Work of breathing
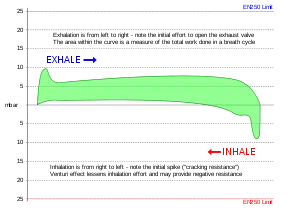
Work of breathing (WOB) is the energy expended to inhale and exhale a breathing gas. It is usually expressed as work per unit volume, for example, joules/litre, or as a work rate (power), such as joules/min or equivalent units, as it is not particularly useful without a reference to volume or time. It can be calculated in terms of the pulmonary pressure multiplied by the change in pulmonary volume, or in terms of the oxygen consumption attributable to breathing.[1][2] In a normal resting state the work of breathing constitutes about 5% of the total body oxygen consumption. It can increase considerably due to illness[3] or constraints on gas flow imposed by breathing apparatus, ambient pressure, or breathing gas composition.
Mechanism of breathing
The normal relaxed state of the lung and chest is partially empty. Further exhalation requires muscular work. Inhalation is an active process requiring work.[4] Some of this work is to overcome frictional resistance to flow, and part is used to deform elastic tissues, and is stored as potential energy, which is recovered during the passive process of exhalation, Tidal breathing does not require active muscle contraction during exhalation. The required energy is provided by the stored elastic energy.
When there is increased gas flow resistance, the optimal respiratory rate decreases.
Work against elastic recoil
This work (generally during the inhalation phase) is stored as potential energy which is recovered during exhalation.
Work against non-elastic resistance
A pressure difference is required to overcome the frictional resistance to gas flow due to viscosity, and to provide non-elastic components of movement of the airway tissues to accommodate pulmonary volume change. Total work done against non elastic forces is 35% of total.
Immersion effects
The properties of the lung can vary if a pressure differential exists between the breathing gas supply and the ambient pressure on the chest. The relaxed internal pressure in the lungs is equal to the pressure at the mouth, and in the immersed diver, the pressure on the chest may vary from the pressure at the mouth depending on the attitude of the diver in the water. This pressure difference is the static lung load or hydrostatic imbalance.[5]
A negative static lung load occurs when the gas supply pressure is lower than the ambient pressure at the chest, and the diver needs to apply more effort to inhale. The small negative pressure differential inside the air passages induces blood engorgement of the distensible lung blood vessels, reducing the compliance of the lung tissue and making the lung stiffer than normal, therefore requiring more muscular effort to move a given volume of gas through the airways. This effect can occur in an upright open-circuit diver, where the chest is deeper than the regulator, and in a rebreather diver if the chest is deeper than the counterlung and will increase the work of breathing.[5]
Mechanics
Work is defined as a force applied over a distance. The SI unit of work is the Joule, equivalent to a force of 1 Newton exerted along a distance of 1 metre. In gas flow across a constant section this equates to a volume flowing against a pressure:[note 1]
Work = Pressure x Volume
and Power = Work / time
with SI units for Power: Watts = Joules per second
Work of breathing should more accurately be called power of breathing unless referring to the work associated with a specific number of breaths, or a given interval of time.
Signs of Increased Work of Breathing
Because measuring the work of breathing requires complex instrumentation, measuring it in patients with acute serious illness is difficult and risky. Instead, physicians determine if the work of breathing is increased by gestalt or by examining the patient looking for signs of increased breathing effort. These signs include nasal flaring, the contraction of sternomastoid, and thoraco-abdominal paradox.[6]
Underwater breathing apparatus
In the diving industry the performance of breathing apparatus is often referred to as work of breathing. In this context it generally means the work of an average single breath taken through the specified apparatus for given conditions of ambient pressure, underwater environment, flow rate during the breathing cycle, and gas mixture - underwater divers may breathe oxygen-rich breathing gas to reduce the risk of decompression sickness, or gases containing helium to reduce narcotic effects. Helium also has the effect of reducing the work of breathing by reducing density of the mixture, though helium's viscosity is fractionally greater than nitrogen's.[7][8] Standards for these conditions exist and to make useful comparisons between breathing apparatus they must be tested to the same standard.
Standards for testing underwater breathing apparatus
- EN 250:2014. Respiratory equipment – Open-circuit self-contained compressed air diving apparatus – Requirements, testing, marking.[9]
- EN 14143:2013. Respiratory equipment. Self-contained re-breathing diving apparatus[9]
- EN 15333 –1: 2008 COR 2009 – Respiratory Equipment – Open-Circuit Umbilical Supplied Compressed Gas Diving Apparatus – Part 1: Demand Apparatus.[9]
- BS 8547:2016 defines requirements for demand regulators to be used at depths exceeding 50 m.[10]
Variations and management of work of breathing
Factors which influence the work of breathing of an underwater breathing apparatus include density and viscosity of the gas, flow rates, cracking pressure (the pressure differential required to open the demand valve), and back pressure over exhaust valves.[5]
Work of breathing of a diver has a physiological component as well as the equipment component. for a given breathing gas mixture, the density will increase with an increase in depth. A higher gas density requires more effort to accelerate the gas in the transition between inhalation and exhalation. To minimise the work of breathing the flow velocity can be reduced, but this will reduce RMV unless the depth of breathing is increased to compensate. Slow deep breathing improves efficiency of respiration by increasing gas turnover in the alveoli, and exertion must be limited to match the gas transfer possible from the RMV which can be comfortably maintained over long periods. Exceeding this maximum continuous exertion may lead to carbon dioxide buildup, which can cause accelerated breathing rate, with increased turbulence, leading to lower efficiency, reduced RMV and higher work of breathing in a positive feedback loop. At extreme depths this can occur even at relatively low levels of exertion, and it may be difficult or impossible to break the cycle. The resulting stress can be a cause of panic as the perception is of an insufficient gas supply due to carbon dioxide buildup though oxygenation may be adequate.[11]
Negative static lung load increases work of breathing and can vary depending on the relative depth of the regulator diaphragm to the lungs in open circuit equipment, and the relative depth of the counterlung to the lungs in a rebreather.[5]
Gas density at ambient pressure is a limiting factor on the ability of a diver to effectively eliminate carbon dioxide at depth for a given work of breathing.[5] At increased ambient pressure the increased breathing gas density causes greater airway resistance. Maximum exercise ventilation and maximum voluntary ventilation are reduced as a function of density, which for a given gas mixture is proportional to pressure. Maximum voluntary ventilation is approximated by a square root function of gas density. Exhalation flow rate is limited by effort independent turbulent flow. Once this occurs further attempts to increase flow rate are actively counterproductive and contribute to further accumulation of carbon dioxide. The effects of negative static lung load are amplified by increased gas density.[12]
To reduce risk of hypercapnia, divers may adopt a breathing pattern that is slower and deeper than normal rather than fast and shallow, as this gives maximum gas exchange per unit effort by minimising turbulence and dead space effects. [13]
Carbon dioxide retention and toxicity
Carbon dioxide is a product of cell metabolism which is eliminated by gas exchange in the lungs while breathing. The rate of production is variable with exertion, but there is a basic minimum. If the rate of elimination is less than the rate of production, the levels will increase, and produce symptoms of toxicity such as headache, shortness of breath and mental impairment, eventually loss of consciousness, which can lead to drowning. In diving there are factors which increase carbon dioxide production (exertion), and factors which can impair elimination, making divers particularly vulnerable to carbon dioxide toxicity.[13]
Oxygen is consumed and carbon dioxide produced in the same quantities underwater as at the surface for the same amount of work, but breathing requires work, and work of breathing can be much greater underwater, and work of breathing is similar to other forms of work in the production of carbon dioxide.[13]
The ability of a diver to respond to increases in work of breathing is limited. As work of breathing increases, the additional carbon dioxide produce in doing this work pushes up the need for higher elimination rate, which is proportional to ventilation, in the case of negligible carbon dioxide in the inspired air.[13]
Carbon dioxide production by the tissues is a simple function of tissue metabolism and oxygen consumption. The more work done in a tissue, the more oxygen will be consumed and the more carbon dioxide will be produced. Carbon dioxide removal in the alveoli depends on the partial pressure gradient for carbon dioxide diffusion between blood and the alveolar gas. This gradient is maintained by flushing carbon dioxide out of the alveoli during breathing, which depends on replacing air in the alveoli with more carbon dioxide by air with less carbon dioxide. The more air moved in and out of the alveoli during breathing, the more carbon dioxide is flushed out, and the greater the pressure gradient between the venous blood and alveolar gas that drives carbon dioxide diffusion from the blood. Maintenance of the correct carbon dioxide levels is critically dependent on adequate lung ventilation, and there are multiple aspects of diving that can interfere with adequate ventilation of the lungs.[13]
Measurement of underwater breathing apparatus performance
The ANSTI machine is used for automated testing of underwater breathing apparatus.[14]
Notes
- Force = Pressure x Area, and Distance = Volume / Area. When both refer to the same area, Force x Distance = (Pressure x Area) x (Volume/Area) = Pressure x Volume
References
- Medical Dictionary for the Health Professions and Nursing. S.v. "work of breathing." Retrieved September 8, 2015, from http://medical-dictionary.thefreedictionary.com/work+of+breathing
- Medical Dictionary. S.v. "work of breathing." Retrieved September 8, 2015, from http://medical-dictionary.thefreedictionary.com/work+of+breathing
- Mosby's Medical Dictionary, 8th edition. S.v. "work of breathing." Retrieved September 8, 2015, from http://medical-dictionary.thefreedictionary.com/work+of+breathing
- Aliverti, Andrea; Pedotti, Antonio (2014-06-19). Mechanics of Breathing: New Insights from New Technologies. Springer. p. 3. ISBN 9788847056473.
- Anthony, Gavin; Mitchell, Simon J. (2016). Pollock, NW; Sellers, SH; Godfrey, JM (eds.). Respiratory Physiology of Rebreather Diving (PDF). Rebreathers and Scientific Diving. Proceedings of NPS/NOAA/DAN/AAUS June 16–19, 2015 Workshop. Wrigley Marine Science Center, Catalina Island, CA. pp. 66–79.
- Tulaimat, A; Patel, A; Wisniewski, M; Gueret, R (August 2016). "The validity and reliability of the clinical assessment of increased work of breathing in acutely ill patients". Journal of Critical Care. 34: 111–5. doi:10.1016/j.jcrc.2016.04.013. PMID 27288621.
- "Viscosity" (PDF). resources.saylor.org. p. 9. Retrieved 27 June 2019.
- Kestin, J; Di Pippo, R. "2r. Viscosity of gases" (PDF). web.mit.edu. p. 2-242. Retrieved 27 June 2019.
- Staff (August 2014). "Diving Breathing Apparatus" (PDF). Diving Standards. Dublin: Health and Safety Authority. Archived from the original (PDF) on 2016-11-18. Retrieved 18 November 2016.
- Committee PH/4/7 (31 March 2016). BS 8547:2016 - Respiratory equipment. Breathing gas demand regulator used for diving to depths greater than 50 metres. Requirements and test methods. London: British Standards Institute. ISBN 978-0-580-89213-4.
- Mount, Tom (August 2008). "1 ~ The Basics Of Physiology For Technical Divers". In Mount, Tom; Dituri, Joseph (eds.). Exploration and Mixed Gas Diving Encyclopedia (1st ed.). Miami Shores, Florida: International Association of Nitrox Divers. pp. 3–32. ISBN 978-0-915539-10-9.
- Mitchell, Simon J.; Cronjé, Frans J.; Meintjes, W. A. Jack; Britz, Hermie C. (2007). "Fatal Respiratory Failure During a "Technical" Rebreather Dive at Extreme Pressure". Aviation, Space, and Environmental Medicine. 78 (2): 81–86. Retrieved 21 November 2019.
- Mitchell, Simon (August 2008). "Four: Carbon Dioxide Retention". In Mount, Tom; Dituri, Joseph (eds.). Exploration and Mixed Gas Diving Encyclopedia (1st ed.). Miami Shores, Florida: International Association of Nitrox Divers. pp. 279–286. ISBN 978-0-915539-10-9.
- staff. "Life Support Equipment Test Facility" (PDF). Retrieved 18 November 2016.
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||