Trimegestone
Trimegestone, sold under the brand names Ondeva and Totelle among others, is a progestin medication which is used in menopausal hormone therapy and in the prevention of postmenopausal osteoporosis.[4][2][3] It was also under development for use in birth control pills to prevent pregnancy, but ultimately was not marketed for this purpose.[5] The medication is available alone or in combination with an estrogen.[6][7] It is taken by mouth.[2]
 | |
| Clinical data | |
|---|---|
| Trade names | Ginotex, Lovelle, Minique, Ondeva, Totelle, others |
| Other names | TMG; RU-27987; 21(S)-Hydroxypromegestone; 21β-Hydroxypromegestone; 21(S)-Hydroxy-17α,21-dimethyl-9-dehydro-19-norprogesterone; 21(S)-Hydroxy-17α,21-dimethyl-19-norpregna-4,9-dien-3,20-dione; 17β-(S)-Lactoyl-17α-methylestra-4,9-dien-3-one; 17β-((S)-2-Hydroxypropanoyl)-17α-methylestra-4,9-dien-3-one |
| Routes of administration | By mouth |
| Drug class | Progestogen; Progestin |
| ATC code | |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability | 100%[1] |
| Protein binding | 98% (to albumin)[2] |
| Metabolism | Mainly hydroxylation[2] |
| Elimination half-life | Range: 12–20 hours[3] Mean: 13.8–15.6 hours[2][4] |
| Identifiers | |
| |
| CAS Number | |
| PubChem CID | |
| DrugBank | |
| ChemSpider | |
| UNII | |
| KEGG | |
| ChEBI | |
| ChEMBL | |
| ECHA InfoCard | 100.189.099 |
| Chemical and physical data | |
| Formula | C22H30O3 |
| Molar mass | 342.479 g·mol−1 |
| 3D model (JSmol) | |
| |
| |
Side effects of trimegestone include headache, breast tenderness, nervousness, abdominal pain, bloating, muscle cramps, nausea, depression, and vaginal bleeding among others.[8][4] Trimegestone is a progestin, or a synthetic progestogen, and hence is an agonist of the progesterone receptor, the biological target of progestogens like progesterone.[2][4] It has weak antiandrogenic and antimineralocorticoid activity and no other important hormonal activity.[2][4]
Trimegestone was first described in 1979 and was introduced for medical use in 2001.[9][10][11] It is sometimes described as a "fourth-generation" progestin.[12][13] The medication is marketed throughout Europe and Latin America.[14][6] It is not available in the United States or Canada.[15][14][6]
Medical uses
Trimegestone is used in menopausal hormone therapy in the treatment of menopausal symptoms such as hot flashes and vaginal atrophy and in the prevention of postmenopausal osteoporosis.[16][10][3][7]
Available forms
Trimegestone is available both alone (as Ondeva) and in combination with estradiol (as Ginotex, Lovelle, Minique, Totelle), both of which are approved for the treatment of menopausal symptoms and prevention of postmenopausal osteoporosis.[7][17] Preparations of trimegestone are oral tablets and contain 0.1 to 0.5 mg of the medication.[18]
Side effects
The most common side effects of trimegestone alone at dosages of 0.25 to 0.5 mg/day include breast tenderness (40.7–43.0%), abdominal pain (13.9–16.7%), headache (16.0–19.4%), nervousness (12.7–16.0%), bloating (10.3–16.0%), muscle cramps (12.3–13.9%), nausea (4.8–12.3%), and depression (3.0–3.1%).[8] The most common side effects of the combination of 1 mg/day estradiol and 0.125–0.25 mg/day trimegestone include headache (26.4%), breast pain (15–20%), abdominal pain (18%), and vaginal bleeding (9–18%), and metrorrhagia (18.8%).[4]
Pharmacology
Pharmacodynamics
Trimegestone is a progestogen, or an agonist of the progesterone receptor (PR).[19][2][20] It has very high affinity for the PR, about 588 to 660% of that of progesterone.[19][2][20] This is greater than that of almost all other widely used progestins, with the exception of the 19-nortestosterone derivative gestodene (which has about 864% of the affinity of progesterone).[19][21][2][20] In accordance with its very high affinity for the PR, trimegestone is described as a very potent progestogen, showing significant clinical effectiveness in the treatment of endometriosis at a dosage of only 0.1 mg/day, and is the most potent progestin of the 19-norprogesterone group.[16][2] Like other progestogens, trimegestone has functional antiestrogenic effects in certain tissues such as the endometrium and has antigonadotropic effects.[2][22] The endometrial transformation dosage of trimegestone is 0.25 to 0.5 mg/day and its ovulation-inhibiting dosage is 0.5 mg/day.[21][2]
In addition to its affinity for the PR, trimegestone has moderate affinity for the mineralocorticoid receptor (42–120% of that of aldosterone), weak to very weak affinity for the glucocorticoid and androgen receptors (9–13% of that of dexamethasone and 1–2.4% of that of testosterone, respectively), and no affinity for the estrogen receptor (less than 0.02% of that of estradiol).[19][2][20] In accordance, it possesses weak antimineralocorticoid activity, very weak antiandrogenic activity, and no androgenic, estrogenic, glucocorticoid, antiglucocorticoid, or mineralocorticoid activity.[2][19][4][20] As such, it is a selective and mostly pure progestogen.[16][2] Unlike progesterone, trimegestone does not metabolize into neurosteroids and hence does not influence GABAA receptor signaling or produce sedative side effects.[19]
The antiandrogenic potency of trimegestone in animals is about 30% of that of cyproterone acetate.[23]
Pharmacokinetics
The oral bioavailability of trimegestone is about 100%.[1][3] Following a single oral dose of trimegestone, peak serum concentrations occur within 0.5 hours and are 12–15 ng/mL (35–44 nmol/L) for a 0.5 mg dose and 25 ng/mL (73 nmol/L) for a 1 mg dose.[2][3] Circulating levels of trimegestone increase proportionally across dosages of 0.25 to 1 mg/day.[3] Steady-state levels of trimegestone are achieved within 3 days of daily administration.[3] The plasma protein binding of trimegestone is 98%; it is bound to albumin.[2] Trimegestone is metabolized mainly via hydroxylation.[2][22] The 1β- and 6β-hydroxy metabolites of trimegestone are progestogens with considerable potency similarly and show little or no affinity to other steroid hormone receptors.[22] The elimination half-life of trimegestone is between 12 and 20 hours, with an average of about 13.8 to 15.6 hours.[2][3][4]
Chemistry
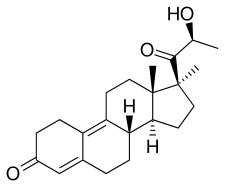
Trimegestone, also known as 21(S)-hydroxy-17α,21-dimethyl-δ9-19-norprogesterone or as 21(S)-hydroxy-17α,21-dimethyl-19-norpregna-4,9-dien-3,20-dione, is a synthetic norpregnane steroid and a derivative of progesterone.[24][2] It is specifically a combined derivative of 17α-methylprogesterone and 19-norprogesterone, or of 17α-methyl-19-norprogesterone.[24][2] Related derivatives of 17α-methyl-19-norprogesterone include demegestone and promegestone.[24][2]
History
Trimegestone was first described in 1979 and was introduced for medical use in 2001.[9][10][11] It was discovered as an active metabolite of promegestone.[9][21][25] The medication originated by Sanofi-Aventis in France, where promegestone was developed, and was first marketed by Wyeth in Sweden.[26]
Society and culture
Generic names
Trimegestone is the generic name of the drug and its INN, USAN, and BAN, while trimégestone is its DCF.[24][6][27] It is also known by its developmental code name RU-27987.[24][6][27]
Brand names
Trimegestone under the brand names Ginotex, Lovelle, Lovelle Ciclico, Lovelle Continuo, Minique, Ondeva, Totelle, Totelle Ciclico, Totelle Ciclo, Totelle Continuo, Totelle Cycle, Totelle Cyclo, Totelle Secuencial, and Totelle Sekvens.[14][6][27][11][3][28] With the exception of Ondeva, which is formulated alone, all of these products are formulated in combination with estradiol.[14][6][27]
Availability
Trimegestone is or has been marketed in Europe and Latin America, including in Argentina, Austria, Belgium, Brazil, Chile, Denmark, Finland, France, Italy, Lithuania, Mexico, Norway, Sweden, and Venezuela.[14][6][26][3][27] It is not available in any predominantly English-speaking countries, including the United States, Canada, the United Kingdom, Ireland, Australia, New Zealand, or South Africa.[15][14][6]
Research
The oral combination of trimegestone and ethinylestradiol was under development by Wyeth in the United States as a birth control pill to prevent pregnancy and the oral combination of trimegestone and conjugated estrogens was under development by Wyeth in the United States to treat menopausal syndrome and to prevent postmenopausal osteoporosis, but the development of both formulations was discontinued and they were never marketed.[5][29] A transdermal patch with the developmental code name PSK-3987 containing estradiol and trimegestone was under development by ProStrakan for the treatment of menopausal syndrome, but it too never completed development and hence was not marketed.[30]
References
- Howard J.A. Carp, MB, BS, FRCOG (9 April 2015). Progestogens in Obstetrics and Gynecology. Springer. pp. 38–. ISBN 978-3-319-14385-9.CS1 maint: multiple names: authors list (link)
- Kuhl H (2005). "Pharmacology of estrogens and progestogens: influence of different routes of administration" (PDF). Climacteric. 8 Suppl 1: 3–63. doi:10.1080/13697130500148875. PMID 16112947. S2CID 24616324.
- Stanczyk FZ (2002). "Pharmacokinetics and potency of progestins used for hormone replacement therapy and contraception". Rev Endocr Metab Disord. 3 (3): 211–24. doi:10.1023/A:1020072325818. PMID 12215716.
- Sitruk-Ware R, Bossemeyer R, Bouchard P (June 2007). "Preclinical and clinical properties of trimegestone: a potent and selective progestin". Gynecol. Endocrinol. 23 (6): 310–9. doi:10.1080/09513590701267727. PMID 17616854. S2CID 39422122.
- "Ethinylestradiol/trimegestone - Wyeth - AdisInsight".
- "Trimegestone".
- "Trimegestone - AdisInsight".
- Wahab M, Al-Azzawi F (September 2001). "Trimegestone: expanding therapeutic choices for the treatment of the menopause". Expert Opin Investig Drugs. 10 (9): 1737–44. doi:10.1517/13543784.10.9.1737. PMID 11772282. S2CID 20860088.
- M. Beato (1 January 1980). Steroid Induced Uterine Proteins: Proceedings of the International Symposium on Steroid Induced Uterine Proteins Held in Marburg, West Germany, 28-29 September, 1979. Elsevier/North-Holland Biomedical Press. pp. 227–228, 227–233. ISBN 9780444802033.
- Annual Reports in Medicinal Chemistry. Academic Press. 31 December 2012. pp. 273, 647. ISBN 978-0-12-397214-9.
- John Bodenhan Taylor; D. J. Triggle (2007). Comprehensive Medicinal Chemistry II: Global perspective. Elsevier. ISBN 978-0-08-044514-4.
- Sitruk-Ware R (2004). "New progestogens: a review of their effects in perimenopausal and postmenopausal women". Drugs Aging. 21 (13): 865–83. doi:10.2165/00002512-200421130-00004. PMID 15493951.
- Paula Briggs; Gabor Kovacs (11 July 2013). Contraception: A Casebook from Menarche to Menopause. Cambridge University Press. pp. 52–. ISBN 978-1-107-43611-4.
- "Micromedex Products: Please Login".
- Thomas L. Lemke; David A. Williams (24 January 2012). Foye's Principles of Medicinal Chemistry. Lippincott Williams & Wilkins. pp. 1403–. ISBN 978-1-60913-345-0.
- Eckhard Ottow; Hilmar Weinmann (8 September 2008). Nuclear Receptors as Drug Targets. John Wiley & Sons. pp. 208–. ISBN 978-3-527-62330-3.
- "Estradiol/trimegestone - AdisInsight".
- Martin Birkhauser; David Barlow; Morris Notelovitz; Margaret Rees (12 August 2005). Health Plan for the Adult Woman: Management Handbook. CRC Press. pp. 24–. ISBN 978-0-203-49009-9.
- Winneker RC, Bitran D, Zhang Z (2003). "The preclinical biology of a new potent and selective progestin: trimegestone". Steroids. 68 (10–13): 915–20. doi:10.1016/s0039-128x(03)00142-9. PMID 14667983.
- Philibert D, Bouchoux F, Degryse M, Lecaque D, Petit F, Gaillard M (October 1999). "The pharmacological profile of a novel norpregnance progestin (trimegestone)". Gynecol. Endocrinol. 13 (5): 316–26. doi:10.3109/09513599909167574. PMID 10599548.
- Schindler AE, Campagnoli C, Druckmann R, Huber J, Pasqualini JR, Schweppe KW, Thijssen JH (2008). "Classification and pharmacology of progestins". Maturitas. 61 (1–2): 171–80. doi:10.1016/j.maturitas.2008.11.013. PMID 19434889.
- Kuhl H (2011). "Pharmacology of progestogens" (PDF). Journal für Reproduktionsmedizin und Endokrinologie-Journal of Reproductive Medicine and Endocrinology. 8 (Special Issue 1): 157–176.
- Sitruk-Ware R, Husmann F, Thijssen JH, Skouby SO, Fruzzetti F, Hanker J, Huber J, Druckmann R (September 2004). "Role of progestins with partial antiandrogenic effects". Climacteric. 7 (3): 238–54. doi:10.1080/13697130400001307. PMID 15669548. S2CID 23112620.
- C.R. Ganellin; David J. Triggle (21 November 1996). Dictionary of Pharmacological Agents. CRC Press. pp. 2063–. ISBN 978-0-412-46630-4.
- Gerald Litwack (2 December 2012). Biochemical Actions of Hormones. Elsevier. pp. 314–. ISBN 978-0-323-15344-7.
- Annette M. Doherty (2002). Annual Reports in Medicinal Chemistry. Elsevier. pp. 273–. ISBN 978-0-12-040537-4.
- Sweetman, Sean C., ed. (2009). "Sex hormones and their modulators". Martindale: The Complete Drug Reference (36th ed.). London: Pharmaceutical Press. p. 2082. ISBN 978-0-85369-840-1.
- Bernardelli, Patrick; Gaudillière, Bernard; Vergne, Fabrice (2002). Chapter 26. To market, to market - 2001. Annual Reports in Medicinal Chemistry. 37. pp. 257–277. doi:10.1016/S0065-7743(02)37027-1. ISBN 9780120405374. ISSN 0065-7743.
- "Conjugated estrogens/trimegestone - Wyeth - AdisInsight".
- "Estradiol/trimegestone transdermal patch - ProStrakan - AdisInsight".
Further reading
- Wahab M, Al-Azzawi F (September 2001). "Trimegestone: expanding therapeutic choices for the treatment of the menopause". Expert Opin Investig Drugs. 10 (9): 1737–44. doi:10.1517/13543784.10.9.1737. PMID 11772282. S2CID 20860088.
- Winneker RC, Bitran D, Zhang Z (November 2003). "The preclinical biology of a new potent and selective progestin: trimegestone". Steroids. 68 (10–13): 915–20. doi:10.1016/S0039-128X(03)00142-9. PMID 14667983.
- Grubb G, Spielmann D, Pickar J, Constantine G (November 2003). "Clinical experience with trimegestone as a new progestin in HRT". Steroids. 68 (10–13): 921–6. doi:10.1016/j.steroids.2003.09.001. PMID 14667984. S2CID 40883746.
- Sitruk-Ware R, Bossemeyer R, Bouchard P (June 2007). "Preclinical and clinical properties of trimegestone: a potent and selective progestin". Gynecol. Endocrinol. 23 (6): 310–9. doi:10.1080/09513590701267727. PMID 17616854. S2CID 39422122.