidase inhibitor (MAOI) tranylcypromine, which is of importance as the combination of a monoamine reuptake inhibitor with an MAOI can produce severe toxicity such as serotonin syndrome or hypertensive crisis.[100][101] Collectively, these findings shed doubt on the involvement of monoamine reuptake inhibition in the effects of ketamine in humans.[100][96][88][101] Ketamine has been found to increase dopaminergic neurotransmission in the brain, but instead of being due to dopamine reuptake inhibition, this may be via indirect/downstream mechanisms, namely through antagonism of the NMDA receptor.[96][88]
Whether ketamine is an agonist of D2 receptors is controversial. Early research by Philip Seeman's group found ketamine to be a D2 partial agonist with the potency similar to that of its NMDA receptor antagonism.[87][102][103] However, later studies by different researchers found the affinity of ketamine of >10 μM for the regular human and rat D2 receptors,[82][88][89] Moreover, whereas D2 receptor agonists like bromocriptine are able to rapidly and powerfully suppress prolactin secretion,[104] subanesthetic doses of ketamine have not been found to do this in humans and in fact have been found to dose-dependently increase prolactin levels.[105][106] Imaging studies have shown mixed results on inhibition of striatal [11C] raclopride binding by ketamine in humans, with some studies finding a significant decrease and others finding no such effect.[107] However, changes in [11C] raclopride binding may be due to changes in dopamine concentrations induced by ketamine rather than binding of ketamine to the D2 receptor.[107]
Relationships between levels and effects
Dissociation and psychotomimetic effects are reported in patients treated with ketamine at plasma concentrations of around 100 to 250 ng/mL (0.42–1.1 μM).[70] The typical intravenous antidepressant dosage of ketamine used to treat depression is low and results in maximal plasma concentrations of 70 to 200 ng/mL (0.29–0.84 μM).[50] At similar plasma concentrations (70 to 160 ng/ml; 0.29–0.67 μM) it also shows analgesic effects.[50] In 1-5 minutes after inducing anesthesia by a rapid intravenous injection of ketamine, its plasma concentration reaches as high as 60–110 μM.[108][109] When the anesthesia was maintained using nitrous oxide together with continuous injection of ketamine, the ketamine concentration stabilized at about 9.3 μM.[108] In an experiment with purely ketamine anesthesia, patients began to awaken once the plasma level of ketamine decreased to about 2,600 ng/mL (11 μM) and became oriented in place and time when the level was down to 1,000 ng/mL (4 μM). [110] In a single-case study, the concentration of ketamine in cerebrospinal fluid, a proxy for the brain concentration, during anesthesia varied between 2.8 and 6.5 μM and was about 40% lower than in plasma.[111]
Pharmacokinetics
Ketamine can be absorbed by many different routes due to both its water and lipid solubility. Intravenous ketamine bioavailability is 100% by definition, intramuscular injection bioavailability is slightly lower at 93%,[6] and epidural bioavailability is 77%.[9] Subcutaneous bioavailability has never been measured but is presumed to be high.[8] Among the less invasive routes, intranasal has the highest bioavailability (45–50%)[6][10] and oral – the lowest (16–20%).[6][10] Sublingual and rectal bioavailabilities are intermediate at about 25–50%.[6][11][10]
After absorption ketamine is rapidly distributed into the brain and other tissues.[71] The plasma protein binding of ketamine is variable at 23 to 47%.[12]
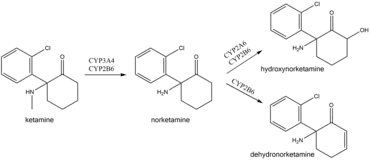
In the body ketamine undergoes extensive metabolism. It is biotransformed by CYP3A4 and CYP2B6 isoenzymes into norketamine, which, in turn, is converted by CYP2A6 and CYP2B6 into hydroxynorketamine and dehydronorketamine.[70] Low oral bioavailability of ketamine is due to the first-pass effect and, possibly, ketamine intestinal metabolism by CYP3A4.[14] As a result, norketamine plasma levels are several-fold higher than ketamine following oral administration, and norketamine may play a role in anesthetic and analgesic action of oral ketamine.[6][14] This also explains why oral ketamine levels are independent of CYP2B6 activity, unlike subcutaneous ketamine levels.[14][112]
After an intravenous injection of tritium-labelled ketamine, 91% of the radioactivity is recovered from urine and 3% from the feces.[17] The medication is excreted mostly in the form of metabolites, with only 2% remaining unchanged. Conjugated hydroxylated derivatives of ketamine (80%) followed by dehydronorketamine (16%) are the most prevalent metabolites detected in urine.[24]
Chemistry
Synthesis
2-chlorobenzonitrile is reacted with the Grignard reagent cyclopentylmagnesium bromide to give (2-chlorophenyl)(cyclopentyl)methanone. This is then brominated using bromine to form the corresponding bromoketone, which is then reacted with methylamine in an aqueous solution to form the methylimino derivative, 1-(2-Chloro-N-methylbenzimidoyl)cyclopentanol, with hydrolysis of the tertiary bromine atom. This final intermediate is then heated in decalin or another suitable high-boiling solvent, upon which a ring-expansion rearrangement occurs, forming ketamine.

Structure
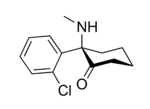
In chemical structure, ketamine is an arylcyclohexylamine derivative. Ketamine is a chiral compound. The more active enantiomer, esketamine (S-ketamine), is also available for medical use under the brand name Ketanest S,[114] while the less active enantiomer, arketamine (R-ketamine), has never been marketed as an enantiopure drug for clinical use.
The optical rotation of a given enantiomer of ketamine can vary between its salts and free base form. The free base form of (S)‑ketamine exhibits dextrorotation and is therefore labelled (S)‑(+)‑ketamine. However, its hydrochloride salt shows levorotation and is thus labelled (S)‑(−)‑ketamine hydrochloride.[115]
Detection
Ketamine may be quantitated in blood or plasma to confirm a diagnosis of poisoning in hospitalized patients, provide evidence in an impaired driving arrest or to assist in a medicolegal death investigation. Blood or plasma ketamine concentrations are usually in a range of 0.5–5.0 mg/L in persons receiving the drug therapeutically (during general anesthesia), 1–2 mg/L in those arrested for impaired driving and 3–20 mg/L in victims of acute fatal overdosage. Urine is often the preferred specimen for routine drug use monitoring purposes. The presence of norketamine, a pharmacologically-active metabolite, is useful for confirmation of ketamine ingestion.[116][117][118]
History
Ketamine was first synthesized in 1962 by Calvin L. Stevens, a professor of Chemistry at Wayne State University and a Parke-Davis consultant. It was known by the developmental code name CI-581. After promising preclinical research in animals, ketamine was tested in human prisoners in 1964.[24] These investigations demonstrated ketamine's short duration of action and reduced behavioral toxicity made it a favorable choice over phencyclidine (PCP) as an anesthetic.[119] The researchers were going to call the state of ketamine anesthesia "dreaming" but Parke-Davis did not like it. Hearing about this problem and about the "disconnected" appearance of the patients, the wife of one of the pharmacologists working on ketamine, Edward Domino, suggested "dissociative anesthesia".[24] Following FDA approval in 1970, ketamine anesthesia was first given to American soldiers during the Vietnam War.[120]
The discovery of antidepressive action of ketamine in 2000[121] has been described as the single most important advance in the treatment of depression in over 50 years.[52][11] It has sparked interest in NMDA receptor antagonists for depression, and has shifted the direction of antidepressant research and development.[122]
Society and culture
Ketamine is primarily sold throughout the world under the brand name Ketalar.[123][1]
Legal status
While ketamine is legally marketed in many countries worldwide,[123] it is also a controlled substance in many countries.[6]
- In Australia, ketamine is listed as a schedule 8 controlled drug under the Poisons Standard (October 2015).[124]
- In Canada, ketamine is classified as a Schedule I narcotic, since 2005.[125]
- In December 2013, the government of India, in response to rising recreational use and the use of ketamine as a date rape drug, has added it to Schedule X of the Drug and Cosmetics Act requiring a special license for sale and maintenance of records of all sales for two years.[126][127]
- In the United Kingdom, it became labeled a Class B drug on 12 February 2014.[128][129]
- The increase in recreational use prompted ketamine to be placed in Schedule III of the United States Controlled Substance Act in August 1999.[130]
Recreational use
At subanesthetic doses ketamine produces a dissociative state, characterised by a sense of detachment from one's physical body and the external world which is known as depersonalization and derealization.[131] At sufficiently high doses, users may experience what is called the "K-hole", a state of dissociation with visual and auditory hallucinations.[132] John C. Lilly, Marcia Moore, D. M. Turner and David Woodard (amongst others) have written extensively about their own entheogenic use of, and psychonautic experiences with, ketamine.[133] Turner died prematurely due to drowning during presumed unsupervised ketamine use.[134] In 2006 the Russian edition of Adam Parfrey's Apocalypse Culture II was banned and destroyed by authorities owing to its inclusion of an essay by Woodard about the entheogenic use of, and psychonautic experiences with, ketamine.[135]:288–295 Recreational ketamine use has been implicated in deaths globally, with more than 90 deaths in England and Wales in the years of 2005–2013.[136] They include accidental poisonings, drownings, traffic accidents, and suicides.[136] The majority of deaths were among young people.[137] Because of its ability to cause confusion and amnesia, ketamine has been used for date rape.[138][120]
Research
Russian doctor Evgeny Krupitsky has claimed to have obtained encouraging results by using ketamine as part of a treatment for alcohol use disorder, which combines psychedelic and aversive techniques.[139][140] Krupitsky and Kolp summarized their work to date in 2007.[141]
Veterinary medicine
In veterinary anaesthesia, ketamine is often used for its anaesthetic and analgesic effects on cats,[142] dogs,[143] rabbits, rats, and other small animals.[144][145] It is frequently used in induction and anaesthetic maintenance in horses. It is an important part of the "rodent cocktail", a mixture of drugs used for anaesthetising rodents.[146] Veterinarians often use ketamine with sedative drugs to produce balanced anaesthesia and analgesia, and as a constant-rate infusion to help prevent pain wind-up. Ketamine is also used to manage pain among large animals. It is the primary intravenous anaesthetic agent used in equine surgery, often in conjunction with detomidine and thiopental, or sometimes guaifenesin.[147]
Ketamine appears not to produce sedation or aneasthesia in snails. Instead, it appears to have an excitatory effect.[148]
References
- Morton IK, Hall JM (6 December 2012). Concise Dictionary of Pharmacological Agents: Properties and Synonyms. Springer Science & Business Media. pp. 159–. ISBN 978-94-011-4439-1. Archived from the original on 11 April 2017.
- "Ketamine (Ketalar) Use During Pregnancy". Drugs.com. 22 November 2019. Retrieved 18 May 2020.
- Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 15: Reinforcement and Addictive Disorders". In Sydor A, Brown RY (eds.). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nd ed.). New York: McGraw-Hill Medical. pp. 374–375. ISBN 978-0-07-148127-4.
Phencyclidine (PCP or angel dust) and ketamine (also known as special K) are structurally related drugs... their reinforcing properties and risks related to compulsive abuse
- Bell RF, Eccleston C, Kalso EA (June 2017). "Ketamine as an adjuvant to opioids for cancer pain" (PDF). The Cochrane Database of Systematic Reviews. 6: CD003351. doi:10.1002/14651858.CD003351.pub3. PMC 6481583. PMID 28657160.
- Moyse DW, Kaye AD, Diaz JH, Qadri MY, Lindsay D, Pyati S (March 2017). "Perioperative Ketamine Administration for Thoracotomy Pain". Pain Physician. 20 (3): 173–184. PMID 28339431.
- Mathew SJ, Zarate Jr CA (25 November 2016). Ketamine for Treatment-Resistant Depression: The First Decade of Progress. Springer. pp. 8–10, 14–22. ISBN 978-3-319-42925-0. Archived from the original on 8 September 2017.
- Brayfield, A, ed. (9 January 2017). "Ketamine Hydrochloride: Martindale: The Complete Drug Reference". MedicinesComplete. London, UK: Pharmaceutical Press. Retrieved 24 August 2017.
- Jianren Mao (19 April 2016). Opioid-Induced Hyperalgesia. CRC Press. pp. 127–. ISBN 978-1-4200-8900-4. Archived from the original on 8 September 2017.
- Pascal Kintz (22 March 2014). Toxicological Aspects of Drug-Facilitated Crimes. Elsevier Science. pp. 87–. ISBN 978-0-12-416969-2. Archived from the original on 8 September 2017.
- Marland S, Ellerton J, Andolfatto G, Strapazzon G, Thomassen O, Brandner B, Weatherall A, Paal P (June 2013). "Ketamine: use in anesthesia". CNS Neurosci Ther. 19 (6): 381–9. doi:10.1111/cns.12072. PMC 6493613. PMID 23521979.
- Hashimoto K (October 2019). "Rapid-acting antidepressant ketamine, its metabolites and other candidates: A historical overview and future perspective". Psychiatry and Clinical Neurosciences. 73 (10): 613–627. doi:10.1111/pcn.12902. PMC 6851782. PMID 31215725.
- Dayton PG, Stiller RL, Cook DR, Perel JM (1983). "The binding of ketamine to plasma proteins: emphasis on human plasma". Eur J Clin Pharmacol. 24 (6): 825–31. doi:10.1007/BF00607095. PMID 6884418. S2CID 807011.
- Hijazi Y, Boulieu R (July 2002). "Contribution of CYP3A4, CYP2B6, and CYP2C9 isoforms to N-demethylation of ketamine in human liver microsomes". Drug Metabolism and Disposition. 30 (7): 853–8. doi:10.1124/dmd.30.7.853. PMID 12065445. S2CID 15787750.
- Rao LK, Flaker AM, Friedel CC, Kharasch ED (December 2016). "Role of Cytochrome P4502B6 Polymorphisms in Ketamine Metabolism and Clearance". Anesthesiology. 125 (6): 1103–1112. doi:10.1097/ALN.0000000000001392. PMID 27763887. S2CID 41380105.
- Sinner B, Graf BM (2008). "Ketamine". In Schüttler J, Schwilden H (eds.). Modern Anesthetics. Handbook of Experimental Pharmacology. 182. pp. 313–33. doi:10.1007/978-3-540-74806-9_15. ISBN 978-3-540-72813-9. PMID 18175098.
- Quibell R, Prommer EE, Mihalyo M, Twycross R, Wilcock A (March 2011). "Ketamine*". Journal of Pain and Symptom Management (Therapeutic Review). 41 (3): 640–9. doi:10.1016/j.jpainsymman.2011.01.001. PMID 21419322.
- Chang T, Glazko AJ (1974). "Biotransformation and disposition of ketamine". Int Anesthesiol Clin. 12 (2): 157–77. doi:10.1097/00004311-197412020-00018. PMID 4603048. S2CID 30723730.
- Sass, William; Fusari, Salvatore (1977). Analytical Profiles of Drug Substances, volume 6. Academic Press. pp. 297–322. doi:10.1016/S0099-5428(08)60347-0. ISBN 9780122608063.
- Green SM, Roback MG, Kennedy RM, Krauss B (May 2011). "Clinical practice guideline for emergency department ketamine dissociative sedation: 2011 update". Annals of Emergency Medicine. 57 (5): 449–61. doi:10.1016/j.annemergmed.2010.11.030. PMID 21256625.
- Zhang K, Hashimoto K (January 2019). "An update on ketamine and its two enantiomers as rapid-acting antidepressants". Expert Review of Neurotherapeutics. 19 (1): 83–92. doi:10.1080/14737175.2019.1554434. PMID 30513009. S2CID 54628949.
- Marcantoni WS, Akoumba BS, Wassef M, Mayrand J, Lai H, Richard-Devantoy S, Beauchamp S (December 2020). "A systematic review and meta-analysis of the efficacy of intravenous ketamine infusion for treatment resistant depression: January 2009 - January 2019". J Affect Disord. 277: 831–841. doi:10.1016/j.jad.2020.09.007. PMID 33065824.
- Swainson J, McGirr A, Blier P, Brietzke E, Richard-Devantoy S, Ravindran N, Blier J, Beaulieu S, Frey BN, Kennedy SH, McIntyre RS, Milev RV, Parikh SV, Schaffer A, Taylor VH, Tourjman V, van Ameringen M, Yatham LN, Ravindran AV, Lam RW (November 2020). "The Canadian Network for Mood and Anxiety Treatments (CANMAT) Task Force Recommendations for the Use of Racemic Ketamine in Adults with Major Depressive Disorder: Recommandations Du Groupe De Travail Du Réseau Canadien Pour Les Traitements De L'humeur Et De L'anxiété (Canmat) Concernant L'utilisation De La Kétamine Racémique Chez Les Adultes Souffrant De Trouble Dépressif Majeur". Can J Psychiatry: 706743720970860. doi:10.1177/0706743720970860. PMID 33174760.
- Bobo WV, Riva-Posse P, Goes FS, Parikh SV (April 2020). "Next-Step Treatment Considerations for Patients With Treatment-Resistant Depression That Responds to Low-Dose Intravenous Ketamine". Focus (Am Psychiatr Publ). 18 (2): 181–192. doi:10.1176/appi.focus.20190048. PMC 7587874. PMID 33162856.
- Domino EF (September 2010). "Taming the ketamine tiger. 1965". Anesthesiology. 113 (3): 678–84. doi:10.1097/ALN.0b013e3181ed09a2. PMID 20693870.
- Morgan CJ, Curran HV (January 2012). "Ketamine use: a review". Addiction. 107 (1): 27–38. doi:10.1111/j.1360-0443.2011.03576.x. PMID 21777321. S2CID 11064759.
- World Health Organization (2019). World Health Organization model list of essential medicines: 21st list 2019. Geneva: World Health Organization. hdl:10665/325771. WHO/MVP/EMP/IAU/2019.06. License: CC BY-NC-SA 3.0 IGO.
- "Ketamine Injection". Drugs.com. Archived from the original on 10 December 2014. Retrieved 1 December 2014.
- Rosenbaum SB, Gupta V, Palacios JL (2020), "Ketamine", StatPearls, StatPearls Publishing, PMID 29262083, retrieved 5 March 2020
- Heshmati F, Zeinali MB, Noroozinia H, Abbacivash R, Mahoori A (December 2003). "Use of ketamine in severe status asthmaticus in intensive care unit". Iranian Journal of Allergy, Asthma, and Immunology. 2 (4): 175–80. PMID 17301376. Archived from the original on 6 October 2014.
- Adams HA (December 1997). "[S-(+)-ketamine. Circulatory interactions during total intravenous anesthesia and analgesia-sedation]" [S-(+)-ketamine. Circulatory interactions during total intravenous anesthesia and analgesia-sedation]. Der Anaesthesist (in German). 46 (12): 1081–7. doi:10.1007/s001010050510. PMID 9451493.
- Wong JJ, Lee JH, Turner DA, Rehder KJ (August 2014). "A review of the use of adjunctive therapies in severe acute asthma exacerbation in critically ill children". Expert Review of Respiratory Medicine. 8 (4): 423–41. doi:10.1586/17476348.2014.915752. PMID 24993063. S2CID 31435021.
- Barrett W, Buxhoeveden M, Dhillon S (October 2020). "Ketamine: a versatile tool for anesthesia and analgesia". Current Opinion in Anesthesiology. 33 (5): 633–638. doi:10.1097/ACO.0000000000000916. PMID 32826629.
- Cohen L, Athaide V, Wickham ME, Doyle-Waters MM, Rose NG, Hohl CM (January 2015). "The effect of ketamine on intracranial and cerebral perfusion pressure and health outcomes: a systematic review". Annals of Emergency Medicine. 65 (1): 43–51.e2. doi:10.1016/j.annemergmed.2014.06.018. PMID 25064742.
- Kurdi MS, Theerth KA, Deva RS (September 2014). "Ketamine: Current applications in anesthesia, pain, and critical care". Anesthesia: Essays and Researches. 8 (3): 283–90. doi:10.4103/0259-1162.143110. PMC 4258981. PMID 25886322.
- Mion G (September 2017). "History of anaesthesia: The ketamine story - past, present and future". Eur J Anaesthesiol. 34 (9): 571–575. doi:10.1097/EJA.0000000000000638. PMID 28731926.
- Nickson C (7 August 2013). "Intubation, Hypotension and Shock". Life in the Fastlane (blog). Critical Care Compendium. Archived from the original on 9 February 2014. Retrieved 10 April 2014.
- Manley G, Knudson MM, Morabito D, Damron S, Erickson V, Pitts L (October 2001). "Hypotension, hypoxia, and head injury: frequency, duration, and consequences". Archives of Surgery. 136 (10): 1118–23. doi:10.1001/archsurg.136.10.1118. PMID 11585502.
- Hemmingsen C, Nielsen JE (November 1991). "Intravenous ketamine for prevention of severe hypotension during spinal anaesthesia". Acta Anaesthesiologica Scandinavica. 35 (8): 755–7. doi:10.1111/j.1399-6576.1991.tb03385.x. PMID 1763596. S2CID 1324453.
- Wong DH, Jenkins LC (May 1975). "The cardiovascular effects of ketamine in hypotensive states". Canadian Anaesthetists' Society Journal. 22 (3): 339–48. doi:10.1007/BF03004843. PMID 1139377.
- Goyal S, Agrawal A (May 2013). "Ketamine in status asthmaticus: A review". Indian Journal of Critical Care Medicine. 17 (3): 154–61. doi:10.4103/0972-5229.117048. PMC 3777369. PMID 24082612.
- Schwenk ES, Viscusi ER, Buvanendran A, Hurley RW, Wasan AD, Narouze S, Bhatia A, Davis FN, Hooten WM, Cohen SP (July 2018). "Consensus Guidelines on the Use of Intravenous Ketamine Infusions for Acute Pain Management From the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists". Reg Anesth Pain Med. 43 (5): 456–466. doi:10.1097/AAP.0000000000000806. PMC 6023582. PMID 29870457.
- Sin B, Ternas T, Motov SM (March 2015). "The use of subdissociative-dose ketamine for acute pain in the emergency department". Academic Emergency Medicine. 22 (3): 251–7. doi:10.1111/acem.12604. PMID 25716117. S2CID 24658476.
- Svenson J, Biedermann M (2011). "Ketamine: a unique drug with several potential uses in the prehospital setting". Journal of Paramedic Practice. 3 (10): 552–556. doi:10.12968/jpar.2011.3.10.552.
- Karlow N, Schlaepfer CH, Stoll CR, Doering M, Carpenter CR, Colditz GA, et al. (October 2018). "A Systematic Review and Meta-analysis of Ketamine as an Alternative to Opioids for Acute Pain in the Emergency Department". Academic Emergency Medicine. 25 (10): 1086–1097. doi:10.1111/acem.13502. PMID 30019434.
- Radvansky BM, Shah K, Parikh A, Sifonios AN, Le V, Eloy JD (2015). "Role of ketamine in acute postoperative pain management: a narrative review". BioMed Research International. 2015: 749837. doi:10.1155/2015/749837. PMC 4606413. PMID 26495312.
- Lee M, Silverman SM, Hansen H, Patel VB, Manchikanti L (2011). "A comprehensive review of opioid-induced hyperalgesia". Pain Physician. 14 (2): 145–61. PMID 21412369.
- Zhou Y, Mannan A, Han Y, Liu H, Guan HL, Gao X, et al. (December 2019). "Efficacy and safety of prophylactic use of ketamine for prevention of postanesthetic shivering: a systematic review and meta analysis". BMC Anesthesiology. 19 (1): 245. doi:10.1186/s12871-019-0910-8. PMC 6937868. PMID 31888509.
- Cohen SP, Bhatia A, Buvanendran A, Schwenk ES, Wasan AD, Hurley RW, Viscusi ER, Narouze S, Davis FN, Ritchie EC, Lubenow TR, Hooten WM (July 2018). "Consensus Guidelines on the Use of Intravenous Ketamine Infusions for Chronic Pain From the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists". Reg Anesth Pain Med. 43 (5): 521–546. doi:10.1097/AAP.0000000000000808. PMC 6023575. PMID 29870458.
- Elia N, Tramèr MR (January 2005). "Ketamine and postoperative pain—a quantitative systematic review of randomised trials". Pain. 113 (1–2): 61–70. doi:10.1016/j.pain.2004.09.036. PMID 15621365. S2CID 25925720.
- Sanacora G, Frye MA, McDonald W, Mathew SJ, Turner MS, Schatzberg AF, et al. (April 2017). "A Consensus Statement on the Use of Ketamine in the Treatment of Mood Disorders". JAMA Psychiatry. 74 (4): 399–405. doi:10.1001/jamapsychiatry.2017.0080. PMID 28249076. S2CID 28320520.
- Molero P, Ramos-Quiroga JA, Martin-Santos R, Calvo-Sánchez E, Gutiérrez-Rojas L, Meana JJ (May 2018). "Antidepressant Efficacy and Tolerability of Ketamine and Esketamine: A Critical Review". CNS Drugs. 32 (5): 411–420. doi:10.1007/s40263-018-0519-3. PMID 29736744. S2CID 13679905.
- Singh I, Morgan C, Curran V, Nutt D, Schlag A, McShane R (May 2017). "Ketamine treatment for depression: opportunities for clinical innovation and ethical foresight". The Lancet. Psychiatry. 4 (5): 419–426. doi:10.1016/S2215-0366(17)30102-5. hdl:10871/30208. PMID 28395988.
- Witt K, Potts J, Hubers A, Grunebaum MF, Murrough JW, Loo C, Cipriani A, Hawton K (January 2020). "Ketamine for suicidal ideation in adults with psychiatric disorders: A systematic review and meta-analysis of treatment trials". Aust N Z J Psychiatry. 54 (1): 29–45. doi:10.1177/0004867419883341. PMID 31729893. S2CID 208035394.
- Bahji A, Vazquez GH, Zarate CA (January 2021). "Comparative efficacy of racemic ketamine and esketamine for depression: A systematic review and meta-analysis". J Affect Disord. 278: 542–555. doi:10.1016/j.jad.2020.09.071. PMC 7704936. PMID 33022440.
- Gomes D, Pimentel J, Bentes C, Aguiar de Sousa D, Antunes AP, Alvarez A, Silva ZC (October 2018). "Consensus Protocol for the Treatment of Super-Refractory Status Epilepticus". Acta Medica Portuguesa. 31 (10): 598–605. doi:10.20344/amp.9679. PMID 30387431.
- Rosati A, De Masi S, Guerrini R (November 2018). "Ketamine for Refractory Status Epilepticus: A Systematic Review". CNS Drugs. 32 (11): 997–1009. doi:10.1007/s40263-018-0569-6. PMID 30232735. S2CID 52302073.
- Strayer RJ, Nelson LS (November 2008). "Adverse events associated with ketamine for procedural sedation in adults". The American Journal of Emergency Medicine. 26 (9): 985–1028. doi:10.1016/j.ajem.2007.12.005. PMID 19091264. Archived from the original on 8 September 2017.
- Acevedo-Diaz EE, Cavanaugh GW, Greenstein D, Kraus C, Kadriu B, Zarate CA, Park LT (February 2020). "Comprehensive assessment of side effects associated with a single dose of ketamine in treatment-resistant depression". J Affect Disord. 263: 568–575. doi:10.1016/j.jad.2019.11.028. PMID 31791675.
- Smith HS (2010). "Ketamine-induced urologic insult (KIUI)". Pain Physician. 13 (6): E343–6. PMID 21102971.
- Castellani D, Pirola GM, Gubbiotti M, Rubilotta E, Gudaru K, Gregori A, Dellabella M (April 2020). "What urologists need to know about ketamine-induced uropathy: A systematic review". Neurourol Urodyn. 39 (4): 1049–1062. doi:10.1002/nau.24341. PMID 32212278. S2CID 214643776.
- Middela S, Pearce I (January 2011). "Ketamine-induced vesicopathy: a literature review". International Journal of Clinical Practice. 65 (1): 27–30. doi:10.1111/j.1742-1241.2010.02502.x. PMID 21155941. S2CID 25034266.
- Morgan CJ, Muetzelfeldt L, Curran HV (January 2010). "Consequences of chronic ketamine self-administration upon neurocognitive function and psychological wellbeing: a 1-year longitudinal study". Addiction. 105 (1): 121–33. doi:10.1111/j.1360-0443.2009.02761.x. PMID 19919593.
- Hui TW, Short TG, Hong W, Suen T, Gin T, Plummer J (March 1995). "Additive interactions between propofol and ketamine when used for anesthesia induction in female patients". Anesthesiology. 82 (3): 641–8. doi:10.1097/00000542-199503000-00005. PMID 7879932. S2CID 24005549.
- Hong W, Short TG, Hui TW (December 1993). "Hypnotic and anesthetic interactions between ketamine and midazolam in female patients". Anesthesiology. 79 (6): 1227–32. doi:10.1097/00000542-199312000-00013. PMID 8267198. S2CID 12246068.
- Krystal JH, Madonick S, Perry E, Gueorguieva R, Brush L, Wray Y, Belger A, D'Souza DC (August 2006). "Potentiation of low dose ketamine effects by naltrexone: potential implications for the pharmacotherapy of alcoholism". Neuropsychopharmacology. 31 (8): 1793–800. doi:10.1038/sj.npp.1300994. PMID 16395307.
- Anand A, Charney DS, Oren DA, Berman RM, Hu XS, Cappiello A, Krystal JH (March 2000). "Attenuation of the neuropsychiatric effects of ketamine with lamotrigine: support for hyperglutamatergic effects of N-methyl-D-aspartate receptor antagonists". Arch Gen Psychiatry. 57 (3): 270–6. doi:10.1001/archpsyc.57.3.270. PMID 10711913.
- Krupitsky EM, Burakov AM, Romanova TN, Grinenko NI, Grinenko AY, Fletcher J, Petrakis IL, Krystal JH (December 2001). "Attenuation of ketamine effects by nimodipine pretreatment in recovering ethanol dependent men: psychopharmacologic implications of the interaction of NMDA and L-type calcium channel antagonists". Neuropsychopharmacology. 25 (6): 936–47. doi:10.1016/S0893-133X(01)00346-3. PMID 11750186.
- Handa F, Tanaka M, Nishikawa T, Toyooka H (February 2000). "Effects of oral clonidine premedication on side effects of intravenous ketamine anesthesia: a randomized, double-blind, placebo-controlled study". J Clin Anesth. 12 (1): 19–24. doi:10.1016/s0952-8180(99)00131-2. PMID 10773503.
- Andrade C (July 2017). "Ketamine for Depression, 5: Potential Pharmacokinetic and Pharmacodynamic Drug Interactions". The Journal of Clinical Psychiatry. 78 (7): e858–e861. doi:10.4088/JCP.17f11802. PMID 28858450.
- Zanos P, Moaddel R, Morris PJ, Riggs LM, Highland JN, Georgiou P, Pereira EF, Albuquerque EX, Thomas CJ, Zarate CA, Gould TD (July 2018). "Ketamine and Ketamine Metabolite Pharmacology: Insights into Therapeutic Mechanisms". Pharmacol Rev. 70 (3): 621–660. doi:10.1124/pr.117.015198. PMC 6020109. PMID 29945898.
- Peltoniemi MA, Hagelberg NM, Olkkola KT, Saari TI (September 2016). "Ketamine: A Review of Clinical Pharmacokinetics and Pharmacodynamics in Anesthesia and Pain Therapy". Clin Pharmacokinet. 55 (9): 1059–77. doi:10.1007/s40262-016-0383-6. PMID 27028535. S2CID 5078489.
- Zanos P, Gould TD (April 2018). "Mechanisms of ketamine action as an antidepressant". Molecular Psychiatry. 23 (4): 801–811. doi:10.1038/mp.2017.255. PMC 5999402. PMID 29532791.
- Zanos P, Thompson SM, Duman RS, Zarate CA, Gould TD (March 2018). "Convergent Mechanisms Underlying Rapid Antidepressant Action". CNS Drugs. 32 (3): 197–227. doi:10.1007/s40263-018-0492-x. PMC 6005380. PMID 29516301.
- Björkholm C, Monteggia LM (March 2016). "BDNF – a key transducer of antidepressant effects". Neuropharmacology. 102: 72–9. doi:10.1016/j.neuropharm.2015.10.034. PMC 4763983. PMID 26519901.
- Castrén E, Kojima M (January 2017). "Brain-derived neurotrophic factor in mood disorders and antidepressant treatments". Neurobiology of Disease. 97 (Pt B): 119–126. doi:10.1016/j.nbd.2016.07.010. hdl:10138/311483. PMID 27425886. S2CID 644350.
- Kim D, Cheong E, Shin HS (June 2018). "Overcoming Depression by Inhibition of Neural Burst Firing". Neuron. 98 (5): 878–879. doi:10.1016/j.neuron.2018.05.032. PMID 29879390.
- Yang Y, Cui Y, Sang K, Dong Y, Ni Z, Ma S, Hu H (February 2018). "Ketamine blocks bursting in the lateral habenula to rapidly relieve depression". Nature. 554 (7692): 317–322. Bibcode:2018Natur.554..317Y. doi:10.1038/nature25509. PMID 29446381. S2CID 3334820.
- Garay R, Zarate CA, Cavero I, Kim YK, Charpeaud T, Skolnick P (October 2018). "The development of glutamate-based antidepressants is taking longer than expected". Drug Discovery Today. 23 (10): 1689–1692. doi:10.1016/j.drudis.2018.02.006. PMC 6211562. PMID 29501913.
- Moaddel R, Abdrakhmanova G, Kozak J, Jozwiak K, Toll L, Jimenez L, Rosenberg A, Tran T, Xiao Y, Zarate CA, Wainer IW (January 2013). "Sub-anesthetic concentrations of (R,S)-ketamine metabolites inhibit acetylcholine-evoked currents in α7 nicotinic acetylcholine receptors". Eur J Pharmacol. 698 (1–3): 228–34. doi:10.1016/j.ejphar.2012.11.023. PMC 3534778. PMID 23183107.
- "Arketamine – Jiangsu Hengrui Medicine – AdisInsight".
- Morris PJ, Moaddel R, Zanos P, Moore CE, Gould TD, Zarate CA, Thomas CJ (September 2017). "Synthesis and N-Methyl-d-aspartate (NMDA) Receptor Activity of Ketamine Metabolites". Organic Letters. 19 (17): 4572–4575. doi:10.1021/acs.orglett.7b02177. PMC 5641405. PMID 28829612.
- Roth BL, Gibbons S, Arunotayanun W, Huang XP, Setola V, Treble R, Iversen L (2013). "The ketamine analogue methoxetamine and 3- and 4-methoxy analogues of phencyclidine are high affinity and selective ligands for the glutamate NMDA receptor". PLOS ONE. 8 (3): e59334. Bibcode:2013PLoSO...859334R. doi:10.1371/journal.pone.0059334. PMC 3602154. PMID 23527166.
- Hirota K, Okawa H, Appadu BL, Grandy DK, Devi LA, Lambert DG (January 1999). "Stereoselective interaction of ketamine with recombinant mu, kappa, and delta opioid receptors expressed in Chinese hamster ovary cells". Anesthesiology. 90 (1): 174–82. doi:10.1097/00000542-199901000-00023. PMID 9915326.
- Hirota K, Sikand KS, Lambert DG (1999). "Interaction of ketamine with mu2 opioid receptors in SH-SY5Y human neuroblastoma cells". Journal of Anesthesia. 13 (2): 107–9. doi:10.1007/s005400050035. PMID 14530949. S2CID 9322174.
- Nemeth CL, Paine TA, Rittiner JE, Béguin C, Carroll FI, Roth BL, Cohen BM, Carlezon WA (June 2010). "Role of kappa-opioid receptors in the effects of salvinorin A and ketamine on attention in rats". Psychopharmacology (Berl). 210 (2): 263–74. doi:10.1007/s00213-010-1834-7. PMC 2869248. PMID 20358363.
- Robson MJ, Elliott M, Seminerio MJ, Matsumoto RR (April 2012). "Evaluation of sigma (σ) receptors in the antidepressant-like effects of ketamine in vitro and in vivo". Eur Neuropsychopharmacol. 22 (4): 308–17. doi:10.1016/j.euroneuro.2011.08.002. PMID 21911285. S2CID 24494428.
- Kapur S, Seeman P (2002). "NMDA receptor antagonists ketamine and PCP have direct effects on the dopamine D(2) and serotonin 5-HT(2)receptors-implications for models of schizophrenia". Molecular Psychiatry. 7 (8): 837–44. doi:10.1038/sj.mp.4001093. PMID 12232776.
- Can A, Zanos P, Moaddel R, Kang HJ, Dossou KS, Wainer IW, et al. (October 2016). "Effects of Ketamine and Ketamine Metabolites on Evoked Striatal Dopamine Release, Dopamine Receptors, and Monoamine Transporters". The Journal of Pharmacology and Experimental Therapeutics. 359 (1): 159–70. doi:10.1124/jpet.116.235838. PMC 5034706. PMID 27469513.
- Jordan S, Chen R, Fernalld R, Johnson J, Regardie K, Kambayashi J, et al. (July 2006). "In vitro biochemical evidence that the psychotomimetics phencyclidine, ketamine and dizocilpine (MK-801) are inactive at cloned human and rat dopamine D2 receptors". European Journal of Pharmacology. 540 (1–3): 53–6. doi:10.1016/j.ejphar.2006.04.026. PMID 16730695.
- Hirota K, Hashimoto Y, Lambert DG (December 2002). "Interaction of intravenous anesthetics with recombinant human M1-M3 muscarinic receptors expressed in chinese hamster ovary cells". Anesth Analg. 95 (6): 1607–10, table of contents. doi:10.1097/00000539-200212000-00025. PMID 12456425. S2CID 25643394.
- Yamakura T, Chavez-Noriega LE, Harris RA (April 2000). "Subunit-dependent inhibition of human neuronal nicotinic acetylcholine receptors and other ligand-gated ion channels by dissociative anesthetics ketamine and dizocilpine". Anesthesiology. 92 (4): 1144–53. doi:10.1097/00000542-200004000-00033. PMID 10754635. S2CID 23651917.
- Ho MF, Correia C, Ingle JN, Kaddurah-Daouk R, Wang L, Kaufmann SH, Weinshilboum RM (June 2018). "Ketamine and ketamine metabolites as novel estrogen receptor ligands: Induction of cytochrome P450 and AMPA glutamate receptor gene expression". Biochemical Pharmacology. 152: 279–292. doi:10.1016/j.bcp.2018.03.032. PMC 5960634. PMID 29621538.
- Nishimura M, Sato K, Okada T, Yoshiya I, Schloss P, Shimada S, Tohyama M (March 1998). "Ketamine inhibits monoamine transporters expressed in human embryonic kidney 293 cells". Anesthesiology. 88 (3): 768–74. doi:10.1097/00000542-199803000-00029. PMID 9523822. S2CID 30159489.
- Zhao Y, Sun L (November 2008). "Antidepressants modulate the in vitro inhibitory effects of propofol and ketamine on norepinephrine and serotonin transporter function". J Clin Neurosci. 15 (11): 1264–9. doi:10.1016/j.jocn.2007.11.007. PMC 2605271. PMID 18815045.
- Chen X, Shu S, Bayliss DA (January 2009). "HCN1 channel subunits are a molecular substrate for hypnotic actions of ketamine". The Journal of Neuroscience. 29 (3): 600–9. doi:10.1523/JNEUROSCI.3481-08.2009. PMC 2744993. PMID 19158287.
- Tyler MW, Yourish HB, Ionescu DF, Haggarty SJ (June 2017). "Classics in Chemical Neuroscience: Ketamine". ACS Chemical Neuroscience. 8 (6): 1122–1134. doi:10.1021/acschemneuro.7b00074. PMID 28418641.
- Hirota K, Lambert DG (October 1996). "Ketamine: its mechanism(s) of action and unusual clinical uses". British Journal of Anaesthesia. 77 (4): 441–4. doi:10.1093/bja/77.4.441. PMID 8942324. Archived from the original on 20 October 2015.
- Orser BA, Pennefather PS, MacDonald JF (April 1997). "Multiple mechanisms of ketamine blockade of N-methyl-D-aspartate receptors". Anesthesiology. 86 (4): 903–17. doi:10.1097/00000542-199704000-00021. PMID 9105235. S2CID 2164198.
- Lodge D, Mercier MS (September 2015). "Ketamine and phencyclidine: the good, the bad and the unexpected". British Journal of Pharmacology. 172 (17): 4254–76. doi:10.1111/bph.13222. PMC 4556466. PMID 26075331.
- Kraus C, Rabl U, Vanicek T, Carlberg L, Popovic A, Spies M, et al. (March 2017). "Administration of ketamine for unipolar and bipolar depression". International Journal of Psychiatry in Clinical Practice. 21 (1): 2–12. doi:10.1080/13651501.2016.1254802. PMID 28097909. S2CID 35626369.
- Bartova L, Vogl SE, Stamenkovic M, Praschak-Rieder N, Naderi-Heiden A, Kasper S, Willeit M (November 2015). "Combination of intravenous S-ketamine and oral tranylcypromine in treatment-resistant depression: A report of two cases". European Neuropsychopharmacology. 25 (11): 2183–4. doi:10.1016/j.euroneuro.2015.07.021. PMID 26302763. S2CID 39039021.
- Seeman P, Guan HC (November 2008). "Phencyclidine and glutamate agonist LY379268 stimulate dopamine D2High receptors: D2 basis for schizophrenia". Synapse. 62 (11): 819–28. doi:10.1002/syn.20561. PMID 18720422. S2CID 206519749.
- Seeman P, Guan HC, Hirbec H (August 2009). "Dopamine D2High receptors stimulated by phencyclidines, lysergic acid diethylamide, salvinorin A, and modafinil". Synapse. 63 (8): 698–704. doi:10.1002/syn.20647. PMID 19391150. S2CID 17758902.
- The Role of Brain Dopamine. Springer Science & Business Media. 6 December 2012. pp. 23–. ISBN 978-3-642-73897-5.
- Krystal JH, Karper LP, Seibyl JP, Freeman GK, Delaney R, Bremner JD, et al. (March 1994). "Subanesthetic effects of the noncompetitive NMDA antagonist, ketamine, in humans. Psychotomimetic, perceptual, cognitive, and neuroendocrine responses". Archives of General Psychiatry. 51 (3): 199–214. doi:10.1001/archpsyc.1994.03950030035004. PMID 8122957.
- Hergovich N, Singer E, Agneter E, Eichler HG, Graselli U, Simhandl C, Jilma B (May 2001). "Comparison of the effects of ketamine and memantine on prolactin and cortisol release in men. a randomized, double-blind, placebo-controlled trial". Neuropsychopharmacology. 24 (5): 590–3. doi:10.1016/S0893-133X(00)00194-9. PMID 11282259.
- Rabiner EA (May 2007). "Imaging of striatal dopamine release elicited with NMDA antagonists: is there anything there to be seen?". Journal of Psychopharmacology. 21 (3): 253–8. doi:10.1177/0269881107077767. PMID 17591653. S2CID 23776189.
- Idvall J, Ahlgren I, Aronsen KR, Stenberg P (December 1979). "Ketamine infusions: pharmacokinetics and clinical effects". Br J Anaesth. 51 (12): 1167–73. doi:10.1093/bja/51.12.1167. PMID 526385.
- Domino EF, Zsigmond EK, Domino LE, Domino KE, Kothary SP, Domino SE (February 1982). "Plasma levels of ketamine and two of its metabolites in surgical patients using a gas chromatographic mass fragmentographic assay". Anesth Analg. 61 (2): 87–92. doi:10.1213/00000539-198202000-00004. PMID 7198883. S2CID 27596215.
- White PF, Schüttler J, Shafer A, Stanski DR, Horai Y, Trevor AJ (February 1985). "Comparative pharmacology of the ketamine isomers. Studies in volunteers". Br J Anaesth. 57 (2): 197–203. doi:10.1093/bja/57.2.197. PMID 3970799.
- Stenberg P, Idvall J (July 1981). "Does ketamine metabolite II exist in vivo?". Br J Anaesth. 53 (7): 778. doi:10.1093/bja/53.7.778. PMID 7248132.
- Li Y, Jackson KA, Slon B, Hardy JR, Franco M, William L, Poon P, Coller JK, Hutchinson MR, Currow DC, Somogyi AA (August 2015). "CYP2B6*6 allele and age substantially reduce steady-state ketamine clearance in chronic pain patients: impact on adverse effects". Br J Clin Pharmacol. 80 (2): 276–84. doi:10.1111/bcp.12614. PMC 4541975. PMID 25702819.
- Synthesis of ketamine references:
- Stevens CL, Klundt IL, Munk ME, Pillai MD (1965). "Amino ketone rearrangements. IV. Thermal rearrangements of α-amino methyl ketones". Journal of Organic Chemistry. 30 (9): 2967–72. doi:10.1021/jo01020a019.
- US patent 3254124, Stevens, Calvin L., "Aminoketones and methods for their production", issued 1966-05-31, assigned to Parke Davis & Co.
- BE 634208, Stevens, Calvin L., "Procédé de production d'aminocétones", issued 1963-07-15.
- Krüger AD (1998). "[Current aspects of using ketamine in childhood]". Anaesthesiologie und Reanimation (in German). 23 (3): 64–71. PMID 9707751.
- Chankvetadze B, Burjanadze N, Breitkreutz J, Bergander K, Bergenthal D, Kataeva O, Fröhlich R, Luftmann H, Blaschke G (2002). "Mechanistic study on the opposite migration order of the enantiomers of ketamine with α- and β-cyclodextrin in capillary electrophoresis". Journal of Separation Science. 25 (15–17): 1155–1166. doi:10.1002/1615-9314(20021101)25:15/17<1155::AID-JSSC1155>3.0.CO;2-M.
- Feng N, Vollenweider FX, Minder EI, Rentsch K, Grampp T, Vonderschmitt DJ. Development of a gas chromatography-mass spectrometry method for determination of ketamine in plasma and its application to human samples. Ther. Drug Monit. 17: 95–100, 1995.
- Parkin MC, Turfus SC, Smith NW, Halket JM, Braithwaite RA, Elliott SP, Osselton MD, Cowan DA, Kicman AT. Detection of ketamine and its metabolites in urine by ultra high pressure liquid chromatography-tandem mass spectrometry. J. Chrom. B 876: 137–142, 2008.
- R. Baselt, Disposition of Toxic Drugs and Chemicals in Man, 8th edition, Biomedical Publications, Foster City, CA, 2008, pp. 806–808.
- Corssen G, Domino EF (January–February 1966). "Dissociative anesthesia: further pharmacologic studies and first clinical experience with the phencyclidine derivative CI-581". Anesthesia and Analgesia. 45 (1): 29–40. doi:10.1213/00000539-196601000-00007. PMID 5325977. S2CID 29516392.
- "Ketamine". Center for Substance Abuse Research (CESAR); University of Maryland, College Park. 29 October 2013. Archived from the original on 12 November 2013. Retrieved 27 July 2014.
- Berman RM, Cappiello A, Anand A, Oren DA, Heninger GR, Charney DS, Krystal JH (February 2000). "Antidepressant effects of ketamine in depressed patients". Biol Psychiatry. 47 (4): 351–4. doi:10.1016/s0006-3223(99)00230-9. PMID 10686270. S2CID 43438286.
- Dhir A (January 2017). "Investigational drugs for treating major depressive disorder". Expert Opinion on Investigational Drugs. 26 (1): 9–24. doi:10.1080/13543784.2017.1267727. PMID 27960559. S2CID 45232796.
- Index Nominum 2000: International Drug Directory. Taylor & Francis. 2000. pp. 584–585. ISBN 978-3-88763-075-1.
- Poisons Standard October 2015 "Archived copy". Archived from the original on 19 January 2016. Retrieved 6 January 2016.CS1 maint: archived copy as title (link)
- Legal status of ketamine in Canada references:
- "Statutes of Canada (S.C.) Controlled Drugs and Substances Act (S.C. 1996 c.19) Schedule I § 14". Justice Laws Website. Government of Canada. 12 June 2014. Archived from the original on 22 November 2013.
- "Order Amending Schedule I to the Controlled Drugs and Substances Act" (PDF). Canada Gazette Part II. 139 (19). 21 September 2005. p. 2130. Archived from the original (PDF) on 8 August 2014. Retrieved 2 August 2014.
- "Status of ketamine under CDSA". Canadian Society of Customs Brokers. 2 May 2005. Archived from the original on 10 August 2014. Retrieved 2 August 2014.
- "Ketamine drug brought under 'Schedule X' to curb abuse". The Times of India. 7 January 2014. Archived from the original on 14 April 2014. Retrieved 2 August 2014.
- Deb Roy S (30 December 2013). "Govt makes notorious 'date rape' drug ketamine harder to buy or sell". The Times of India. Archived from the original on 30 December 2013.
- Baker, Norman; (Minister for Crime Prevention); Home Office; United Kingdom (12 February 2014), Response to ACMD recommendation on ketamine (PDF) (Correspondence to Les Iverson [chair of]; Advisory Council on the Misuse of Drugs), Crown copyright; Open Government Licence, archived (PDF) from the original on 28 February 2014, retrieved 21 February 2014.
- Dixon H (12 February 2014). "Party drug ketamine to be upgraded to Class B". The Daily Telegraph. Archived from the original on 9 June 2014. Retrieved 2 August 2014.
- Marshall DR, (Deputy Administrator), Drug Enforcement Administration, Department of Justice (13 July 1999). "Schedules of Controlled Substances: Placement of Ketamine into Schedule III [21 CFR Part 1308. Final Rule 99-17803]" (PDF). Rules and Regulations. Federal Register. 64 (133): 37673–5. Archived (PDF) from the original on 5 May 2015.
- Giannini AJ, Underwood NA, Condon M (November 2000). "Acute ketamine intoxication treated by haloperidol: a preliminary study". American Journal of Therapeutics. 7 (6): 389–91. doi:10.1097/00045391-200007060-00008. PMID 11304647.
- Giannini AJ (1999). Drug Abuse. Los Angeles: Health Information Press. p. 104. ISBN 978-1-885987-11-2.
- References for recreational use in literature:
- Lilly JC (1997). The Scientist: A Metaphysical Autobiography. Berkeley, CA: Ronin. pp. 144–. ISBN 978-0-914171-72-0.
- Kelly K (2001). The Little Book of Ketamine. Ronin. pp. 23, 40–45, 46–51, ibid. ISBN 978-1-57951-121-0.
- Alltounian HS, Moore M (1978). Journeys Into the Bright World. Rockport, MA: Para Research. ISBN 978-0-914918-12-7.
- Palmer C, Horowitz M (2000). Sisters of the Extreme: Women Writing on the Drug Experience. Inner Traditions. pp. 254–258, ibid. ISBN 978-0-89281-757-3.
- Turner DM (1994). The Essential Psychedelic Guide. San Francisco: Panther Press. ISBN 978-0-9642636-1-1.
- Jansen K (2001). Ketamine: Dreams and Realities. Multidisciplinary Association for Psychedelic Studies. pp. 50, 89. ISBN 978-0-9660019-3-8.
- Woodard, D., “The Ketamine Necromance”, in A. Parfrey, Apocalypse Culture II (Los Angeles: Feral House, 2000), pp. 288–295.
- See Max Daly, 2014, "The Sad Demise of Nancy Lee, One of Britain's Ketamine Casualties," at Vice (online), 23 July 2014, see "The Sad Demise of Nancy Lee, One of Britain's Ketamine Casualties". 23 July 2014. Archived from the original on 7 June 2015. Retrieved 7 June 2015., accessed 7 June 2015.
- The Crown, 2013, "Drug related deaths involving ketamine in England and Wales," a report of the Mortality team, Life Events and Population Sources Division, Office for National Statistics, the Crown (U.K.), see "Archived copy". Archived from the original on 7 June 2015. Retrieved 7 June 2015.CS1 maint: archived copy as title (link) and "Deaths Related to Drug Poisoning in England and Wales – Office for National Statistics". Archived from the original on 19 June 2015. Retrieved 7 June 2015., accessed 7 June 2015.
- "Do you know... Ketamine". Knowledge Exchange. Toronto: Centre for Addiction and Mental Health. 2003. Archived from the original on 7 April 2014. Retrieved 27 July 2014.
- Krupitsky EM, Grineko AY, Berkaliev TN, Paley AI, Tetrov UN, Mushkov KA, Borodikin YS (1992). "The combination of psychedelic and aversive approaches in alcoholism treatment". Alcoholism Treatment Quarterly. 9 (1): 99–105. doi:10.1300/J020V09N01_09.
- Krupitsky EM, Grinenko AY (1997). "Ketamine psychedelic therapy (KPT): a review of the results of ten years of research". Journal of Psychoactive Drugs. 29 (2): 165–83. doi:10.1080/02791072.1997.10400185. PMID 9250944.
- Krupitsky E, Kolp E (2007). "Ch. 6: Ketamine Psychedelic Psychotherapy". In Winkelman MJ, Roberts TB (eds.). Psychedelic Medicine: New Evidence for Hallucinogens as Treatments. 2. Westport, CT: Praeger. ISBN 978-0-275-99023-7.
- Robertson SA, Taylor PM (October 2004). "Pain management in cats—past, present and future. Part 2. Treatment of pain—clinical pharmacology". Journal of Feline Medicine and Surgery. 6 (5): 321–33. doi:10.1016/j.jfms.2003.10.002. PMID 15363764. S2CID 25572412.
- Lamont LA (November 2008). "Adjunctive analgesic therapy in veterinary medicine". The Veterinary Clinics of North America. Small Animal Practice. 38 (6): 1187–203, v. doi:10.1016/j.cvsm.2008.06.002. PMID 18954680.
- Stunkard JA, Miller JC (September 1974). "An outline guide to general anesthesia in exotic species". Veterinary Medicine, Small Animal Clinician. 69 (9): 1181–6. PMID 4604091.
- Riviere JE, Papich MG (2009). Veterinary Pharmacology and Therapeutics. John Wiley & Sons. p. 200. ISBN 978-1-118-68590-7.
- Standard Operating Procedure No. 1 Anesthesia and Analgesia in Rodents, Washington College, 2012, pp. 1–2, archived from the original on 4 August 2013, retrieved 27 November 2015
- Hubbell, J. A., W. W. Muir, and R. A. Sams. "Guaifenesin: cardiopulmonary effects and plasma concentrations in horses." American journal of veterinary research 41.11 (1980): 1751-1755.
- Woodall AJ, McCrohan CR (December 2000). "Excitatory actions of propofol and ketamine in the snail Lymnaea stagnalis". Comparative Biochemistry and Physiology. Toxicology & Pharmacology. 127 (3): 297–305. doi:10.1016/S0742-8413(00)00155-9. PMID 11246501.
External links
| Wikimedia Commons has media related to Ketamine. |
- "Ketamine". Drug Information Portal. U.S. National Library of Medicine.
- "Ketamine hydrochloride". Drug Information Portal. U.S. National Library of Medicine.
- DEA: Ketamine Fact Sheet
| Authority control |
|---|